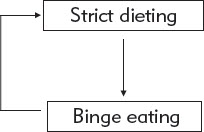
FIGURE 7. The vicious circle linking strict dieting and binge eating.
Sometimes a binge is just a binge. It is an isolated behavior that, even if recurrent, is not associated with other problems. More often than not, though, binge eating is associated with other difficulties. You may, in fact, be reading this book because of these difficulties rather than the binge eating. The relationship between these problems and the binge eating is complex, and often vicious circles develop that are self-maintaining and difficult to break.
The goal of this chapter and the next is to describe the many problems and concerns associated with binge eating and to examine their possible contribution to binge eating problems. This chapter focuses on problems that can be described as psychological or social; physical problems are examined in Chapter 5.
DIETING
Many people who binge also diet to an extreme degree, or at least attempt to do so, the exception being people with binge eating disorder. Sustained dieting punctuated by episodes of binge eating is the eating pattern seen in bulimia nervosa and those cases of anorexia nervosa in which there are binges. In some cases little or nothing is eaten outside the binges. In binge eating disorder the eating pattern is different. There is a tendency to overeat in general on top of which is superimposed the binge eating. People with binge eating disorder do diet at times: indeed, it is common for them to alternate between periods of successful dieting, which may last for months at a time, and periods of overeating when they also binge. As a result, their body weight may change markedly from month to month and year to year.
It is common for people with bulimia nervosa to make the mistake of thinking that their dieting is simply their response to binge eating. While dieting is undoubtedly encouraged by binge eating, especially among those who are highly concerned about their shape and weight, dieting plays an important role in causing binge eating. For example, binge eating is much more likely to occur on days in which the person is dieting. This is illustrated in Figure 7 which shows dieting both encouraging binge eating and being a response to it. Both these processes are powerful and together they result in binge eating persisting month after month, year after year. When tackling a binge eating problem it is therefore crucial to address not only the binge eating but also any contributory dieting.
FIGURE 7. The vicious circle linking strict dieting and binge eating.
Three Forms of Dieting
There are three main ways in which people diet. People who binge, and particularly those with bulimia nervosa or anorexia nervosa, tend to practice all three of them.
Delaying Eating. Some people eat barely anything between their binges. Indeed, they may not eat for days at a time (i.e., they fast). More commonly, though, they delay eating for as long as possible during the day, often not eating until the evening. About one in four people with bulimia nervosa does this, whereas it is much less common in binge eating disorder (about one in 20). Among the general population, only about one in 100 does not eat during the daytime.
Restricting the Overall Amount Eaten. Usually this involves trying to keep food intake below a certain calorie limit. For many people with bulimia nervosa the limit is 1,000 or 1,200 calories a day, well below the amount needed for normal day-to-day functioning. Some people set themselves even more extreme and inappropriate calorie limits, such as 800 or even 600 calories a day.
Avoiding Certain Types of Food. People who binge may avoid certain types of food because they perceive them as fattening or because eating them has triggered binges in the past. They often describe these foods as “forbidden,” “bad,” or “dangerous.” Research has shown that about one in five women in the general population diets in this way. In contrast, three-quarters of those with bulimia nervosa do so, as do half of those with binge eating disorder.
The range of foods avoided varies greatly. Among extreme dieters few foods—other than those manufactured and marketed as “diet foods”—are eaten freely. Figure 8 shows the “avoided food list” of a patient with bulimia nervosa.
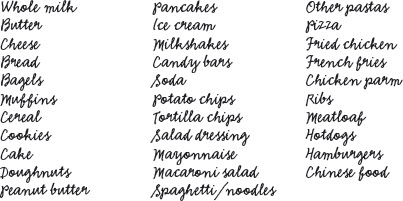
FIGURE 8. A list of foods avoided by someone with bulimia nervosa.
It is not uncommon for those who diet strictly to describe what they are doing as “healthy eating” or to justify their restrictive practices on the grounds that they are vegetarian or have a food allergy. Whatever way dieting is described, any dietary restriction that is intended at least in part to reduce weight or change shape should be viewed as dieting.
The Effects of Dieting
Food dominates my every waking minute. Even my dreams center on food.
