4
Implications of Developmental
Levels of Organization
Like politics, psychotherapy is the art of the possible. One advantage of conceptualizing each client developmentally is that one can derive a sense of what is reasonably expectable, with optimal treatment, for each one. Just as a physician expects a healthy person to recover faster and more completely from an illness than a sickly one, or as a teacher assumes that an intelligent student will master more material than a slow one, a therapist should have different expectations for people with different levels of character development. Realistic goals protect patients from demoralization and therapists from burnout.
It was easier to write the first edition of this chapter; in the early 1990s there was something closer to a psychoanalytic consensus about what approach is appropriate for each level of personality organization. Since that time, several things have occurred. Analysts in the relational movement have challenged many aspects of traditional technique—especially its assumptions about the analyst’s capacity for objectivity and neutrality. They have also questioned the value of any generalizations about character structure and have revised our understandings of the patient–therapist dyad to put the emphasis on what the two parties construct together rather than on what the therapist does for or to the patient. The two-person model of the therapeutic process has gone mainstream and has influenced even those who think more traditionally. It will probably be evident, even in this book with its one-person focus on patients’ individual psychologies, that relational analysts have greatly influenced my thinking.
At the same time, several specific therapies for borderline personality organization have been developed, and psychoanalytic theorists no longer dominate professional conversations about how to understand borderline phenomena. Marsha Linehan, the architect of dialectical behavior therapy (e.g., 1993), has frequently acknowledged her debt to Otto Kernberg, but the treatment she created reflects both cognitive-behavioral concepts and some Zen Buddhist ideas, not assumptions about a dynamic unconscious. Jeffrey Young’s schema therapy (e.g., Rafaeli, Bernstein, & Young, 2010), which also derives from cognitive-behavioral psychology with some psychodynamic influences, has been applied to borderline-level personality disorders. In the specifically psychoanalytic realm, where Kernberg’s original notion of expressive therapy once predominated, we have seen the development of several specific, research-tested treatments: Kernberg’s transference-focused psychotherapy (Clarkin, Yeomans, & Kernberg, 2006) and Fonagy’s mentalization-based therapy (Bateman & Fonagy, 2004) being the best known.
Finally, the International Society for the Psychological Treatments of Schizophrenia has brought together therapists interested in psychotherapy with psychotic patients, and their synergy has added new elements to what we know about treating severely troubled people. Even more than in 1994, our mental health culture tends to overstate the pharmaceutical needs of people with psychoses and to understate their need for therapy. I think there is greater urgency now than in earlier decades to pass on our knowledge about effective talk therapy for those who suffer the most.
I start, as before, with considerations about treating neurotic-level clients, then those in the psychotic range, and finally those in the borderline spectrum. Even though the story has become more complicated, I think it is still useful to note clinical implications of levels of severity. I cannot do justice to the subtleties of specific approaches, but I try to present enough of a feel for how to work, depending on a person’s inferred developmental challenges, that I demonstrate the value of assessing these levels. The goal of any dynamic therapy is to help each client with the maturational task that is most compelling for that person—whether that is the full flowering of one’s creativity or the attainment of some minimal awareness that one exists and deserves to stay alive.
THERAPY WITH NEUROTIC-LEVEL PATIENTS
It used to be commonly claimed that psychoanalytic therapy is unsuited to anyone but the “worried well.” The kernel of truth in this view is that psychoanalysis as a specific treatment works best with articulate neurotic-level clients who have the ambitious goal of character change and/or deep self-knowledge. The arrangements that define classical Freudian analysis (frequent sessions, free association, use of the couch, attention to transference and resistance, open-ended contract) work less well for other patients—although early in the psychoanalytic movement, before modified approaches were developed, analysis was attempted with a wide array of clients. Also, the session frequency that Freud had recommended (originally six, then five times a week; later four or even three) made traditional analysis affordable only by people of some means.
That psychoanalytic therapy works faster and goes further with already advantaged people can be compared to the responses of healthy people to medical care or bright people to education. There are many reasons why it is easier to do analytic therapy with healthier patients than with borderline or psychotic individuals. In Eriksonian terms, one can assume basic trust, considerable autonomy, and a reliable sense of identity. Treatment goals may include removing unconscious obstacles to full gratification in the areas of love, work, and play. Freud equated psychoanalytic “cure” with freedom, and in the Platonic tradition, he believed it is truth that ultimately makes us free. A search for difficult truths about the self is possible for neurotic-level people because their self-esteem is resilient enough to tolerate some unpleasant discoveries. Accordingly, Theodor Reik (1948) used to say that the primary requisite to conduct or undergo analysis is moral courage.
Psychoanalysis and Open-Ended Psychoanalytic Therapies
Neurotic-level patients quickly establish with the therapist a working alliance in which the clinician and the observing part of the client are allies in accessing previously unconscious or disavowed defenses, feelings, fantasies, beliefs, conflicts, and strivings. If the patient is seeking a thorough understanding of his or her personality, with the goal of the greatest possible degree of growth and change, intensive analysis should be considered. Lately, students in psychoanalytic training constitute the majority of patients willing at the outset to make the three-or-four-sessions-per-week commitment that analysis dictates (usually because their training institute requires it), but some patients who are not in the mental health field decide after a period of less intensive therapy that they want to “go deeper” and move from analytically oriented treatment (twice a week or less) into analysis. In the United States, this is happening less frequently, not because of lack of interest, but because of insurance companies’ unwillingness to fund intensive treatments.
The fact that psychoanalysis may go on for years does not obviate the fact that, perhaps especially with healthier persons, symptomatic and behavioral improvement may happen quickly. But people have a feel for the difference between behavior change that is possible in spite of one’s psychology and behavior change that has come to feel congruent with one’s insides. To move from the first to the second is one reason people may choose to stay in analytic treatment for the long haul. An analogy would be the difference that a man addicted to alcohol feels between early sobriety, during which he struggles minute by minute to resist the temptation to drink, and later recovery, when he no longer feels the urge. The behavior of not drinking is the same in early and late sobriety, but the underpinnings of it change. It may have taken years of AA meetings and unremitting discipline to alter old patterns, habits, and beliefs, but to the recovering alcoholic the shift from a barely controlled compulsion to indifference toward alcohol is a priceless achievement.
