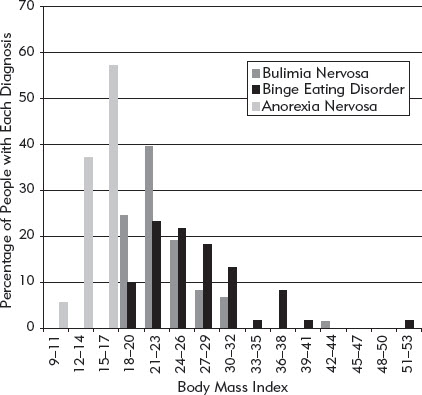
FIGURE 3. The weight distribution of people with bulimia nervosa, anorexia nervosa, and binge eating disorder shown in terms of their body mass index (see Box 3). Data kindly provided by Dr. Riccardo Dalle Grave.
Few people have not heard of bulimia nervosa and the “dieter’s disease” anorexia nervosa. Unfortunately the publicity that these disorders have attracted has resulted in them being trivialized; for example, the term anorexic is now synonymous with being underweight. One of the goals of this chapter is to clarify what these terms actually mean, while also explaining how binge eating problems are classified.
EATING PROBLEMS VERSUS EATING DISORDERS
The great majority of people who binge do not have an “eating disorder.” Their binge eating is occasional rather than frequent, it does them no physical harm, and it does not impair their quality of life. If, however, they view their binge eating as a “problem,” then that is exactly what it is, an “eating problem.” On the other hand, there are significant numbers of people whose binge eating does interfere with their physical health or quality of life. These people are viewed as having an eating disorder.
In adults and teenagers three eating disorders are distinguished:
• Bulimia nervosa
• Anorexia nervosa
• Binge eating disorder
This is not the complete picture, however. Clinical and community-based studies indicate that it is not uncommon for people to have an eating disorder that falls outside these three categories. These people may be viewed as having an “atypical eating disorder.”
BULIMIA NERVOSA
Bulimia nervosa, originally known in North America as “bulimia,” has come to attention only in the last 30 or so years. Box 2 lists the major milestones in the history of this “new” eating disorder.
BOX 2. A brief history of bulimia nervosa.
1976—Reports of “bulimarexia” among American college students (see Chapter 3).
1979—Publication of Professor Gerald Russell’s classic paper “Bulimia nervosa: An ominous variant of anorexia nervosa.” This paper introduced the term bulimia nervosa.
1980—Syndrome of “bulimia” added to the American Psychiatric Association’s diagnostic manual.
1980–1982—Studies in Great Britain and North America indicate that bulimia nervosa is likely to be common (see Chapter 3).
1981–1982—Reports describe two promising treatments for bulimia nervosa: cognitive behavior therapy and antidepressant medication (see Chapter 8).
1987—Bulimia redefined and renamed bulimia nervosa by the American Psychiatric Association, bringing the concept more in line with Russell’s one.
2013—Diagnostic criteria of the American Psychiatric Association broadened to include cases in which the binge eating occurs once a week. Previously the lower limit was twice weekly.
In principle, three features have to be present to make the diagnosis bulimia nervosa, and one feature has to be absent. These features are as follows:
1. The person must have frequent objective binges; that is, he or she must have recurrent episodes of eating during which he or she eats genuinely large amounts of food—taking into account the circumstances—with there being a sense of loss of control at the time. By definition, all people with bulimia nervosa binge eat.
2. The person must engage in one or more extreme methods of weight control. These include self-induced vomiting, the misuse of laxatives or diuretics, intensive exercising, and extreme dieting or fasting.
3. The person must show “overevaluation” of the importance of his or her shape or weight, or both; that is, people with bulimia nervosa should judge themselves largely, or even exclusively, in terms of their ability to control their shape or weight. (This feature is described in detail in “Concerns about Shape and Weight” in Chapter 4.) Their concern about shape and weight goes far beyond just feeling fat or being unhappy with their appearance.
4. The person does not currently have anorexia nervosa (defined shortly). In effect this means that the person cannot be significantly underweight. In practice the great majority of those with the three defining features of bulimia nervosa have a body weight in the healthy range. Figure 3 shows the weight distribution of people with bulimia nervosa, anorexia nervosa, and binge eating disorder.
FIGURE 3. The weight distribution of people with bulimia nervosa, anorexia nervosa, and binge eating disorder shown in terms of their body mass index (see Box 3). Data kindly provided by Dr. Riccardo Dalle Grave.