Dieting has physical and psychological effects. The physical effects are described in Chapter 5. An important psychological effect is that the dieter becomes preoccupied with thoughts about food and eating and may also develop a sense of deprivation. Some dieters find themselves totally preoccupied with the very subject they are trying to avoid, unable to think about anything other than food and eating. They find it difficult to engage in everyday activities requiring concentration and even activities that demand minimal mental focus, such as watching television, may become impossible. No matter what they are doing, thoughts about food and eating keep intruding into their mind and even into their dreams. And as you may be aware if you have a friend or relative who is dieting, some also talk incessantly about food and eating. If you look at the figures in Table 2, you will see that preoccupation of this type is rare among young women in general, but as many as one in four of those with a binge eating problem is affected to a moderate or marked degree.
TABLE 2. Preoccupation with thoughts about food and eating among women with binge eating problems and women in the general population.
| Women in the community (%) | Women with binge eating disorder (%) | Women with bulimia nervosa (%) | |
| Little or none | 95 | 57 | 49 |
| Slight | 3 | 18 | 23 |
| Moderate | 2 | 21 | 13 |
| Marked | 0 | 4 | 15 |
Strict versus Ordinary Dieting
The three forms of dieting just described are all extreme; that is, the restrictions on how much, what, and when the person eats are marked. The dieting of some people who binge, particularly those with bulimia nervosa, also tends to be strict. Rather than having a general goal, these people have a very specific one, and if they do not achieve it they feel they have failed. Most dieters might want to keep their calorie intake below, say, 1,500 calories a day and are likely to be content if they achieve this goal on more days than not. In contrast, strict dieters feel that they must achieve this goal to the letter and that they have “failed” if they eat any more than their “rules” allow.
When dieting is both extreme and strict, involving highly specific dietary rules that demand considerable restraint, repeated “failures” are likely. This is demoralizing. But to make matters worse, these failures trigger binges because strict dieters are prone to abandon dieting, at least temporarily, when they break their rules, and the result is a binge. This reflects their thinking style, one that is characteristic of many of those who binge, so-called “all-or-nothing” or “dichotomous” thinking. People with this type of thinking see things in extreme, or black-or-white, terms; they see themselves as succeeding or failing; they view foods as good or bad; and so on. As a result, dieting characterized by multiple strict rules and accompanied by all-or-nothing thinking create a cycle of binge eating and dieting, with each promoting the other.
OTHER MEANS OF CONTROLLING SHAPE AND WEIGHT
Dieting is the most common weight control method practiced by those with binge eating problems. However, some utilize more extreme measures, including inducing vomiting and taking laxatives and diuretics. These forms of behavior are common in bulimia nervosa and anorexia nervosa and many atypical eating disorders but, by definition (as explained in Chapter 2), they are not present in binge eating disorder. Together, they are often referred to as “purging.”
Self-Induced Vomiting
I started vomiting after eating too much one day. It seemed a brilliant way to stay thin without dieting. I could eat as much as I wanted and then get rid of it. It would be so much easier than all that dieting.
I eat until I literally cannot eat any more. Then, using my fingers I make myself sick. Over the next half hour, drinking water between vomits, I purge all the food from my stomach. I then feel despondent, depressed, alone, and desperately scared because I have lost control again. I feel physically terrible: exhausted, puffy-eyed, dizzy, weak, and my throat hurts. I am also scared because I know it is dangerous. After a couple of sessions of vomiting when I actually brought up blood, I tried to stop. But I continued to binge, and the fear that built up was so great that I started making myself sick again.
It is not widely known that as many as 5 to 10% of young women admit to having made themselves vomit, and as many as 2% of young adult women vomit as often as once or more a week. “Epidemics” of self-induced vomiting sometimes occur, for example, in college dorms. Self-induced vomiting is especially common among people with bulimia nervosa, but it also occurs in up to half of those with anorexia nervosa. While most of these people vomit to get rid of food they have eaten—that is, in an effort to limit the number of calories absorbed—over time other motives may be acquired; for example, some people find that vomiting releases tension.
Self-induced vomiting is not necessarily evidence of an eating disorder (as defined in Chapter 2). The key issue is whether the vomiting and the other features of the eating problem interfere with physical health or quality of life. A particularly important matter is whether the person has control over the behavior. If someone chooses to vomit on occasions, however socially unorthodox it might be, the behavior is unlikely to be evidence of an eating disorder. But if the vomiting is frequent or cannot be resisted, it is almost certainly indicative of a significant eating problem.