For neurotic-level people who are unable or unwilling to take on the commitment of time, money, and emotional energy involved in intensive analysis, psychoanalytic (or “psychodynamic”) therapy, which developed as a modification of classical analysis in the direction of being more specifically problem focused, may be the treatment of choice. Patient and therapist meet for fewer than three sessions a week, usually face-to-face. The therapist is less encouraging of emotional regression and more active in pointing out themes and patterns that patients who come more frequently tend to notice by themselves. Both psychoanalysis and modified psychoanalytic therapies have been referred to as “uncovering” or “exploratory” or “expressive” treatments because the invitation to the client is to be as open as possible, to focus on feelings, and to try to push past defensiveness. Sometimes they have been also called “insight-oriented” therapies, in reference to the analytic assumption that self-knowledge reduces conflict and promotes growth.
Short-Term Treatments and Nonpsychodynamic Therapies
Patients in the neurotic range are also often good candidates for short-term analytic therapies (Bellak & Small, 1978; Davanloo, 1980; Fosha, 2000; Malan, 1963; Mann, 1973; Messer & Warren, 1995; Sifneos, 1992). Intensive focusing on a conflict area can be overwhelming to someone with a borderline or psychotic structure; in contrast, a neurotic-level person may find it stimulating and productive. Similarly, higher-functioning clients tend to do well in analytically informed group and family modes of treatment, while borderline and psychotic people often do not. (Lower-functioning clients absorb so much of the emotional energy of the group or family unit that the other parties get hopelessly torn between resentment at their always being center stage and guilt about that resentment, as the more troubled person is obviously suffering so much.)
In fact, virtually any approach to therapy will be helpful to most clients in the neurotic range. In CBT therapy they tend to do any homework the therapist suggests, and with biologically oriented psychiatrists, they may willingly take the medicines they are prescribed. They have had enough experiences with loving people that they assume benevolence in the therapist and try to cooperate. They are, understandably, popular clients. One of the reasons for the prestige that once attended classical analysis may be that people with the requisites to be analysands are readily responsive to and appreciative of their treatment. They are good advertisements for their analysts, unlike borderline people, for example, who may—even when they may be improving in therapy—disparage their therapists ruthlessly to outsiders or idealize them in such a cloying way that everyone in their circle of friends thinks they have been taken in by a master charlatan.
Most psychodynamic writers feel that intensive psychoanalysis offers neurotically organized people the greatest ultimate benefits and that anyone with the resources to undergo in-depth, high-frequency treatment, especially someone in young adulthood with years ahead to reap the psychological rewards, would be well advised to do so. I share this opinion, having benefited all my adult life from a good early classical analysis. It is also true, however, that a person in the neurotic range can benefit from all sorts of different experiences and can extract psychological growth even from some conditions that others might find disabling.
THERAPY WITH PATIENTS IN THE PSYCHOTIC RANGE
Probably the most important thing to understand about people with psychotic illnesses or psychotic-level psychologies is that they are terrified. It is no accident that many drugs that are helpful for schizophrenic conditions are major antianxiety agents; the person with a vulnerability to psychotic disorganization lacks a basic sense of security in the world and is ready to believe that annihilation is imminent. Adopting any approach that permits a lot of ambiguity, as does traditional analytic therapy with neurotics, is like throwing gasoline into the flame of psychotic-level terror. Consequently, the treatment of choice with psychotic-level patients has generally been framed as “supportive therapy,” an approach that emphasizes active support of the patient’s dignity, self-esteem, ego strength, and need for information and guidance.
All therapy is supportive, but in the ego psychology tradition the phrase has had a narrower meaning, reflecting the experience of several decades of psychodynamic work with more deeply disturbed people (Alanen, Gonzalez de Chavez, Silver, & Martindale, 2009; Arieti, 1974; Eigen, 1986; Federn, 1952; Fromm-Reichmann, 1950; Jacobson, 1967; Karon & VandenBos, 1981; Klein, 1940, 1945; Lidz, 1973; Little, 1981; Pinsker, 1997; Rockland, 1992; Rosenfeld, 1947; Searles, 1965; Segal, 1950; Selzer, Sullivan, Carsky, & Terkelson, 1989; Silver, 2003; Sullivan, 1962; R. S. Wallerstein, 1986). It is generally agreed that there is a continuum from supportive through expressive (or “uncovering,” or “exploratory”) therapy (Friedman, 2006), in which at the uncovering end one encourages full expression of intrapsychic conflict, leading to insight and resolution, while at the supportive end one tries to “support the ego in its struggle to contain, or repress intrapsychic conflicts and to suppress their symptomatic expression” (R. S. Wallerstein, 2002, p. 143). Much of what I cover in this section can apply to work with any patient but is particularly critical to working with more disturbed people.
Explicit Safety, Respect, Honesty
The first aspect of supportive work I should mention is the therapist’s demonstration of trustworthiness. The fact that psychotic-level people are often compliant does not mean that they trust. In fact, their compliance may mean quite the opposite: It may express their fear that authorities will kill them for being separate, for having their own will. The therapist needs to keep in mind that it is important not to act in ways that reinforce the primitive images of hostile and omnipotent authority with which psychotic-level people are tormented. To prove that one is a safe object is not so easy. With a neurotic-level person in a paranoid state, it may be enough to interpret the transference, that is, to comment on how the patient is mixing one up with some negative person from the past or some projected negative part of the self. Interpretation of this sort is useless with severely disturbed people; in fact, they are likely to consider it a diabolical evasion.
