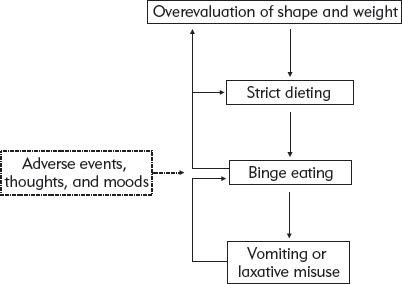
FIGURE 14. The vicious cycles that maintain binge eating.
I began binge eating when I was about 17. I was lonely, shy, and lacking in self-esteem. Every binge made me feel worse, made me hate myself more. I punished myself with more and more food. Within months I was binge eating as a matter of course and I gained weight rapidly. I loathed myself and continued with ordinary life only by pretending to be “normal.”
Circumstances improved, and I binged less. However, my eating habits remained atrocious. Food was always on my mind. I never admitted my problems to anyone. And I lied to myself—denying what I had eaten or that I had eaten at all. Now, looking back on it all, I think of the years (almost 16) wasted, thinking about food and how fat I am. So many years spent depressed and hating myself.
Stories like this one raise an obvious two-part question: Why did this binge eating problem develop, and why did it persist for so long? Unfortunately, there is no simple, or complete, answer. Our understanding of the cause of binge eating problems is still limited.
WHY THE QUESTION IS SO DIFFICULT TO ANSWER
Many Processes Are Involved
Psychological, social, and physical processes all seem to play a part in causing binge eating problems. Chapter 3 mentioned, for example, that bulimia nervosa seems to have emerged only recently. This suggests that environmental processes play a role and that these are likely to be social in nature. However, because not everyone develops a binge eating problem, despite being subject to similar social conditions, additional processes must also be involved. We have also seen that some psychological processes appear to be relevant such as the low self-esteem and perfectionism mentioned earlier, in Chapter 4. And, as this chapter shows, genetically determined processes also appear to make a contribution, which means that physical processes play a role too.
Binge Eating Problems Vary in How They Start
The research that has been done on the development of binge eating problems suggests that there is more than one route to these problems.
People with bulimia nervosa generally report that their eating problem started when they began dieting during their teenage years. This may have been provoked by a real or perceived weight problem or by a need to feel “in control” in the context of difficulties in their life. In some cases incidental weight loss (perhaps due to illness) was the trigger. Whatever the precipitant, the result is weight loss, which can be so marked that the person develops anorexia nervosa. Then, after a variable length of time, control over eating breaks down, binge eating develops, and body weight increases to near its original level.
A very different pathway is described by many people with binge eating disorder. They report a long-standing tendency to overeat, particularly when feeling unhappy or stressed. This tendency eventually becomes so marked that they develop frank episodes of binge eating. However, the binge eating tends to be phasic, that is, there are extended periods free from binge eating. This is most unlike bulimia nervosa.
To complicate matters further, some people report a mixture of these pathways especially if they have a mixed eating disorder.
Binge Eating Problems Vary in Their Course
Binge eating problems vary in their course over time. For some, the binge eating problem is short lived and does not recur. For others, recurrences and relapses are common. For others still, once the problem begins it lasts for years. This suggests that additional processes, often separate from those that were responsible for the binge eating at the outset, come into play to keep the problem going.
What processes govern whether a binge eating problem persists or remits is not clear. In Chapter 4 we discussed the contributions of strict dieting, all-or-nothing thinking, and concerns about shape and weight. As we will see in this chapter, difficulties with relationships also seem relevant, as do certain events and circumstances.
A CRUCIAL DISTINCTION
When thinking about the cause of enduring difficulties, such as binge eating problems, it is important to distinguish the processes that are likely to have caused the problem to start in the first place from those that lead it to persist. So the question of cause has two parts:
1. Why do binge eating problems develop?
2. Why do they persist?
Two phases therefore need to be distinguished: the development phase (before the onset of the problem) and the maintenance phase (after its onset).