I stop eating when I begin to feel ill. By then I have an overwhelming desire to rid myself of all the food I have eaten. I push my fingers down my throat and vomit again and again until I feel completely empty. This makes me feel relieved and cleansed. It also leaves me exhausted.
Usually self-induced vomiting is achieved by sticking an object down to the back of the throat to induce the gag reflex. After a while, however, some people can regurgitate at will by bending over and perhaps pressing on their stomach. There are others who cannot make themselves vomit, however hard they try.
Most people vomit after eating truly large amounts of food, but some people vomit after eating almost anything, particularly if they view it as fattening. Some people vomit just once after eating, and this rids them of sufficient food to relieve their anxiety over what they have eaten. Others vomit again and again until they cannot bring up anything more. This process can take an hour or more, and may leave them physically drained. A minority practice a flushing technique: They drink something, then vomit, drink again and vomit, drink again, and so on, repeating this process until the liquid comes back clear of any food. Only at this point do they feel confident that they have retrieved everything that they can. This practice is physically hazardous as it can result in electrolyte disturbance (see “Fluid and Electrolyte Imbalance”).
The belief that vomiting is an effective means of getting rid of food is a mistaken one. While it clearly removes some of the food, laboratory studies have shown that it retrieves only about half the calories consumed. For example, one study found that while volunteers’ binges averaged 2,131 calories, their vomit only comprised 979 calories. The relative ineffectiveness of vomiting explains why most people with bulimia nervosa are a normal weight. It is because they are living off the residue of each of their binges, the 50% they cannot retrieve. And remember the average binge contains between 1,000 and 2,000 calories (see “The Size of Binges”).
Some people say that they know that they bring almost everything up when they vomit. This is usually because they eat a “marker” food (such as tomatoes) at the beginning of each binge and they repeatedly vomit until this food (i.e., the tomato skins) reappears. They are acting on the erroneous (geological) assumption that food is deposited in the stomach in layers. In fact, the stomach contents are churned around, so the reappearance of the marker food does not indicate that the stomach has been emptied of everything that has been eaten.
I first started vomiting as a way of eating what I liked, without feeling guilty and without putting on weight. Vomiting was surprisingly easy and I was pretty pleased with myself. It was only later that I realized what a problem it had become.
Over the past 8 years I have repeatedly said to myself: “This is going to be the last time that I throw up.” At first I was not that bothered: I thought I could control it if I chose to. But it soon became clear that it had control over me. Now stopping seems completely beyond my reach.
If you take a long-term perspective, self-induced vomiting becomes even less attractive as a means of weight control. People who induce vomiting often describe the delight that they experienced when they first made themselves sick. Here was the answer to their problems: instead of struggling to control their urges to eat, they could give in yet not gain weight. In practice, they pay a heavy price because vomiting encourages overeating. This is the result of two mechanisms. First, since people believe that by vomiting they will avoid absorbing most of what they have eaten, their attempts to resist eating are undermined and as a result they tend to become more prone to binge, and furthermore their binges become larger in size. They also find that it is easier to vomit if their stomach is full. As a result of these processes a further vicious circle becomes established with vomiting being both a response to binge eating and a behavior that encourages it (see Figure 9). Indeed, vomiting can become one of the main processes that maintains binge eating. This is illustrated by the fact that many people who vomit are able to resist binge eating—which would otherwise be outside their control—if they know that there will be no opportunity to vomit.
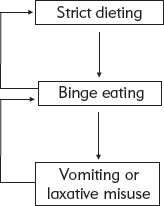
FIGURE 9. The vicious circles linking strict dieting, binge eating, and vomiting.
The one other point to stress is an obvious one. Vomiting has harmful physical effects. These are described in Chapter 5. Table 3 summarizes the key facts about self-induced vomiting.
TABLE 3. Four key facts about self-induced vomiting.
1. Vomiting is inefficient. It only retrieves about half the calories eaten in a typical binge.
2. Vomiting encourages overeating: people become more prone to binge and their binges become larger.
3. Vomiting maintains binge eating.
4. Vomiting has harmful physical effects.
Laxative and Diuretic Misuse
I started taking laxatives because I was scared that because I was eating so much I would get fat really quickly. I thought that if I took laxatives all the food would go straight through me.
I read in a magazine about people using laxatives as a way of purging themselves. I’d tried vomiting but couldn’t do it. So I went out and bought some laxatives and downed 10 after every binge. I knew deep down that they didn’t really do anything to counteract the binge, but they made me feel empty and cleansed inside.