Instead, one must repeatedly counteract the patient’s most frightening expectations. A facial expression that conveys respect is enough to make a neurotic-level patient comfortable, but with a person at risk for psychosis, one must demonstrate much more actively one’s acceptance of the patient as a morally equal human colleague. This might include simple communications such as asking such clients to tell you if it gets too warm or too cold in the office, asking their opinions about a new painting, creating opportunities for them to demonstrate areas of personal expertise, or commenting on the creative and positive aspects of even their most bizarre symptoms. In this context, Karon (1989) has provided a pertinent example:
Therapeutically, it is often useful to tell the patient, “That is a brilliant explanation.” The patient is generally startled that any professional would take his or her ideas seriously. “You mean you think it is right?” If, as is usually the case, the therapist believes that the patient can tolerate it, the therapist might usefully say, “No, but that is because I know some things about the human mind which you don’t know yet, and I’ll tell you if you’re interested. But given what you do know, that is a brilliant explanation.” With such a nonhumiliating approach to the patient, it is often possible to get the most suspicious paranoid to consider what might be going on and its real meaning as an attempt to solve the terrifying dilemmas of his or her symptoms and life history. (p. 180)
Another aspect of demonstrating that one is trustworthy is behaving with unwavering honesty. Anyone experienced with schizophrenic clients can attest to their attunement to affective nuance and their need to know that their therapist is emotionally truthful. Psychotic-level people require much more emotional self-disclosure than other patients; without it, they may stew in their worst fantasies. This is an area where supportive therapy diverges from traditional analytic therapy with neurotic-level people. With healthier people, one may avoid emotional revelations so that the patient can notice and explore what his or her fantasies are about the therapist’s affective state. With more troubled clients, one must be willing to be known.
Take irritation, for example. It is natural for the therapist to feel irritated with any patient at various points, especially when the person seems to be behaving self-destructively. A perception that one’s therapist looks annoyed would be upsetting to any client, but it is mortally terrifying to more deeply troubled ones. If a neurotic-level person asks, “Are you mad at me?” one helpful response would be something along the lines of “What are your thoughts and feelings about what it would mean if I were mad at you?” If the same query is made by a potentially psychotic patient, the therapeutic reply might be “You’re very perceptive. I guess I am feeling a little irritation. I’m a bit frustrated that I can’t seem to help you as fast as I would like. What was your reason for asking?”
Notice that with the supportive approach, one still invites the patient to explore his or her perceptions, but only after a potentially inhibiting apprehension has been directly counteracted by specific information. In the example above, the therapist has also explicitly expressed respect for the patient’s accurate perception, thus supporting his or her realistically based self-esteem, and has implicitly counteracted primitive fantasies of the therapist’s dangerous omnipotence by connecting anger with ordinary human limitation rather than with talionic destruction. No one who finds it uncomfortable to admit to baser human motives should work with people in the psychotic range; they can smell hypocrisy, and it literally makes them crazy.
Along these lines, it is important with a psychotic-level patient to give explicit rationales for one’s way of working, rationales that will make emotional sense to the person. Higher-functioning people are often therapy-savvy, and if any arrangement does not seem reasonable to them, they will usually ask about it. Take the fee, for example. With neurotic patients, regardless of how many fantasies they have about what money means to you and to them, there is rarely a need to go into why one charges what one does. It was part of the original contract, and the reasonable part of the healthier patient understands that this is a relationship where a fee is charged for services rendered.
Psychotically vulnerable people, in contrast, can have all kinds of secret and very peculiar ideas about the meaning of money exchange—not in the form of fantasies that coexist with more rational notions, but as their private conviction. One of my more psychotically organized patients told me after several months that he believed that if I really wanted to help him, I would see him for free, and that any other basis for our relationship was corrupt. He was cooperating with me, he explained, because maybe if he could work his way enough into my affections, I would treat him simply out of love and thereby heal his deep conviction of unlovability. This kind of thinking in symbiotically preoccupied people is far from rare and has to be addressed directly. “Analyzing” it as one would do with a neurotic-level person will not be helpful because the belief is syntonic, not a buried vestige of infantile forms of thought.
Hence, if one is asked about the fee by a patient with these fantasies, one might say something like, “I charge what I do because this is the way I earn my living, helping people with emotional problems. Also, I have learned that when I charge less than this, I find myself feeling resentful, and I don’t believe I can be fully helpful when I’m in a state of resentment.” This is not only useful education about how the world works and about the essentially reciprocal nature of psychotherapy—which is in itself corrective to the more fused, enmeshed conceptions of relationship held by more disturbed people—but it is also emotionally honest and will consequently be received with relief even if the patient still thinks the fee is unnecessary or too high.
My own style with most psychotic-level people is quite self-disclosing. I have been known to talk about my family, my personal history, my opinions—anything to put the person at ease with me as an ordinary human being. Such an approach is controversial; not every therapist is temperamentally comfortable with exposure. It also has certain hazards, not the least of which is that some aspect of the therapist’s revealed person will incite a psychotic response in the patient. My rationale lies in the contrast between symbiotically organized people and more individuated ones. The former have such total, encompassing transferences that they can only learn about their distortions of reality when reality is painted in stark colors in front of them, whereas the latter have subtle and unconscious transferences that may surface only when the therapist is more opaque.
The terror of the patient that he or she is in the hands of a powerful, distant, and perhaps persecutory Other is so great that the benefits of being more open may outweigh the risks. And if some revelation provokes a psychotic response, it can be addressed; nondisclosure certainly provokes its share of psychotic upset anyway. In fact, occasional disasters are inevitable in work with more disturbed people and cannot be avoided by the “right” technique. Once I sent a paranoid young man into a full-scale delusion about my intent to murder him because I absentmindedly swatted a bug (“You killed a living thing!”) in his presence.
Another way one may have to demonstrate basic concern, and thereby trustworthiness, is by extending oneself to help in a more specific, problem-solving way than would be warranted in psychotherapy with healthier persons. Advice is ordinarily not given to healthier clients, as it implicitly infantilizes a person with a sense of agency. Karon and VandenBos (1981) discuss the value of practical advice to the patient about counteracting insomnia. One may have to take a position on the patient’s behalf on certain matters. For instance, “I think it’s important that you go to your sister’s funeral. I know it won’t be easy, but I’m afraid if you avoid it you’ll always fault yourself, and you won’t have another chance. I’ll be here afterward to help you cope with any upset you feel.” One may have to advocate for the patient with agencies and social authorities.
The reader will have picked up by now that with psychotic-level people one must relate in a more authoritative (not authoritarian) way than with higher-functioning patients. By behaving like a professional expert but a human equal, the therapist can make frightened clients feel safer. The egalitarian tone is nonhumiliating; the sense of authority reassures them that the therapist is strong enough to withstand their fantasied destructiveness. Naturally, the issues on which one takes an authoritative stand must be ones in which the therapist is genuinely confident. Eventually, as they progress in treatment, even very disturbed people will develop enough security in the relationship to express a difference of opinion, and the therapist can take pride in having fostered the evolution of some genuine psychological independence.