As explained in Chapter 3, bulimia nervosa is largely confined to women, with the majority being in their 20s. The proportion of cases that are male is uncertain—it is likely to be less than one in 10. The problem usually starts in the late teenage years with a period of strict dieting that eventually becomes punctuated by repeated episodes of binge eating. In about a quarter of cases the dieting is so extreme that the person first develops anorexia nervosa and then progresses to bulimia nervosa.
People with bulimia nervosa have chaotic eating habits. All have objective binges, but these binges occur against the background of extreme attempts to restrict eating—indeed, the person’s eating outside their binges closely resembles that of people with anorexia nervosa. Some eat virtually nothing outside their binges, and most of the others diet strictly. Many make themselves vomit after each binge in order to get rid of the food they have eaten. Laxatives, diuretics, and diet pills may also be used for this purpose, as may intense exercising.
Once established, bulimia nervosa tends to be self-perpetuating. It has little tendency to remit spontaneously, although it can wax and wane in severity. By the time people seek help, if indeed they do, most have eaten in this way for 5 to 10 years or even longer.
ANOREXIA NERVOSA
Most people have heard of anorexia nervosa, perhaps because of the media attention it attracts, either because it can be fatal or because the sufferers look so unwell. Two main conditions must be met for someone to be said to have this eating disorder:
1. The person should be significantly underweight, and this should be the result of his or her own efforts. The threshold for viewing someone as significantly underweight is debated and varies—a body mass index (BMI) below 17.5, 18.0, or 18.5 are widely used figures. (Box 3 describes the BMI.)
2. The person should show evidence of the overevaluation of the importance of shape and weight, as in bulimia nervosa. Rather than worrying about being underweight, people with anorexia nervosa are terrified of gaining weight and becoming fat. Indeed, many regard themselves as already being “fat” despite their low weight. For this reason they are sometimes said to have a “morbid fear of fatness” or a “weight phobia,’’ and their dieting has been described as being driven by a “relentless pursuit of thinness.”
BOX 3. The body mass index (BMI).
The body mass index (BMI) is a useful way of determining whether you are underweight, normal weight, or overweight. It is your weight adjusted for your height. Specifically it is weight in kilograms divided by height in meters squared (i.e., weight/[height × height]). The BMI applies to all adults of both sexes between the ages of 18 and 60. Appendix II provides a chart for identifying your BMI.
Below are the BMI thresholds used to classify people as underweight, as having a healthy weight, as overweight, or as having obesity. Note that they are based on health risks, not appearance.
| Underweight | Below 18.5 |
| Healthy weight | 18.5 to 24.9 |
| Overweight | 25.0 to 29.9 |
| Obese | 30.0 and above |
There is good evidence that people of Asian origin have greater health risks at lower BMIs than Caucasians. For this reason, the World Health Organization has considered lowering the BMI thresholds for overweight and obesity for Asian people.
It is also important to bear in mind that there are some limitations of the BMI. It does not apply to children below 18, adults above 60, people with a large muscle mass (e.g., many athletes), or those with physical illnesses.
Anorexia nervosa mainly affects teenage girls and young women, but about one in 10 cases occurs in men. People with the disorder achieve their low weight by eating very little, although excessive exercising may also contribute. They avoid eating foods they view as fattening, and they may fast at times. About a third have “binges,” most of which are small in size (i.e., they are subjective binges), during which their attempts to restrict their food intake break down. For people with anorexia nervosa a binge may consist simply of a few cookies.
I had been anorexic for about a year and was attempting to start eating properly. One day, out of the blue, I ate a chocolate cookie. Suddenly I began eating all those things I’d deprived myself of. It wasn’t a large binge by my current standards, but it was more calories than I normally ate in a whole week. I came out of my trance-like state and was suddenly terrified about what I had done. I immediately went to the bathroom and stuck my fingers down my throat. I had to throw up and get rid of all the garbage inside me.
Anorexia nervosa may be short-lived with the person making a complete recovery with or without treatment. This is most typical of cases in their teens. Alternatively, it may evolve into bulimia nervosa or an atypical eating disorder (see below). A small proportion of sufferers get “stuck” in anorexia nervosa, an extremely serious state from which it can be hard to escape.
