FIGURE 6. The Cosmopolitan notice (from the “Health Reports” page of the April 1980 issue).
For anyone who binges, the answer to this question is of great interest because many people have the sense that they are the only one. To a large extent this is the result of the shame and secrecy that accompany the behavior. This secrecy has been a problem for researchers too as it has made it difficult to discover exactly who does binge.
THE EMERGENCE OF BULIMIA NERVOSA
Interest in the number of people who binge has its origins in the identification of bulimia nervosa in the mid-1970s. The first sign of the problem came with the publication of a number of reports describing “bulimarexia” or the “binge–purge syndrome” among female students on U.S. college campuses. The problem came to wider attention with the publication in 1979 of a paper titled “Bulimia nervosa: An ominous variant of anorexia nervosa” written by Gerald Russell from London, a respected authority on anorexia nervosa. In this paper he described the characteristics of 30 patients (28 women and two men) whom he had seen between 1972 and 1978. These patients had bulimia nervosa as we know it today.
Simultaneously in Edinburgh, I was seeing a similar group of patients. The most striking thing about these patients was that the majority thought they were the only person with their type of eating problem. They thought that they alone had repeated bouts of uncontrolled overeating followed by vomiting or taking laxatives. Their view was not surprising since bulimia nervosa had not yet attracted public attention. Indeed, in those days binge eating had hardly been heard of.
Most of my Edinburgh patients had kept their eating problem secret for many years. They had done this in part because of shame and self-disgust and in part because they thought that nothing could be done to help them. And keeping the problem hidden was not too difficult since most had an unremarkable body weight and most could eat relatively normally when with others. Their binge eating occurred in private. Some described having eventually summoned up the courage to see their family doctor, only to be told that they could not have an eating problem because their weight was normal.
The fact that my patients had kept their problem hidden for many years suggested that it might not be an unusual variant of anorexia nervosa, as suggested by Gerald Russell; rather, it might be a significant health problem in its own right. The challenge was to find out whether this was indeed the case. How could hidden cases be uncovered?
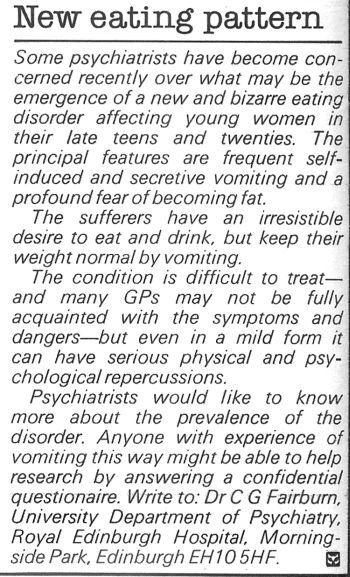
The solution was to enlist the help of the magazine Cosmopolitan. Since most of my patients were young women, I guessed that many might read this magazine. So I arranged for a small notice to be placed in the April 1980 issue of the U.K. edition (see Figure 6). The result was dramatic. Within a week or so I had received letters from more than a thousand women, the majority of whom seemed certain to have bulimia nervosa (see Box 4).
FIGURE 6. The Cosmopolitan notice (from the “Health Reports” page of the April 1980 issue).
BOX 4. The Cosmopolitan study.
To find out whether bulimia nervosa was a significant, yet undetected, health problem, a notice was placed in the Health Reports page of the April 1980 issue of the women’s magazine Cosmopolitan (see Figure 6). It asked people who were using self-induced vomiting as a means of weight control to write in if they were willing to complete a confidential questionnaire. Vomiting was chosen as the feature for identifying potential cases since it is the least ambiguous of the core features of bulimia nervosa.
Within a week or so more than a thousand replies were received. The first 800 were sent a questionnaire designed to obtain information on weight, eating habits, and attitudes toward shape and weight. Six hundred and sixty-nine questionnaires (84%) were returned fully completed. On the basis of the responses it was clear that 499 of the respondents were highly likely to have bulimia nervosa.
All 499 cases were women (remember, it was a women’s magazine). Their average age was 24 years, and two-thirds were in their 20s. Over three-quarters (83%) had a body weight within the healthy range for their age and height. In most cases the eating problem had started in their teenage years, and they had been binge eating, on average, for 5 years. A quarter (27%) reported that they were binge eating at least daily, and over half (56%) vomited daily. Nineteen percent abused laxatives.
The degree of distress reported by these women was extreme. Many wrote lengthy letters pleading for help. Two-thirds (68%) had clinically significant levels of depression and anxiety. Most expressed surprise and relief at knowing that they were not the only one with the problem.
Over half these women thought that they needed professional help, yet only 2.5% were receiving any form of treatment. Of those who wanted help, fewer than half (43%) had ever mentioned the problem to a health professional.
The findings of this study strongly suggested that bulimia nervosa was a significant, largely undetected problem.
Source: Fairburn, C. G., & Cooper, P. J. (1982). Self-induced vomiting and bulimia nervosa: An undetected problem. British Medical Journal, 284, 1153–1155.
More or less simultaneously in Chicago, Craig Johnson was receiving large numbers of requests for information following the publication of various popular articles on bulimia nervosa. He and his colleagues also sent out a number of questionnaires and in this way identified 361 women with bulimia nervosa (termed bulimia in the United States at the time). These women were very similar to those identified through Cosmopolitan (see Table 1).