Education
A related aspect of supportive therapy is the therapist’s educative role. Individuals in the psychotic range have areas of great cognitive confusion, especially about emotions and fantasies. Older research into family dynamics in schizophrenia (Bateson et al., 1956; Lidz, 1973; Mischler & Waxier, 1968; Singer & Wynne, 1965a, 1965b) suggest that many psychotic people grew up in systems in which baffling, paralyzing emotional language was used. Family members may have talked about love while acting hatefully, claimed to represent the client’s feelings while unwittingly distorting them, and so forth. As a result, psychosis-prone people often need explicit education about what feelings are, how they are natural reactions, how they differ from actions, how everyone weaves them into fantasies, and how universal are the concerns that the psychotically organized person believes constitute his or her idiosyncratic and warped drama. In many vulnerable people, feelings are not so much unconscious as they are fundamentally unformulated (D. B. Stern, 1997).
One component of the educative process is normalization. The active solicitation of all the client’s concerns and then the reframing of frightening thoughts and feelings as natural aspects of being an emotionally responsive human being are vital to work with more disturbed people. For example, a psychotically bipolar woman became agitated on finding herself admiring my legs as I opened a window; she worried that this meant she was a lesbian. With a less fragile person, I would have asked her to associate to that worry, assuming that her anxiety about sexual orientation was tolerable and would lead to interesting discoveries about disowned aspects of herself. With this woman, however, I remarked warmly that I felt complimented (she looked frightened, as if expecting me to be horrified by the prospect of her attraction), and I went on to say that as far as I could tell on the basis of her history she was not essentially a lesbian, although everyone has some sexual feelings toward people of both genders, and that the only way she might differ from others in having noticed this idea in herself is that some people have a knack for automatically keeping such perceptions unconscious. I recast her worry as being another instance of her greater sensitivity to her inner life and to emotional subtlety than most people have, and I reiterated that my role with her included my trying to help her become comfortable with the fact that she was often in touch with aspects of universal human psychology that many people keep out of awareness.
In this work, one draws on accumulated clinical wisdom, generalizing to the patient what therapists have learned about human psychology. Early conceptions of psychosis as a state of defenselessness, contrasting with the overdefendedness of neurotic people, contributed to the development of this difference in technique. (We now understand psychotic-level people as having defenses, but very primitive ones that cannot be analyzed without making the client feel bereft of one of his or her few means of feeling less frightened.) Psychotically inclined people become traumatically overstimulated by primary process material and often can reduce their upset from that material only by having it normalized.
For example, a young man I treated briefly for a psychotic reaction to his father’s death confessed that he sometimes believed that he had become his father: his self had died, and his father had taken over his body. He was having recurrent dreams in which monsters pursued him, turned into his father, and tried to kill him, and he was genuinely terrified that the dead man, who had been a difficult and punitive parent in life, was capable of invading his body from the grave. I assured him that this was a natural though not always conscious fantasy that people have after bereavement, told him he could expect to lose that feeling as the mourning period progressed, and explained that his belief that his father inhabited his body was expressing numerous natural responses to the death of a parent. First, it indicated denial that his father was dead—a normal phase of grief; second, it expressed his own survivor guilt, handled by the fantasy that he rather than his father had died; third, it was an attempt to reduce anxiety, in that if his father was in his body, he was not somewhere else planning to murder his son for the sin of outliving him.
This kind of active, educative stance is vital to the emotional equilibrium of a psychotically anxious person because it mitigates the terror that he or she harbors about going crazy. It also welcomes the client into a world of greater psychological complexity and implicitly invites him or her to “join the human race.” Many people with psychotic tendencies have been placed since early childhood in the sick role, first by their families and later by other social systems that define them as oddballs. Consequently, they come to treatment expecting that a therapist will be similarly impressed by their lack of sanity. Interventions that embrace rather than stigmatize are relievingly corrective and can have a self-fulfilling effect. In educative conversations it is more important to convey a general expectation of eventual understanding than to be completely accurate. Since one never does understand perfectly, it is also important to modify one’s authoritative tone with some qualifications about such explanations being a “best guess” or “provisional understanding.”
This style of intervention was first developed for children whose primitive preoccupations coexisted with fears of regression (B. Bornstein, 1949) and has variously been called “reconstruction upward” (Greenson, 1967; R. M. Loewenstein, 1951), “interpreting upward” (Horner, 1990), and simply “interpreting up.” These phrases imply a contrast with the kind of interpretation helpful to neurotic-level patients, by which one works “from surface to depth” (Fenichel, 1941), addressing whatever defense is closest to conscious understanding. In interpreting up, one directly plumbs the depths, names their contents, and explains why that material would have been set off by the patient’s life experiences. Oddly, this essential aspect of psychodynamic work with frightened patients is seldom spelled out in books on technique.
Identification of Triggers
A third principle of supportive therapy involves attention to feelings and stresses rather than defenses. For example, when working with more disturbed people we frequently have to sit through extended paranoid tirades when the patient is upset. It is tempting, in the face of an assault on the senses of a psychotic degree of fear and hatred, to try to explain away the projective defense or to contrast the client’s distortions with the therapist’s view of reality, but either of those strategies is likely to make the patient worry that the therapist is secretly in league with the persecutors. Yet just witnessing a disorganized psychotic outburst seems hardly therapeutic. So what is one to do?
First, one waits until the patient pauses for breath. It is better to wait too long than not long enough (this may mean sitting quietly and nodding sympathetically for most of the session), reminding oneself that at least the patient now trusts you enough to express uncensored feelings. Second, one makes a comment something like “You seem more upset than usual today,” with no implication that the content of the upset is crazy. Finally, one tries to help the client figure out what set off this intensity of feeling. Often, the source of the distress is only peripherally related to the topic of the rant; it may be, for example, some life circumstance involving a separation (the client’s child is entering kindergarten, or a brother announced his engagement, or the therapist mentioned vacation plans). Then one empathizes actively with how disconcerting separations can be.