Making this distinction not only helps us understand the role of all possible causes but it also has significant practical implications. If the goal is the prevention of binge eating problems, the task is to identify those processes that exert their influence before onset—during the development phase—and try to stop them from operating. In contrast, if successful treatment is the goal, the task is to identify the processes that are keeping the problem going.
PROCESSES THAT CONTRIBUTE TO THE DEVELOPMENT OF BINGE EATING PROBLEMS
Social Processes
As Chapter 3 discussed, bulimia nervosa appears to have emerged in the 1970s and 1980s in those parts of the world where anorexia nervosa was already encountered, mainly North America, northern Europe, Australia, and New Zealand. Because these are countries where it is fashionable for women to be slim, and where dieting among young women is common, social processes that encourage dieting may have contributed to the emergence of the disorder. Key among these is the shape of fashion models. Bulimia nervosa emerged when being extremely thin, like the English model Twiggy, became fashionable. But it is not unlikely that in different cultures different processes may contribute to the problem. Nor is the situation static as research from Fiji shows (see Box 9).
BOX 9. Culture change: lessons from Fiji.
Until the 1990s the Fijian islands were largely isolated from external social influences. They maintained a strong traditional culture that valued appetite and a healthy body size. Indeed, a robust body was valued. But perhaps the most protective feature of traditional Fijian culture was that people generally accepted their bodies.
In 1995, television broadcasting Western channels reached Fiji and an “explosion” of eating problems followed. One explanation is that the spread of Western culture led girls in particular to place new emphasis on their bodies, causing them the same dissatisfaction that is found in girls in the West. However, it has been argued that this explanation is too simple and that the particular nature of the clash between Western culture and Fijian values should also be considered. The islands were undergoing a major social transition at the time and this created concerns about achievement and social position. Interviews with Fijian schoolgirls suggest that many associated the slimness of Western actresses with power and success. Simultaneously, concerns about the health risks associated with obesity were promoting an emphasis on personal responsibility for body shape and weight. Therefore it seems likely that a variety of complex interacting processes were involved.
Source: Becker, A. E. (2004). Television, disordered eating and young women in Fiji: Negotiating body image and identity during rapid social change. Culture, Medicine and Psychiatry, 28, 533–559.
Recently, there has been a move to counter the impact of underweight fashion models. In 2006 Spain banned models with a BMI below 18.0 and in the same year Italy required the fashion industry to provide medical proof that their models did not have an eating disorder. In 2012 Israel banned models from advertisements or fashion shows if their BMI was below 18.5; and a similar line was taken by the fashion magazine Vogue. Unfortunately, there are forces working in the opposite direction. For example, some activities encourage unhealthy weight control practices and may as a result promote eating problems. This is particularly true of those in which a certain (low) weight is required at a specific time (e.g., horse racing; see Box 6) or where appearance is crucial, as in ballet (see Box 10).
BOX 10. Body image and classical ballet.
In the world of ballet the “Balanchine body,” which consists of a thin frame, long legs, a long neck, and a short torso, represents the ideal. This aesthetic is attributed to George Balanchine who was a dancer, teacher, and celebrated choreographer. It is reported that Balanchine told his dancers that he “must see the bones” and they should “eat nothing.” Whether or not this is true, there continues to be pressure on ballerinas to achieve this body type. The success of their careers depends upon it.
A recent review of The Nutcracker in The New York Times commented that one of the dancers looked as if she had “eaten one sugar plum too many.” The “Nutrition Policy” of The Royal Ballet School in London acknowledges the risk of eating problems among aspiring ballet dancers. But while the school aims to promote healthy attitudes concerning weight, eating and body image, it concedes that the pressure to be thin cannot be completely removed.
The average BMI of a ballerina is somewhere around 18.5, meaning that many are close to being clinically underweight, and a substantial number have BMIs within the anorexia nervosa range (44.3% in one study). Studies also show that many ballet dancers want to lose further weight, do not menstruate, and experience a level of body dissatisfaction somewhere between that of girls in the general population and those diagnosed with anorexia nervosa.