BINGE EATING DISORDER
As the term implies, binge eating is the main feature of binge eating disorder. The diagnosis is a recent one, although its origins go back to the late 1950s when Albert Stunkard of the University of Pennsylvania noted that some people with obesity have significant problems with binge eating. This observation was largely ignored or forgotten until the mid-to-late 1980s when evidence began to mount that about a quarter of those who seek treatment for obesity report binge eating, yet few meet the criteria for bulimia nervosa. About the same time, community studies of the prevalence of bulimia nervosa showed that the majority of those who binge eat do not have bulimia nervosa. Together, these findings led to the proposal that a new eating disorder be recognized characterized by recurrent binge eating in the absence of extreme methods of weight control. This disorder is now termed binge eating disorder. Prior to this, such people had been described, somewhat pejoratively, as “compulsive eaters.”
People with binge eating disorder have repeated objective binges, but they do not engage in the extreme weight control measures used by people with bulimia nervosa. Thus they do not vomit; they do not take laxatives, diuretics, or diet pills; they do not overexercise; and they do not diet to an extreme degree. Instead, their eating is typically characterized by a general tendency to overeat upon which binge eating is superimposed. This is illustrated in the eating record shown in Figure 4. Hardly surprisingly, therefore, many people with binge eating disorder are overweight or have frank obesity (as shown in Figure 3).
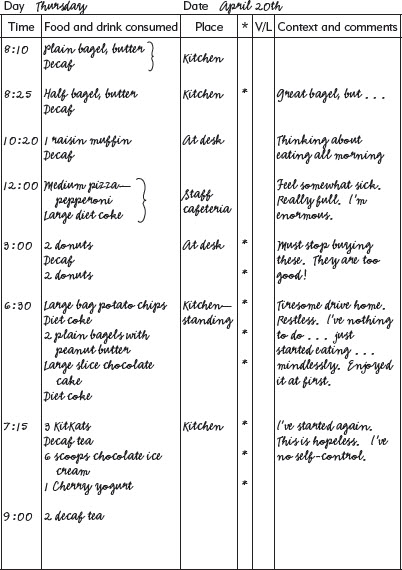
FIGURE 4. An eating record of someone with binge eating disorder. Note the general tendency to overeat, upon which binge eating is superimposed. (Asterisks signify eating viewed by the person as excessive. V/L signifies vomiting or laxative use.)
Binge eating disorder affects a broader range of people than anorexia nervosa and bulimia nervosa; the gender distribution is more even with about a third of cases being male, and the age range is broader, stretching from the teens to middle age. It also tends to have a phasic course in which there are periods when the person is prone to binge interspersed with others when he or she has control over eating. These phases may be quite long, lasting months or even years.
Community-based studies of binge eating disorder indicate that those who seek help are an atypical subgroup. The cases in the community are younger and most are not overweight.
THE ATYPICAL EATING DISORDERS
Many eating disorders do not meet the diagnostic criteria for anorexia nervosa, bulimia nervosa, or binge eating disorder. These eating disorders have attracted a variety of labels, one of the more widely used ones being “eating disorder not otherwise specified” or “ED-NOS.” In this book I will employ the less cumbersome term atypical eating disorder.
The atypical eating disorders are those eating disorders seen in adults and teenagers that do not fit the technical definitions of anorexia nervosa, bulimia nervosa, or binge eating disorder. The category has recently attracted considerable attention as it has been discovered that it is much more common than had been assumed (see Figure 5). In common with bulimia nervosa and anorexia nervosa, it mainly affects teenage girls and young women.
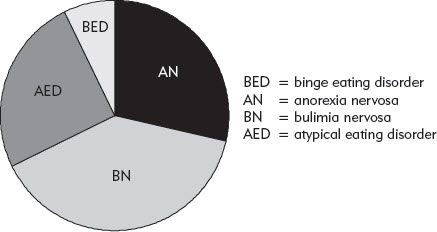
FIGURE 5. Pie chart showing the distribution of the four eating disorder diagnoses among adult patients attending a well-established eating disorder clinic. Data taken from Fairburn, C. G., & Cooper, Z. (2011). Eating disorders, DSM-5 and clinical reality. British Journal of Psychiatry, 198, 8–10.
The atypical eating disorders may be divided into five more-or-less distinct subgroups:
1. Subthreshold bulimia nervosa in which the eating disorder resembles bulimia nervosa but just fails to meet its diagnostic criteria.
2. Subthreshold anorexia nervosa in which the eating disorder resembles anorexia nervosa but just fails to meet its diagnostic criteria.
3. Subthreshold binge eating disorder in which the eating disorder resembles binge eating disorder but just fails to meet its diagnostic criteria.