In this process, one must sometimes tolerate the odd role of accepting what the therapist sees as the person’s distortions, and occasionally, as most strikingly dramatized in Robert Lindner’s (1955) entertaining essay, “The Jet-Propelled Couch,” one must even actively accept the patient’s frame of reference. Sometimes only in being joined this way will the patient feel sufficiently understood to accept later reflections (cf. Federn, 1952). The school of “Modern Psychoanalysis” (Spotnitz, 1985) has raised this style of therapy to a high art. Originally labeled “paradigmatic psychoanalysis” (Coleman & Nelson, 1957), this approach has a lot in common with later “paradoxical intervention” techniques favored by some family systems therapists. Joining is not as cynical as it may seem, as there is always some truth in even the most paranoid constructions.
Some examples of joining: A woman storms into her therapist’s office, accusing him of involvement in a plot to kill her. Rather than questioning the existence of the plot or suggesting that she is projecting her own murderous wishes, the therapist says, “I’m sorry! If I’ve been connected with such a plot, I wasn’t aware of it. What’s going on?” A man falls into a miserable silence and when prodded confesses that he is responsible for the carnage in the Middle East. The therapist responds, “It must be terrible to carry that burden of guilt. In what way are you responsible?” Or a patient confides that the therapist’s colleague and friend, the ward nurse, tried to poison him. The therapist says, “How awful. Why do you suppose she is mad enough at you to try to kill you?”
Note that in all these instances, the therapist does not express agreement with the patient’s interpretations of events, but neither does he or she inflict the wound to the patient’s pride of dismissing them. And most important, the therapist invites further discussion. Usually, once the client lets off enough steam, a less terrifying understanding will gradually replace more paranoid attributions. Sometimes the therapist can assist this process by gently asking about alternative explanations of the patient’s perceptions, but only after giving the client time for self-expression. Often by the end of the session, the patient feels reoriented and leaves in a more composed state.
By now it is probably evident how different psychoanalytic work with psychotic-level people is from therapy with neurotic individuals. Not everyone has the temperament to do this kind of work comfortably—it is facilitated by both counterphobia and a sense of personal power that is alien to the personalities of many therapists; those without such qualities may be better off in other areas of mental health service. One of the most important things to learn in one’s training is which kinds of people one enjoys and treats effectively, and which kinds one should refer.
Therapy with psychotic and potentially psychotic people has different aims and satisfactions from therapy with healthier clients. Despite some prejudice against it in the name of cost cutting (a position I see as comparable to arguing that cancer patients should receive aspirin), psychotherapy with psychotic people is effective (Gottdiener, 2002, 2006; Gottdeiner & Haslam, 2002; Silver, 2003) and may be gratefully received (see, e.g., A Recovering Patient, 1986; Saks, 2008). By the mid-1990s, cognitive-behavioral therapists (e.g., Hagarty et al., 1995) were describing effective work with psychotic patients characterized by education, support, and skills training—an approach that in practice seems pretty similar to psychoanalytic supportive treatment. Therapy with the severely disturbed can be lifesaving; expertise in it is much rarer than expertise treating healthier people; it is intellectually and emotionally stimulating; it nourishes one’s creativity. At the same time, it can be depleting, confusing, and discouraging, and it inevitably confronts one with the limits on one’s capacities to effect dramatic transformations.
In closing this section, I offer the following rules from Ann-Louise Silver (2003, p. 331) for working with people with psychoses:
THERAPY WITH BORDERLINE PATIENTS
The term “borderline,” used as a level of organization, encompasses great diversity. Not only is a depressive person with borderline character structure quite different from a narcissistic or hysterical or paranoid borderline person, but there is a wide range of severity within the borderline spectrum, extending from the border with the neuroses to the border with the psychoses (Grinker et al., 1968)—somewhat arbitrary borders to begin with. The closer a person’s psychology is to neurotic, the more positively he or she will respond to a more “uncovering” kind of treatment, whereas clients who border on psychosis will react better to a more supportive style. We are not unidimensional; every neurotic-level person has some borderline tendencies, and vice versa. But in general, people with a borderline level of personality organization need highly structured therapies. In what follows I mention some cognitive and behavioral approaches along with psychodynamic ones, as in practice, there are significant similarities across treatment approaches.
The aim of therapy for people with borderline psychologies is the development of an integrated, dependable, complex, and positively valued sense of self. Along with this goes the evolution of a capacity to love other people fully despite their flaws and contradictions and the ability to tolerate and regulate a wide range of emotions. A gradual movement from capricious reactivity to steady reliance on one’s perceptions, feelings, and values is possible for borderline people, despite the difficulties they present to therapists, especially in the early part of treatment.
Theorists with different explanatory constructions about borderline personality structure have emphasized different aspects of treatment. Originally, it was widely seen as a developmental arrest (e.g., Adler & Buie, 1979; Balint, 1968; Blanck & Blanck, 1986; Giovacchini & Boyer, 1982; Masterson, 1976; Meissner, 1988; Pine, 1985; Searles, 1986; Stolorow, Brandchaft, & Atwood, 1987) in interaction with a constitutional temperament (Gabbard, 1991; Kernberg, 1975; M. H. Stone, 1981). More recently, it has been viewed as a result of trauma (e.g., Briere, 1992; C. A. Ross, 2000), especially attachment trauma (Blatt & Levy, 2003). These theories are not mutually exclusive; “borderline personality” is a complex concept and probably multiply determined.
Although the generalizability of most empirical studies of therapy for people with borderline psychologies is limited to those meeting DSM criteria for BPD, research on treatments for borderline conditions has been encouraging and has given empirical support to several approaches. Linehan’s dialectical behavior therapy (e.g., 1993) is often cited as “the” evidence-based therapy for BPD, but there have also been methodologically rigorous studies (e.g., Bateman & Fonagy, 2004; Levy et al., 2006) of both Fonagy’s mentalization-based therapy (MBT) and Kernberg’s transference-focused psychotherapy (TFP)—the latter being the manualized version of the “expressive therapy” denoted in this book’s first edition. Recently, Young’s schema-focused therapy (SFT—whence the three-letter acronym rule?!) has been empirically tested (van Asselt et al., 2008). Differing views of etiology and differing therapy traditions naturally lead to different treatments, and there is sufficient controversy in the literature on treating borderline clients that a few paragraphs cannot address all the divergences. Still, it is remarkable how much practical consensus, despite varied theoretical languages and etiological assumptions, there is about overall principles of treatment, some of which I summarize here (cf. Paris, 2008).