Sources: Ringham, R., Klump, K., Kaye, W., Stone, D., Libman, S., Stowe, S., & Marcus, M. (2006). Eating disorder symptomatology among ballet dancers. International Journal of Eating Disorders, 39, 503–508.
Bettle, N., Bettle, O., Neumärker, U., & Neumärker, K.- J. (1998). Adolescent ballet school students: Their quest for body weight change. Psychopathology, 31, 153–159.
Gender
In Chapter 3 we discussed the fact that all the eating disorders other than binge eating disorder are much more common among women than men. This pattern of women being disproportionately affected is mirrored across all cultures and ethnic groups. Why should women be at greater risk? One major reason is likely to be the fact that dieting is so much more common among women than men and, as we will discuss, dieting greatly increases the risk of developing eating problems.
This raises another question: Why do women tend to diet more than men? Two answers come to mind. First, the social pressures to be slim are focused largely on women. And second, women are more prone to base their self-worth on their appearance. Both of these observations raise important wider issues concerning differences between male and female development and the competing and conflicting roles of women in Western societies.
Ethnic Group and Social Class
When patients in treatment are considered, bulimia nervosa and anorexia nervosa seem to be largely confined to Caucasian women, but patient samples are biased with respect to ethnicity. The findings of community-based studies suggest that binge eating problems are much more evenly dispersed. As far as social class is concerned, there is similarly evidence of a social class skew, with patients with bulimia nervosa and anorexia nervosa being disproportionally more common among those with a middle- or upper-class background. But this may be due to a bias in treatment-seeking with people from middle- and upper-class backgrounds being more likely to enter treatment.
Age, Adolescence, and Puberty
There is strong evidence that binge eating problems usually develop during teenage years or in early adulthood. This age of onset can probably be attributed to the fact that dieting among women is particularly common at this age. The dieting, in turn, is likely to be the result of two forces. First, as already mentioned, women are more prone than men to judge their self-worth in terms of their appearance, and this is particularly true in this age group. Second, at puberty many young women begin to develop a body shape that deviates from that considered fashionable.
This is not the same for men. Although men are under pressure to look a certain way, male puberty creates an appearance that society desires. As boys go through puberty their musculature and height increase and their shoulders become broader.
Adolescence itself may also be relevant. As we all know, this stage in life presents major developmental challenges: changing appearance, fluctuations in mood, and changes in social expectations and roles. Teenagers who have the personality traits thought to put people at risk of developing binge eating problems—perfectionism and low self-esteem—are more prone to experience a sense of loss of control at this time. Some find that dieting helps restore their sense of being in control and, as a behavior considered socially desirable by their peers, it also gives them a sense of achievement. For them, dieting may be more about self-control than anything else.
The timing of pubertal changes in relation to one’s peers may also be important. It is thought that early development in girls may heighten their risk of emotional difficulties because it increases the probability that they will have to confront new problems and expectations before they are ready to do so. Additionally, the changes in shape may be particularly difficult to cope with if they occur prior to the rest of their peer group.
Certain age-dependent life changes are also relevant. A particularly important one is leaving home to go away to college. It is not at all uncommon for eating problems to develop or worsen at this time. It is easy to see why this occurs. Not only is the home-to-college transition a stressful one, but for some teenagers it is the first time that they have had full control over what and when they eat. As a result some go through a phase of unchecked undereating while others overeat and gain substantial amounts of weight.
Obesity
Research findings indicate that there is a raised rate of childhood and parental obesity among people who develop bulimia nervosa, and the same appears to be true of those with binge eating disorder. Naturally any tendency to be overweight during the childhood or teenage years is likely to magnify concerns about body shape and weight, and thereby encourage dieting. In addition, having a family member with a significant weight problem may sensitize people to “fatness” and dieting, making them strive to avoid it by restricting their eating.
Eating Problems and Disorders within the Family
It is well established that eating disorders run in families. The close relatives of a person with an eating disorder have an increased risk of developing one themselves. This could be due to genetic factors, and the research findings do indeed suggest that there is a significant genetic contribution. This said, what is inherited is not known. There are many possibilities, including the tendency to be a particular weight, biological or psychological responses to dieting, and certain personality traits. Nor is it clear which specific genes are likely to be involved. It is not unlikely that “epigenetic” processes contribute; for example, dieting may alter gene expression.