The use of laxatives or diuretics (water pills) to control weight is less common than the use of self-induced vomiting. Laxatives are taken by about a third of those with bulimia nervosa and diuretics by about 10% (see Table 4). Both may occur in isolation or in combination with self-induced vomiting. By definition, all three forms of behavior are uncommon among those with binge eating disorder, although they do occur in anorexia nervosa and some atypical eating disorders.
TABLE 4. Common methods of weight control (besides dieting) in people with bulimia nervosa.
| Community sample (%) | Clinic sample (%) | |
| Self-induced vomiting | 54 | 76 |
| Laxative misuse | 35 | 38 |
| Both vomiting and laxative misuse | 19 | 23 |
| Diuretic misuse | 10 | 12 |
People with binge eating problems misuse laxatives in two ways. They take them either to compensate for specific episodes of overeating, in which case the behavior is very similar to self-induced vomiting and the numbers taken may be very large, or they take them on a regular basis, independent of particular episodes of overeating, in which case the number taken is smaller and the behavior is more like dieting. Diuretics tend to be taken in the latter way.
Laxatives have little effect on calorie absorption because most food is absorbed high up in the intestine whereas laxatives act lower down. Diuretics have no effect on calorie absorption: they are merely dehydrating. Nevertheless some people find the use of these drugs rewarding, mainly because weight drops, albeit transitorily, due to the fluid lost in the diarrhea or excess urine. (In Chapter 5, I discuss hydration and its importance in relation to body weight.) In addition, some people find that taking laxatives gives them a sense of having rid themselves, or “cleansed” themselves, of the food that they have eaten. In this way laxatives, like self-induced vomiting, can encourage further binge eating. Many people also describe liking the feeling that their abdomen is empty after taking laxatives, and some particularly value the flat appearance that may temporarily result. A minority welcome the unpleasant physical effects. They view the abdominal cramps and spasms, and the associated diarrhea, as just punishment for having overeaten.
The physical effects of laxative and diuretic misuse are described in Chapter 5.
Diet Pills
Diet pills, typically appetite suppressants, are also misused by some of those with eating disorders. This is despite the fact that these drugs only have a modest effect on body weight.
Extreme Exercising
Some people who binge exercise a lot, in large part to influence their shape or weight. This is not usually a problem unless it starts to take over their life. If it begins to take precedence over other important activities, such as eating, sleeping, or socializing, it is of greater concern.
A subset of people develop driven or “compulsive” exercising. This is characterized by difficulty resisting exercising, even when the costs far outweigh the benefits, and it is most often seen in anorexia nervosa. In these people “overuse injuries” may occur.
Another exercise-related phenomenon is “debting.” This is when eating and exercising become linked in such a way that the people will not eat unless they have burned off the requisite number of calories beforehand. It tends to coexist with extreme exercising and, although unusual, it is seen in all the eating disorders other than binge eating disorder.
At the other end of the spectrum, exercising too little is more characteristic of people with obesity including those with binge eating disorder. This contributes both to their obesity and to its associated health risks.
Manipulation of Fluid Intake
It is not uncommon for people who binge to manipulate their fluid intake as a means of controlling their eating or weight. Among the behaviors seen are the following:
• Drinking large quantities of fluid in order to curb appetite and feel full.
• Drinking large quantities of fluid to facilitate vomiting.
• “Flushing”—after binge eating, repeated drinking followed by vomiting until the liquid comes back clear of any food.
• Minimizing fluid intake in order to dehydrate (and lose weight).
All of these behaviors can disturb the body’s level of hydration and electrolyte levels too (as we shall discuss in Chapter 5, “Fluid and Electrolyte Imbalance”).
PHYSICAL AND PSYCHOLOGICAL EFFECTS OF BEING UNDERWEIGHT
Some people with binge eating problems are unambiguously underweight, even if they do not view themselves this way. Anyone with a BMI of 18.5 or below is underweight medically speaking (see Chapter 2) and is at risk of adverse physical, psychological, and social effects. These markedly increase once the BMI falls below 17.5.
Knowledge about the consequences of a low body weight has come from a variety of sources. These include studies of the effects of famines and experimental studies in which volunteers have adhered to a restricted diet for extended periods of time, the most famous being the Minnesota Semi-Starvation Study (see Box 5). Consistent findings have emerged from these studies and they are summarized below. If you are underweight and have an eating disorder you will experience the same effects, some of which are due to being underweight whereas others are direct effects of undereating. Almost all these effects are reversed by gaining weight to a healthy level and eating well.