Safeguarding Boundaries and Tolerating Emotional Intensity
Although borderline patients have more capacity to trust than psychotically organized people do, and thus rarely require the therapist’s continual demonstration that they are safe in the consulting room, they may take up to several years to develop the kind of therapeutic alliance that a neurotic client may feel within minutes of meeting the therapist. By definition, the borderline client lacks an integrated observing ego that sees things more or less as the therapist does; instead, he or she is subject to shifting chaotically between different ego states, with no capacity yet for putting disparate attitudes together. Whereas the psychotic person tends to fuse psychologically with the clinician and the neurotic one to keep a clear separate identity, the borderline person alternates—confusingly to self and others—between symbiotic attachment and hostile, isolated separateness. Both states are upsetting: One raises the specter of engulfment, the other of desertion.
Given this instability of ego state, a critical dimension of treatment with borderline patients is the establishment of the consistent conditions of the therapy—what Langs (1973) has called the therapeutic frame. This includes not only arrangements as to time and fee but may also involve numerous other decisions about the boundaries of the relationship that rarely come up with other clients. All the mainstream therapies for BPD have mechanisms (contracts, consequences, rules of the treatment, ways to limit self-destructiveness) to maintain treatment via explicit boundary conditions. One can be more flexible with either neurotic- or psychotic-level patients.
Common concerns of borderline clients include “Can I call you at home?” “What if I’m suicidal?” “Will you break confidentiality for any reason?” “How late can I cancel a session without being charged?” “Can I sleep on the floor in your waiting room?” “Will you write my professor and say I was too stressed out to take the exam?” Some of these issues are articulated as questions; others come up in enacted form (e.g., one finds the client sleeping on the waiting room floor). The possibilities for boundary struggles are limitless with people in the borderline range, and the critical thing for the therapist to know is not so much what conditions should be set (these may vary according to the patient’s personality, the therapist’s preferences, and the situation) but that they must be set, consistently observed, and enforced by specific sanctions if the patient fails to respect them. It is disturbing to people with separation–individuation issues to be indulged rather than contained, much as it is to adolescents whose parents do not insist on responsible behavior. Without explicit limits, they tend to escalate until they find the ones that have been unstated.
Borderline-level clients will often react with anger to the practitioner’s boundaries, but two therapeutic messages will be received nonetheless: (1) the therapist regards the patient as a grown-up and has confidence in his or her ability to tolerate frustration, and (2) the therapist refuses to be exploited and is therefore a model of self-respect. Often, the histories of people in the borderline range give evidence of their having had ample exposure to the opposite messages; they have been indulged when regressed (and usually ignored when acting more mature), and they have been expected to be exploitable and allowed to exploit.
When I first began practicing, I was struck by the amount of deprivation and trauma in the histories of borderline clients. I tended to see them as hungry and needy more than as aggressive and angry and I would extend myself beyond my usual limits in the hope of making up for their hardships. I learned that the more I gave, the more they regressed, and the more I became resentful. I eventually learned to adhere to my frame, however harsh it might seem in the moment. I would not let sessions run over, for example, even when the patient had just gone into a state of intense grief. Instead, I learned to end the session gently but firmly at the regular time and then to listen in the next meeting for the person’s anger at having been kicked out. When borderline patients could tell me off about my rigid, selfish rules, I noticed that they did a lot better than when I was trying to put them into a state of gratitude for my generosity—an inherently infantilizing position.
Therapists new to work with borderline patients often wonder when all the preconditions of therapy will finally be worked out, a working alliance created, and the actual therapy begun. It may be painful to realize that all the work with the conditions of treatment is the therapy. The beginner wonders when the borderline patient will “calm down.” The intensity of borderline patients will characterize the work throughout, and it is critical that the therapist be able to tolerate or “contain” that intensity, even when it involves verbal attacks on the therapist (Bion, 1962; Charles, 2004). Once a neurotic-type alliance is achieved, the patient by definition will have taken a giant step developmentally. It is disconcerting to spend so much time on boundary issues, especially when they stimulate over-the-top reactivity, with people who are often bright, talented, and articulate, and with whom one naturally wants to get on to other things. Niggling over limits is scarcely what we envisioned as constituting therapy when we went into this field. Thus, people working with their first borderline clients may suffer periodic fits of doubt about their competence.
Even for patients who are attracted to psychoanalysis and who want to “go deep,” face-to-face therapy is generally better for borderline clients. Although not as subject to overwhelming transferences as psychotically vulnerable people are, they have more than enough anxiety without the therapist’s being out of their line of vision. Seeing the therapist’s facial affect may also be critical for the recovery of more difficult patients. In videotaped therapies with clients who had had prior treatment failures, Krause and his colleagues (e.g., Anstadt, Merten, Ullrich, & Krause, 1997) found that irrespective of the therapist’s orientation, improvement correlated with the client’s seeing a “nonmatching” affect on the therapist’s face. For example, when the client’s face showed shame, the therapist’s might show anger that someone had shamed the client; when there was fear on the client’s face, the therapist’s might show curiosity about the fear). Also, again because intensity needs no encouragement in borderline clients, only unusual circumstances (such as the need for increased support during withdrawal from an addiction) would warrant scheduling borderline clients at a frequency of more than three times a week, as in classical analysis.
Voicing Contrasting Feeling States
A second thing to attend to with borderline clients is one’s way of speaking. With neurotic patients, one’s comments may be infrequent, with the goal of being impactful when they occur (“less is more”). One can talk with healthier clients in a pithy, emotionally blunt way (Colby, 1951; Fenichel, 1941; Hammer, 1968), noting the underside of some conflict in which the client is aware of only one feeling. For example, a woman in the neurotic range may be gushing about a friend with whom she is in a somewhat competitive situation in a way that suggests she is not in touch with any negative affects. The therapist may say something along the lines of “But you’d also like to kill her.” Or a man may be going on about how independent and free spirited he is; the therapist may comment, “And yet you are always worried about what I think of you.”