The fact that eating disorders run in families does not necessarily indicate that inherited factors are wholly or even partly responsible. Aggregation within families could be due to environmental influences. A number of studies have been done concerning the eating habits and attitudes of the family members of those with eating problems. To date these studies have mainly focused on the relatives of patients with anorexia nervosa, and their findings have varied greatly. Some have found high rates of unusual eating attitudes and behavior; others have not.
In clinical practice accounts of apparent contagion are not uncommon. An example is mothers putting pressure on their daughters to join them on a diet (see Box 11).
BOX 11. Mothers, daughters, and disturbed eating.
Two groups of mothers and daughters were identified on the basis of the daughters’ scores on a widely used measure of disturbed eating. There was a high-scoring group and, for comparison purposes, a low-scoring group. The average age of the daughters was 16 years and the mothers was 43 years.
The mothers of the daughters with disturbed eating differed from the comparison mothers in the following noteworthy ways:
1. They had more disturbed eating habits.
2. They thought that their daughters should lose more weight.
3. They were more critical of their daughters’ appearance.
These findings suggest that the transmission of eating disorders within families may be, at least in part, due to contagion.
Source: Pike, K. M., & Rodin, J. (1991). Mothers, daughters, and disordered eating. Journal of Abnormal Psychology, 100, 198–204.
Other Psychiatric Disorders within the Family
The possibility that other psychiatric disorders in the family might contribute to eating disorders has also been studied. Most of this work has focused on people with anorexia nervosa or bulimia nervosa.
The psychiatric disorder that has been most widely studied is clinical depression. The findings suggest that the presence of depression within a family increases the risk that daughters will develop an eating problem. We do not know what mechanism might be responsible for this association. On the one hand, there could be a common underlying physiological abnormality, such as a defect in the regulation of serotonin in the brain, a chemical thought to be involved in both depression and the control of food intake. On the other hand, it could be the environmental influence on the child of being brought up by a depressed parent.
The other disorder to have been studied is psychoactive substance abuse (i.e., alcohol or drug abuse). The findings are discussed in Chapter 7.
Events and Disorders during Childhood
Clinicians who work with those with binge eating problems cannot fail to notice how common it is for traumatic events to have occurred during their patients’ childhoods. Deaths, separations, parental disharmony, physical illnesses, teasing, sexual and physical abuse, and bullying all seem to occur with disturbing frequency. However, research indicates that such events occur no more often among these patients than among those with other psychiatric disorders, suggesting that they increase the risk of developing a psychiatric disorder, but not necessarily an eating disorder.
It has also been found that there is an increased rate of psychiatric problems before the onset of the eating problem. Anxiety problems are particularly common and a small subgroup has a history of childhood depression.
Personality Characteristics
As I mentioned in Chapter 4, certain personality traits seem to be common among those who develop binge eating problems. Most of the research on this topic has focused on people with bulimia nervosa or anorexia nervosa. Its relevance to binge eating disorder is uncertain.
Those who develop bulimia nervosa or anorexia nervosa are unusually compliant and conscientious as children. They are often somewhat shy and solitary, and they may have had difficulty mixing with other children. In addition, they tend to be competitive and achievement-oriented. They set themselves high standards and work hard to meet them. These traits seem to be the precursors of the low self-esteem and perfectionism seen in many people with anorexia nervosa or bulimia nervosa.
Exploratory psychotherapy often confirms these findings. Michael Strober from UCLA, a leading expert on personality and eating disorders, has stated that a detailed investigation of these patients’ inner worlds reveals “the omnipresent fear of seeming weak, inadequate and average; the inability to take pleasure in leisure; a reluctance to confront risks and novelty, to engage in uninhibited spontaneous action, or to assert feelings; and the experiencing of impulses and desires as wasteful distractions to achieving higher moral objectives.” Michael Strober argues that personality characteristics of this type result in these people being “hopelessly ill prepared” for the developmental demands of adolescence.