4. Mixed eating disorders in which the features of bulimia nervosa, anorexia nervosa, or binge eating disorder are combined in such a way as to make it impossible to classify the state as a variant of a single one of these disorders.
5. Night eating syndrome in which there are recurrent episodes of eating in the evening or during the night.
MIXED EATING DISORDERS
What may be termed mixed eating disorders are the most common form of atypical eating disorder. The term refers to eating disorders in which the features of anorexia nervosa and bulimia nervosa, and sometimes binge eating disorder, are jumbled up together. An example would be someone with the overevaluation of shape and weight that is characteristic of anorexia nervosa and bulimia nervosa, a somewhat low weight (but not low enough to be said to have anorexia nervosa), occasional but not regular binges, extreme dieting, and intermittent self-induced vomiting.
What is known about such eating disorders is that they are equivalent to bulimia nervosa in terms of their severity, duration, and impact on the person’s quality of life. Often the person has had anorexia nervosa or bulimia nervosa in the past. Binge eating is a common feature of the mixed eating disorders.
You may come across the term purging disorder. This is a term used by some clinicians to refer to an eating disorder in which there is recurrent purging (mainly in the form of self-induced vomiting or the misuse of laxatives or diuretics) in the absence of binge eating. Our data from Oxford indicate that most of these people report having subjective binges and so may be better viewed as having a form of subthreshold bulimia nervosa.
NIGHT EATING SYNDROME
Night eating syndrome is a relatively new diagnosis about which much remains to be learned. In principle, three features have to be present to make the diagnosis:
1. Recurrent episodes of eating at night (after falling asleep) or eating excessively during the evening.
2. Awareness of the behavior at the time.
3. The pattern of eating results in significant distress or impairment.
Night eating syndrome tends to begin during early adulthood and it seems to run a long-term course, although there may be extended periods when it is not present. It tends to be particularly prevalent among people with insomnia or obesity and those with binge eating disorder. It appears to run in families, and it is equally common among men and women.
The only eating disorder that can get confused with night eating syndrome is binge eating disorder. There are four main differentiating features. In night eating syndrome the episodes of overeating only occur in the evening or at night; the episodes are relatively small in size (averaging about 300 calories); there is often no sense of loss of control at the time; and the eating is frequently motivated by the goal of getting back to sleep.
THE TRANSDIAGNOSTIC PERSPECTIVE
The diagnostic distinctions above delineate the main forms of eating disorders that exist. However, they have shortcomings. First, they can blind one to the important fact that people with eating disorders have a remarkable amount in common. Most important, they share similar eating habits and similar concerns about shape and weight. This results in some of the diagnostic distinctions being particularly difficult to make. Take, for example, a person with all the features of bulimia nervosa but a somewhat low weight—perhaps a BMI around 18.0. What diagnosis this person is given depends largely on whether this BMI is viewed as “significantly low”—a matter of debate. If it is viewed as significantly low, then they are likely to be given the diagnosis of anorexia nervosa; if it is not, the person will be said to have bulimia nervosa. Another problematic boundary is that between bulimia nervosa and binge eating disorder. In people who do not vomit or take laxatives, the distinction hinges mainly on how little they eat between their binges. If it is very little, they are likely to be given a diagnosis of bulimia nervosa, whereas if it is somewhat larger, they will be said to have binge eating disorder. In other words, there are no sharp dividing lines between the various eating disorders.
A second limitation of the diagnostic system is that the three eating disorder diagnoses provide an incomplete picture of the range of problems that are present, both in community and clinic samples. As we have already discussed, many eating disorders do not meet the diagnostic criteria for anorexia nervosa, bulimia nervosa, or binge eating disorder, and so have to be placed into a neglected residual category, termed here atypical eating disorder.
The meaningfulness of the diagnostic distinctions is further undermined by the fact that most eating disorders change in form over time. It is not uncommon for a person to be eligible for one eating disorder diagnosis in January and another in June, without a major change in their state. “Diagnostic migration” is the norm, rather than the exception. In my clinical practice I have encountered innumerable people in their 20s or 30s who have had an eating disorder since their teens, but at one stage it would have been called anorexia nervosa, later on bulimia nervosa, and most recently an atypical eating disorder. Have they really had three separate mental health disorders, one after the other? No, they have had a single eating problem that has evolved in form over time.
This book adopts a “transdiagnostic” perspective on eating problems and how to overcome them. Part I describes the full range of problems that people experience and what causes them to persist. Part II describes a way of breaking out of those eating problems in which binge eating is a major feature, irrespective of the eating disorder diagnosis.