BOX 5. The Minnesota semi-starvation study.
A seminal study of the effects of being underweight was conducted in the 1940s by Ancel Keys of the University of Minnesota. In this study 36 conscientious objectors (all male) were observed and assessed while their food intake was decreased to the point where their weight dropped to 75% of their prestarvation weight. The selection criteria for the men were strict: only the most socially and physically healthy volunteers were allowed to take part. Despite this, during the starvation period it was noticed that the once gregarious men became inward looking; they lost interest in socializing and other activities; and they became much more irritable, often provoking fights with each other. The men began to focus their lives around food and eating, paying little attention to anything else. This is very like what is seen in anorexia nervosa.
Source: Keys, A., Brozek, J., Henschel, A., Mickelsen, O., & Taylor, H. L. (1950). The biology of human starvation (2 vols.). Minneapolis: University of Minnesota Press.
Psychological Effects
Thinking. The brain is affected by both undereating and being underweight. It is therefore hardly surprising that thinking is impaired. It becomes somewhat inflexible, with there being difficulty switching from topic to topic. Decision making is also affected, and this often results in procrastination.
Concentration is almost always impaired although some people are unaware of this since they force themselves to focus on what they are doing. The concentration impairment is worsened by the presence of intrusive thoughts about food and eating.
The almost constant thinking about food and eating has secondary effects. It leads some people to become particularly interested in cooking and thus they selectively read recipes and watch TV cooking shows. They may also do a lot of cooking themselves. They may even take up careers that involve food and eating. A consequence of this focus on food and eating is that they become less interested in other things—for example, they may abandon prior interests and hobbies.
Emotions. Mood is affected by being underweight. It is generally somewhat low and many people are prone to get irritated rather easily.
Behavior. There are also remarkably consistent changes in behavior. One of the most prominent behavioral changes is heightened “obsessiveness.” This term refers to the tendency to be inflexible and rigid in one’s routines, and it is often accompanied by difficulty being spontaneous. The obsessiveness is particularly striking when it comes to eating, which may become a mini “ceremony” that has to be conducted alone. Some people eat very slowly, chewing each mouthful a certain number of times; others eat in a ritualized way, such as always eating from a certain plate or cutting food into small pieces. Hoarding objects is yet another sign of the obsessiveness although not everyone shows it. The hoarding may be of food or other things. Often people cannot explain why they are hoarding.
Social Effects
Being underweight has a profound effect on social functioning. There is a tendency to become inward-looking and self-focused. This is exaggerated by the heightened need for routine and predictability, and the difficulty being spontaneous. As a result people often withdraw socially and get used to this way of living.
These psychological and social characteristics are often mistaken as the person’s personality whereas their true personality is being masked by the effects on the brain of being underweight.
CONCERNS ABOUT SHAPE AND WEIGHT
My confidence and feelings of self-worth are deeply rooted in the idea that I must be physically attractive, i.e., thin. When I put on weight, even 1 pound, I risk being unattractive, and I see my future as bleak and lonely. This thought fills me with despair, so I force myself to eat as little as possible.
Most people who binge are extremely concerned about their shape and weight. Indeed, these concerns may be so intense that their life becomes dominated by them; nothing else much matters. This “overconcern” is characteristic of most forms of eating disorder: indeed, many experts view it as the “core” feature as everything else seems to stem from it. The overconcern is most prominent in bulimia nervosa and anorexia nervosa and many atypical eating disorders (see Chapter 2). It is less prominent in people with binge eating disorder. Their concerns tend to have a different quality. They are better described as dissatisfaction and they are somewhat more understandable in view of these people’s higher weight. Nevertheless, they can be a problem. For example, some people with binge eating disorder go to great lengths to prevent others from seeing their body, and they may also avoid seeing it themselves. Some even view their appearance with disgust and loathing.
What does overconcern about shape and weight mean? Think for a moment about how you evaluate yourself as a person. Whereas the majority of people evaluate themselves on the basis of how they are performing in a variety of areas of their life (such as the quality of their relationships, their performance at work, their athletic accomplishments, etc.), most people with an eating problem judge their self-worth largely, or even exclusively, in terms of their shape and weight and their ability to control them. This can be represented diagrammatically in the form of a pie chart in which each slice represents an area of life that is valued; the bigger the slice the more important that area is to the person concerned. Figures 10 and 11 show two such pie charts, one of a young woman with no eating problem and the other of someone with overconcern about shape and weight.