In these cases, the respective neurotic clients will know that the therapist has revealed a part of their subjective experience that they had been keeping out of consciousness. Because they can appreciate that the clinician is not being reductive, is not claiming that the disowned attitude is their real feeling and that their conscious ideas were illusory, they may feel expanded in their awareness as a result of the interpretation. They feel understood, even if slightly wounded. But borderline clients to whom one talks this way will feel criticized and diminished, because unless the statement is phrased differently, the main message that will be received is “You’re utterly wrong about what you really feel.” This response derives from their tendency to be in one or another self-state rather than in a frame of mind that can experience and tolerate ambivalence and ambiguity.
For these reasons, it is common for beginning therapists to think they are expressing solicitous understanding and to find that the borderline person reacts as if attacked. One way around this problem is to appreciate that the borderline client lacks the reflective capacity to process an interpretation as additional information about the self, and that consequently one must provide that function within the interpretation. So one would have a better chance of being heard as empathic if one said, “I can see how much Mary means to you. Is it possible, though, that there is also a part of you—a part that you would not act upon of course—that would like to get rid of her because she’s in some ways in competition with you?” Or, “You certainly have established that you have a very independent, self-reliant streak. It’s interesting that it seems to coexist with some opposite tendencies, like a sensitivity to what I think of you.” Such interventions lack the punch and beauty of an economy of words, but given the particular psychological problems of borderline people, they are much more likely than more trenchant formulations to be taken in as intended.
Interpreting Primitive Defenses
A third feature of effective psychoanalytic therapy with patients in the borderline range is the interpretation of primitive defenses as they appear in the relationship. This work is not different in principle from ego psychological work with neurotic-level people: one analyzes defensive processes as they appear in the transference. But because the defenses of a borderline person are so primal, and because they may come across as entirely different in different ego states, the analysis of their defenses requires a special approach.
With borderline clients, it is rarely helpful to make “genetic” (historical) interpretations, in which a transference reaction is linked to feelings that belonged to a figure from the patient’s past. With neurotic-level clients, one can get a lot of mileage out of a comment like “Perhaps you’re feeling so angry at me because you’re experiencing me as like your mother.” The patient may agree, notice the differences between the therapist and the mother, and get interested in other instances in which this association might have been operating. With borderline patients, reactions can vary from “So what?” (meaning, “You’re a lot like my mother, so why wouldn’t I react that way?”) to “How’s that supposed to be useful?” (meaning, “You’re just talking party-line shrink talk now. When are you going to get down to helping me?”) to “Right!” (meaning, “Finally you’re getting the picture. The problem is my mother, and I want you to change her!”). Such reactions can leave a beginning therapist bewildered, disarmed, and deskilled, especially if genetic interpretations were a helpful aspect of the therapist’s personal experience in psychotherapy.
What can be interpreted with borderline clients is the here-and-now emotional situation. For example, when anger permeates the therapeutic dyad, it is likely that the patient’s defense is not displacement or straightforward projection, as it would be in the above example of the neurotic person with the mother transference; instead, the patient may be using projective identification. He or she is trying to unload the feeling of “bad me” (Sullivan, 1953) and the associated affect of rage by putting them on the therapist, but the transfer of image and affect is not “clean”; the client retains feelings of badness and anger despite the projection. This is the painful price paid by the borderline person, and inevitably shared by the therapist, for inadequate psychological separation.
Here is a critical difference between borderline clients and both psychotic and neurotic ones. The psychotic client is sufficiently out of touch with reality not to care whether a projection “fits.” The neurotic person has an observing ego capable of noticing that he or she is projecting. Borderline patients cannot quite succeed in getting rid of the feeling being projected. They cannot take an attitude of indifference about how realistic the projected material is because unlike psychotics, they have intact reality testing. And they cannot relegate it to the unconscious part of the ego because, unlike neurotics, they switch states rather than using repression. So they keep feeling whatever is projected, along with the need to make it fit so that they will not feel crazy. The therapist gets the client’s anger (or other strong affect), and as the client tries to make the projection fit by insisting that he or she is angry because the therapist is hostile, also begins to feel a rage at being misunderstood. Soon, the therapist is hostile. Such transactions account for the bad reputation borderline clients have among many mental health professionals, even though they are not always unpleasant people and are usually responsive to good treatment.
The kind of interpretation that may reach a borderline person in such a predicament is something like “You seem to have a conviction that you are bad. You’re angry about that, and you’re handling that anger by saying that I am the one who is bad, and that it’s my anger that causes yours. Could you imagine that both you and I could be some combination of good and bad and that that wouldn’t have to be such a big deal?” This is an example of a here-and-now confrontation of a primitive defense. It represents an effort by the therapist, one that will have to be repeated in different forms for months at best, to help the patient shift from a psychology in which everything is black or white, all or nothing, to one in which diverse good and bad aspects of the self, and a range of emotions, are all consolidated within an overall identity. This kind of intervention does not come easily to most people, but fortunately, it improves with practice.
Getting Supervision from the Patient
A fourth dimension of work with borderline clients that I have found valuable is asking the patient’s help in resolving the either/or dilemmas into which the therapist is typically put. This technique, by which one in effect gets the patient to be one’s supervisor, relates to the all-or-nothing way in which borderline people construe things. They tend to evoke in a therapist the sense that there are two mutually exclusive options for responding to a given situation, and that both would be wrong, for different reasons. Usually there is a test involved (Weiss, 1993) in which if the therapist acts one way, he or she will fail according to one polarity of the patient’s conflict, and if the other alternative is chosen, there will be an equal failure of the opposite sort.
For example, I once treated a 22-year-old man with an alcoholic father, who seemed not to notice his existence, and an overinvolved, anxious, intrusive mother, who took over her son’s life to the extent of picking out his clothes each day. (I had met the parents and was thus in a position to know more about the real people who had influenced this man than one often knows with borderline clients.) As the therapy progressed, this patient would stop speaking for increasing amounts of time during our sessions. At first, it seemed as if he simply needed the space to get his thoughts together, but as the silences stretched out to 15 and then 20 minutes at a time, I felt that something less benign was going on and that I would be remiss in not addressing it.