The personality characteristics of those who develop binge eating disorder have not been characterized so thoroughly. Problems with assertiveness and low self-esteem seem to be especially common, whereas perfectionism seems more restricted to those who develop anorexia nervosa, bulimia nervosa, or an atypical eating disorder.
Dieting
In Chapter 4 we discussed the link between binge eating and strict dieting and the fact that both perpetuate each other. However, dieting also increases the risk of developing a binge eating problem in the first place; indeed, it is a well-substantiated risk factor for anorexia nervosa and bulimia nervosa. It seems less relevant to binge eating disorder. Still, we know that the majority of those who diet do not develop eating problems. Therefore, other factors of the type already mentioned must somehow interact with dieting in the etiological process. Also, it may be that only certain forms of dieting are prone to put people at risk.
The Bottom Line: There Is No Single Cause
To conclude, there is no single cause of binge eating problems. There are a variety of risk factors and a variety of modes of onset. If you have a binge eating problem a multitude of factors are likely to have contributed to its development. However, as we shall now see, rather fewer processes are likely to be causing it to persist.
PROCESSES THAT PERPETUATE BINGE EATING PROBLEMS
The research on how binge eating problems change over time and what factors influence their course suggests that a limited number of interacting processes are involved. These are illustrated in Figure 14 and are discussed in turn.
FIGURE 14. The vicious cycles that maintain binge eating.
Ongoing Dieting
In Chapter 4 we considered the various ways in which dieting makes people prone to binge. If the dieting is “extreme” (i.e., if the dieter exercises such restraint that he or she eats very little), strong physiological pressures will come to bear. And if the dieting is “strict” (the dieter sets highly specific dietary goals and holds an all-or-nothing attitude toward them), he or she will tend to swing between dieting and binge eating, with each promoting the other. Through these mechanisms, ongoing dieting seems to maintain many binge eating problems. It is for this reason that many treatments focus on eliminating or moderating dieting. This especially applies to treatments for anorexia nervosa, bulimia nervosa, and the atypical eating disorders. It is less relevant to binge eating disorder as in most cases there is little or no dieting.
Various factors encourage dieting, the main ones being the need to feel in “control” mentioned earlier and the influence of concerns about appearance and weight. Again, as discussed earlier, these concerns are reinforced by Western society’s preference for a slim body shape. People who have been overweight in the past may be particularly likely to diet for fear of regaining their lost weight, and their efforts may be encouraged by friends and relatives.
Vomiting and the Misuse of Laxatives
Both of these methods of weight control encourage binge eating because belief in their effectiveness neutralizes a major deterrent against binge eating, namely, the fear of weight gain. This faith is unfounded, however, as we discussed in Chapter 4.
Adverse Moods and Thoughts
Mood and eating are linked in everyone, not just in those with eating problems. But binge eating has a particularly complex and circular relationship with mood. People who binge find that their binge eating helps them cope with adverse moods and thoughts because it is both distracting and calming. In this way some can come to rely on binge eating to cope with such thoughts and feelings, while being unaware of the link.
Relationships, Events, and Circumstances
A variety of events and circumstances also influence the course of binge eating problems. Personal relationships are particularly important in this regard. For example, establishing a close and accepting relationship with a partner may improve self-esteem, decrease concerns about shape and weight, and remove some sources of stress, thereby promoting recovery. The breakdown of a relationship can have the opposite effect.
Desire to Change
The processes just discussed do not constitute an exhaustive list. In fact our discussion of the processes contributing to the persistence of binge eating problems omitted one key factor, namely, the desire to change. Some people seem to have little desire to change. They accept their binge eating problem and adjust their life around it. In such cases the problem tends to persist, often year in, year out. Others decide to change, to make a fresh start and, interestingly, having made the decision, some are able to overcome the problem without outside help. Others, however, cannot.
What stimulates people to decide to change—to make a fresh start—has not been studied, but it should be. One of my hopes is that reading this book might provide some readers with just such a stimulus.