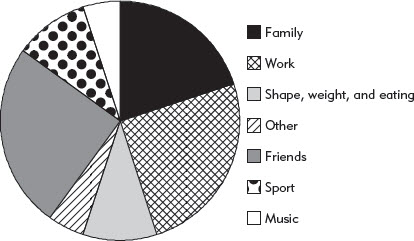
FIGURE 10. The pie chart of a young woman without an eating problem.
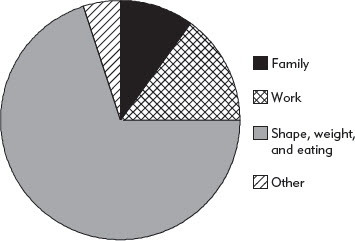
FIGURE 11. The pie chart of a young woman with an eating problem.
The overconcern about shape and weight seen in bulimia nervosa, anorexia nervosa, and many atypical eating disorders is of great importance in understanding these problems. It is central to their persistence—it is the “engine” that drives these problems. It accounts for the strict dieting (and therefore any binge eating), the vomiting, the misuse of laxatives and diuretics, and excessive exercising. It also accounts for a range of other phenomena that we are about to discuss. And, understandably, the over-concern is maintained by any tendency to binge eat, creating a further vicious circle (see Figure 12). Reducing the intensity of these concerns is therefore a major goal of treatment. Guidelines for doing this are provided in Part II.
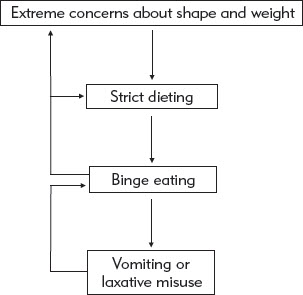
FIGURE 12. The central role of concerns about shape and weight.
Weight Checking and Weight Avoidance
I am obsessed with my weight. I weigh myself over and over again, sometimes up to 15 times a day. At other times I am so disgusted with my body that I don’t use the scales for weeks or months at a time.
The most direct “expression” of overconcern about weight and shape is body checking. This may involve weight checking, shape checking, or both.
Many people with binge eating problems weigh themselves at frequent intervals, sometimes many times a day. For example, over a quarter of those with bulimia nervosa weigh themselves at least once a day, compared to only one in 20 women in the community (see Figure 13). As a result many become concerned about day-to-day weight fluctuations that would otherwise pass unnoticed. This leads them to restrict their eating, whatever the number on the scales: if it is “up” or “the same,” they try to diet even harder; and if it is “down,” their dieting is reinforced. Whatever the number, they tend to conclude that they must continue to diet. This is yet another process that maintains binge eating problems. What is often not appreciated is that day-to-day weight changes are not indicative of changes in body fat. They are much more likely to be due to changes in hydration, as explained in Chapter 5.
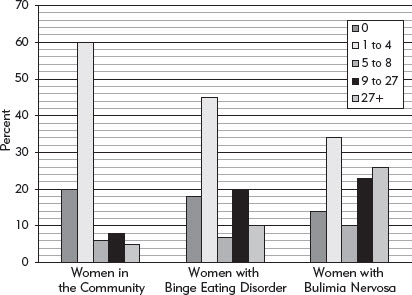
FIGURE 13. How often people weigh themselves (times per 28 days).
Other people with binge eating problems actively avoid knowing their weight while remaining highly concerned about it. Generally these people used to weigh themselves frequently but switched to avoidance as they found frequent weighing too aversive. Unfortunately, avoidance of weighing is as problematic as frequent weighing because it results in fears and assumptions about weight remaining unchallenged.
Shape Checking
I am confident in many ways, yet I hate my body and can’t bear to look at it. I feel bloated, wobbly, and huge all over. This drives me to binge. My boyfriend loves me. Why can’t I like myself?
Immediately I wake up I feel my hips and stomach to check that they’re not covered in a layer of fat.