TABLE 1. A comparison of the samples recruited in two early surveys of bulimia nervosa.
| British sample | American sample | |
| Age (in years) | 23.8 | 23.7 |
| Marital status | ||
Married (%) |
20.7 | 18.4 |
| Binge eatinga | ||
Age at onset (years) |
18.4 | 18.1 |
Duration (years) |
5.2 | 5.4 |
Frequency—at least daily (%) |
27.2 | 50.0 |
| Self-induced vomiting | ||
Frequency—at least daily (%) |
56.1 | 45.7 |
| Laxative misuse | ||
Regular misuse (%) |
18.8 | 33.0 |
| Weighta | ||
Normal weight |
83.2 | 61.6 |
Ever overweight (%) |
45.2 | 50.1 |
Menstrual disturbance (%) |
46.6 | 50.7 |
Sources: British sample—Fairburn, C. G., & Cooper, P. J. (1982). Self-induced vomiting and bulimia nervosa: An undetected problem. British Medical Journal, 284, 1153–1155.
American sample—Johnson, C. L., Stuckey, M. K., Lewis, L. D., & Schwartz, D. M. (1983). A survey of 509 cases of self-reported bulimia. In P. L. Darby, P. E. Garfinkel, D. M. Garner, & D. V. Coscina (Eds.), Anorexia nervosa: Recent developments in research. New York: Alan Liss.
aDifferent definitions were used in the two studies.
Other clinics were also encountering cases of this “new” eating disorder. More or less simultaneously the disorder emerged in North America, the United Kingdom, Australia, and New Zealand.
Little is known about the origins of bulimia nervosa. It is possible that it was a source of undetected suffering years, decades, or even centuries before the disorder was recognized. Indeed, the experience of my Edinburgh patients and those who responded to the Cosmopolitan notice indicates that the disorder certainly went undetected at least for a time. This said, there are far fewer documented cases of binge eating and purging predating the mid-20th century than there are of individuals who have had anorexia nervosa. Overall, it seems unlikely that bulimia nervosa plagued young women for centuries before the disorder was recognized. But the question of why there was such a dramatic upsurge in the 1970s remains unanswered. Research into the causes of bulimia nervosa provides some clues (see Chapter 6).
THE MATTER OF DETECTION
You will perhaps have been struck by the fact that only 2.5% of those identified in the Cosmopolitan study were in treatment. Today far more people seek help, but typically this is after a significant delay. Why is this? There are many reasons:
1. As we have already discussed, binge eating problems are accompanied by feelings of shame and guilt. By seeking treatment, sufferers run the risk of others finding out about their problem and the years of deceit and subterfuge that have been required to keep it secret.
2. Men may find it particularly difficult admitting to having a binge eating problem as these problems are widely viewed as being confined to women.
3. Some people feel they do not deserve help.
4. Some people think their eating problem is not severe enough to merit treatment.
5. Some people hope the problem will resolve of its own accord.
6. Others do not want help as they obtain some benefit from the problem. For example, it might help them cope with intense emotions (see Chapter 6) or it might provide them with an excuse for not performing well in some aspect of life (e.g., career, relationships).
7. There may be financial barriers to getting help. Sufferers may not have the financial resources or insurance needed to cover the cost of treatment. Shockingly, some insurance companies do not provide coverage for the treatment of the atypical eating disorders.
8. It can be difficult to tell health professionals. Prior health problems (e.g., menstrual irregularity; see Chapter 5) may have been a result of the eating problem, yet the health professional was kept in the dark about their likely cause.
The fact that only a small proportion of those with binge eating problems are getting professional help is disturbing because there are treatments capable of helping them. These include the self-help program in Part II of this book.
THE FINDINGS OF COMMUNITY STUDIES
Since 1980 there have been numerous studies of the prevalence of binge eating problems. Most have focused on Caucasian women between the ages of 14 and 40 as they are thought to be most at risk. However, more and more studies are including men, a broader age range, and different ethnic groups.
The method used to detect cases is usually a simple questionnaire, but such questionnaires tend to generate inflated estimates. More reliable are the studies in which people are interviewed. Interestingly, these studies have produced relatively consistent findings. It seems that bulimia nervosa affects between 1 and 2% of young adult women whereas binge eating disorder affects about 2 to 3% of both men and women and a much broader age range. These figures are noteworthy as binge eating problems impair both quality of life (see Chapter 4) and physical health (see Chapter 5).
There have also been studies of children. These have found that binge eating does occur in children, particularly among those who are overweight. In one sample of 112 overweight children, over 5% met the criteria for binge eating disorder.
STUDIES OF OTHER SOCIAL GROUPS
There have been few studies of ethnic groups other than Caucasians. This is regrettable because there is evidence that Asian Americans and Hispanic Americans are prone to develop binge eating problems—indeed, some studies have suggested that they may be even more vulnerable.
Lower and middle income countries have also been neglected. This is largely because eating disorders have tended to be viewed as “culture-bound syndromes” of the West. This view is now outdated as more and more evidence accumulates that they occur across the globe. For example, bulimia nervosa and anorexia nervosa most certainly occur in both high- and low-income Asian countries including Japan, China, India, and Malaysia. In the Arab world, eating problems are also becoming a public health concern.