Shape checking is another form of body checking. Of course, everyone checks their body to some extent but many people with a binge eating problem check their body repeatedly and in ways that are unusual. They may study themselves in the mirror, measure themselves, and even take repeated photographs of themselves when unclothed. In addition, they may assess the tightness of set items of clothing or accessories (e.g., watches or rings), and they may look down at themselves when sitting to assess how much their stomach bulges out or to what extent their thighs splay. If you are male you may be concerned about your build and muscularity (or lack of it) and focus your checking on this. Such shape checking can become so “second nature” that you may not be fully aware that you are doing it; for example, when taking a shower many people are also inadvertently shape checking by feeling their bones and pinching their flesh.
Mirrors can be a particular problem. Studying yourself in the mirror is a particular form of shape checking that has the potential to provide highly credible, but misleading, information. We all believe what we see in the mirror, yet assessing oneself in a mirror is far more complex than is generally realized. To illustrate this point, consider the size of your image when you look at yourself in a full-length mirror. Is the image that you see on the surface of the mirror the same height as your true height? If not, what height is it? And what about the width of the image? To find out the answer, ask a friend to mark on the mirror surface the top and bottom of your reflection as you see it (when you are standing sufficiently far away so that you can see your head and feet) and then measure how far apart they are. You will find that your image on the mirror surface is about half your size in all dimensions, something that you have probably not noticed before. The fact that you have not realized that you have been looking at a very small version of yourself over all these years should help to persuade you that mirrors are complex and that a lot of mental processing goes on “behind the scenes” when you look into the mirror.
There are three points to emphasize about shape checking. First, it generally involves the studying of aspects of appearance that are disliked. This is bound to maintain body dissatisfaction. Second, when checking, what you discover depends to a large extent upon the way that you assess yourself. If people look at themselves in detail, “flaws” that would normally go unnoticed become prominent and, once noticed, they are hard to forget. Even really attractive people would find flaws if they studied themselves. And third, scrutiny is prone to magnify apparent defects. This is illustrated by a phenomenon seen among people with spider phobias. They tend to see spiders as larger than they really are. This is because when looking at spiders they focus down on them and their unpleasant characteristics while not looking at the surrounding environment. As a result they get detailed information about the spider in the absence of any reference points for size. An equivalent phenomenon happens to people who study themselves in the mirror because scrutinizing aspects of one’s body is prone to magnify them. If you look for fatness, you will find it: indeed, you will create it.
Comparison Making
Comparison making is a particular form of shape checking. Some people with binge eating problems do this repeatedly and usually in a way that makes them conclude that they are unattractive relative to others. This is because they make a superficial assessment of the other person while critically scrutinizing themselves. Furthermore, they tend to compare themselves with people who are thin and goodlooking: they fail to notice those who are less thin and attractive.
It is also common for people with eating problems to compare themselves with photographs in magazines and on the Internet without taking into account that these images have often been manipulated. As we discuss in Part II, it is important to become street-wise in this regard (see Addressing Shape Avoidance).
Shape Avoidance
I cannot put into words how repulsed I am with my body. I cannot bear to look at it. I will have no mirrors in the house. I take showers instead of baths to avoid having to look at myself. I have not gone shopping for clothes for more than 3 years.
I can never shower with the lights on. If I do, I will see all my fat.
Shape avoidance is the counterpart to shape checking. The term refers to behavior designed to prevent the person from seeing his or her body and being aware of it. It often includes avoidance of others seeing their body too. It stems from a strong dislike of how their body looks or feels. Often people with shape avoidance used to engage in shape checking but switched to avoidance because the checking became too distressing.
Shape avoidance takes various forms: it can involve avoiding looking in the mirror, not wearing tight clothes, covering the stomach (e.g., with the arms), and not looking at photographs. It is as problematic as it is distressing and it allows concerns about shape to persist unquestioned.
When extreme, shape avoidance can profoundly interfere with day-to-day life. At the mild end it affects clothes choice, the ability to go swimming, and changing in public. At the more severe end, the person may be unable to have a sex life or any form of physical intimacy due to his or her dislike of being touched or seen. Telling these people that they look fine is rarely reassuring as most are impervious to comments of this type or they interpret them negatively.
Occasionally shape checking and avoidance coexist. When this occurs the person checks some aspects of his or her body while avoiding others, or switches from checking to avoidance and back.
Feeling Fat
Feeling fat is another product of concerns about shape and weight. Of course, feeling fat is an experience reported by many women, and some men, but its intensity and frequency is far greater among people with eating problems. It is an important phenomenon because it can be equated with actually being “fat,” and when this occurs it tends to encourage dieting.
Feeling fat is ill-understood: indeed, remarkably little has been written about it. What is noteworthy is that the experience fluctuates markedly in intensity from day to day and even within a day. This is quite unlike overconcern with shape and weight, which tends to be stable, as are one’s actual shape and weight.
Feeling fat is usually the result of mislabeling unpleasant emotions and bodily experiences. These include feeling depressed, lonely, or unloved; or feeling bloated, premenstrual, or hungover. Why this mislabeling occurs is not clear but it could be a consequence of the long-standing and profound preoccupation with thoughts about shape.
When feeling fat is frequent, intense, or distressing, it needs to be tackled in treatment. Doing so is one element of the self-help program in Part II.
OTHER PSYCHOLOGICAL AND SOCIAL PROBLEMS
My eating problem has taken over my whole life. My friendships have been upset by my violent swings in mood. I never talk to my parents since they have never understood what I am going through, yet we were so close. I have so little self-confidence. I get terribly depressed and anxious. I can’t face seeing people.
My life revolves around my eating. I can no longer concentrate on my work, which has suffered as a result. My problem has caused family rows [arguments]. I no longer enjoy sharing meals with family or friends. I have become withdrawn and introspective and have lost all self-confidence and self-respect. I don’t want to go out. I don’t like myself anymore.
I am late for everything because eating takes so much time . . . and not just the eating part but the buying of food, getting rid of the packages, cleaning up, etc, etc.
As you will be aware if you have a binge eating problem, your quality of life suffers. You may feel depressed and demoralized. Many people are ashamed of their lack of willpower and feel guilty about their secrecy and deceit. They are highly self-critical. Some get so desperate that they attempt to take their life. Others repeatedly harm themselves, often by cutting their skin. This can be to punish themselves, to relieve tension, or both. Irritability is also common.
The feelings of depression can be severe. Generally they are secondary to the binge eating problem and when this is the case they resolve once the person regains control over his or her eating. However, in a subgroup, a true clinical depression develops. Features that suggest that this has happened include a sustained lowering of mood, loss of psychological drive, thoughts about death and dying, uncharacteristic tearfulness, and social withdrawal. If you have some or all of these features then it is important to seek professional advice as depression is serious yet eminently treatable.
Those who binge are also prone to be anxious, both as a character trait and, most especially, when in situations that activate their concerns. For example, some avoid social occasions, particularly those that involve eating. This might mean missing the wedding of a close friend or the birthday party of a parent—all of which hurt both the person with the eating problem and his or her friends or family. Events and circumstances that involve some degree of body exposure are also often avoided. These include swimming, parties, and beach vacations.
Nor is excessive drinking uncommon. This may take the form of habitual overconsumption or intermittent binge drinking. The latter is typically triggered by adverse events or moods, much like binge eating. A small minority misuses psychoactive drugs.
Two character traits are prominent among people with binge eating problems. The first is low self-esteem. Feelings of inadequacy and worthlessness are common. While they are often part of any accompanying demoralization or depression, and so improve as the eating problem resolves, they can also be the expression of a long-standing personality trait. Some people describe such feelings as stretching back into their childhoods.
The other common character trait is perfectionism. Many people who binge tend to set unduly demanding standards for themselves. Their perfectionism tends to affect most aspects of their life, but it is particularly obvious in the dietary goals that they set for themselves. The trait does, of course, have its positive side as perfectionists may perform exceptionally well at work and in other aspects of life that they value. The key issue is whether their standards are realistic. If they are, there is no problem. However, if they are not, they will experience repeated “failures” even when their performance is high by most people’s standards. Failing in this way can be undermining, especially if self-esteem is low. Indeed, the combination of low self-esteem and perfectionism is not unusual among those who binge, and especially those with bulimia nervosa, anorexia nervosa, or an atypical eating disorder (see Chapter 2), and it may well contribute to the development of the problem (see Chapter 6).
At their worst, binge eating problems affect every aspect of life. Nothing is spared. So much time and effort is taken up by the problem that little is left for anything else. Relationships with family and friends may even become unsustainable. As with the feelings of depression most interpersonal problems improve markedly, if not go away altogether, once the binge eating problem recedes. One of the most gratifying aspects of helping people overcome binge eating problems is seeing the person underneath gradually emerge as the problem goes away. The depression, tension, and irritability fade; relationships improve; and old interests return.