If this patient had been in the neurotic range, I would have reminded him of his agreement to keep talking about whatever was on his mind and explored with him what was getting in the way of his willingness to do that; in other words, I would have done simple resistance analysis. But with this young man I could feel that something more primitive was going on, involving counterpoised terrors of engulfment and abandonment, and I knew we did not have enough of a working alliance for me to approach his silence as I would with a healthier person. If I remained quiet, I was fairly sure he would feel hurtfully neglected, as by his father; yet if I spoke, I suspected he would experience me as taking over, like his mother. My quandary at this juncture probably mirrored his sense that he would be damned if he did talk and damned if he didn’t.
After trying for a while to figure out which intervention would be the lesser evil, it occurred to me to ask him to help me solve the problem. At least that way, whatever came out of our interaction would have an element of his autonomy in it. So I asked him how he wanted me to respond when he went into a long silence. He answered that he guessed he wanted me to ask him questions and to draw him out. I then commented that I would be glad to do that, but that he should know that I might be way off base in my pursuit of what he was thinking about since when he was quiet, I had no idea what was on his mind. (There had been evidence in the dreams and fantasies he had reported, while still talking, that he believed that others, like the fantasied omniscient mother of early infancy, could read his mind. I wanted to send a contrary and more realistic message.)
He brightened up and on that basis changed his mind, deciding I should wait until he felt ready to talk. He then came for three sessions in a row in which he greeted me cheerfully, sat down, said nothing for 45 minutes, then departed politely when I said our time was up. Interestingly, whereas I had been in a miserable internal state before I got him to supervise me in this way, I was at peace with his silence afterward. A couple of years later, he was able to tell me that my willingness to take his direction marked the beginning of his ability to feel like a separate person in the presence of someone else. This approach thus reduces the therapist’s immediate uneasiness; more important, it models an acceptance of uncertainty, affirms the patient’s dignity and creativity, and reminds both parties nonjudgmentally of the cooperative nature of the work.
It is important in such interventions to talk from the perspective of one’s one own motives rather than the patient’s inferred motives. The value of “I-statements” is as great here as when one argues with a lover or friend. There is a huge difference between being on the receiving end of “You’re putting me in a bind” or “You’re setting it up so that whatever I do is wrong” and hearing “I’m trying to do right by you as your therapist, and I find myself feeling in a bind. I worry that if I do X, I’ll be unhelpful in one direction, and if I do Y, I’ll disappoint you in another.”
Promoting Individuation and Discouraging Regression
People with borderline psychologies need empathy as much as anyone else, but their mood changes and ego-state fluctuations make it hard for clinicians to know how and when to convey it. Because they tend to evoke loving countertransferences when they are depressed or frightened, and hateful ones when they act antagonistically, one may find oneself inadvertently rewarding them for regression and punishing them for individuation. Therapists trained to work with neurotic-level patients by fostering a contained regression may, out of habit, evoke some of the least healthy responses of borderline clients. An appreciation of their psychology helps us to act somewhat counterintuitively; that is, to be relatively nonresponsive to states of subjective helplessness and to show appreciation for assertiveness—even when it takes the form of angry opposition.
As I mentioned in Chapter 3, Masterson (1976) noted that when borderline clients, whose mothers he saw as having rewarded their clinging, are in a regressed, dependent relationship, they feel safe. When alone, they suffer an anguished desperation that he called “abandonment depression.” His observations comport with those of researchers in attachment (e.g., M. Main, 1995), who have related some insecure attachment patterns to an anxious, autonomy-impeding mothering style. Because separateness is eventually empowering, Masterson urged therapists to behave with borderline patients conversely from the way their mothers purportedly had; namely, to confront regressive and self-destructive behaviors actively (e.g., “Why would you want to pick up men at bars?”) and to endorse empathically any efforts toward autonomy and competence (e.g., “I’m glad to see you can tell me off when I make you angry”). He advised us not to reward the clinging that gives the patient no basis for self-esteem, and to take pains to see the forward-moving, adaptive elements in even aggravating manifestations of self-assertion. At first such a posture may feel a bit contrived, but as one sees clients respond, it may become more integrated and authentic to one’s therapeutic style.
Interpreting during Quiescence
Pine (1985) contributed an important dictum to our literature on working with clients who struggle over separation and individuation: “Strike when the iron is cold.” With many neurotic-level people, the best time to make interpretations is when the patient is in a state of emotional arousal, so that the content of the therapist’s observation is not intellectualized and the affective power of the issues being addressed is unmistakable. With borderline clients, the opposite consideration applies, because when they are in a state of heightened emotionality, they are too upset to take anything in. One can comment on what happened in their rage or panic or desperate regression, but only after that state is over and they are internally reassured of having recovered from such a disturbing intensity of feeling.
Thus one might say to a borderline patient, “I was thinking. What you’re talking about now, your tendency to feel murderous envy and to attack people when you’re in that state . . . was something like that part of your outburst at me last week? It felt as if whatever I offered you, you had to destroy it.” In a state of emotional repose, a borderline client may be willing—even relieved—to hear that the therapist has named such a dynamic and tried to understand it. But in a state of intense feeling, the patient may receive such a comment not only as condemnation but also as an effort to dismiss passionately held attitudes as if they were contemptible. Telling someone in the throes of an envious rage that he or she is trying to destroy the therapist may increase the person’s helpless fury and shame over having such raw impulses. Talking about it later may be fruitful.
Respecting Countertransference Data
A final aspect of the implications of a borderline diagnosis for psychotherapy concerns the central role of the therapist’s understanding of countertransference. Much more than neurotic-level people, borderline clients communicate through powerful and unverbalized affect transmission, probably via the early right-brain-to-right-brain communication characteristic of parents and infants (Schore, 2003a). By this I mean that even though they may talk freely in therapy, the most vital communications they send are often not in the content of their words but in the “background music” of their emotional state. The intuitive, affective, and imaginal responses of therapists when sitting with a borderline patient can often provide better data about the essence of what is going on between the two people than either cognitive reflection on the content of the patient’s communication or recourse to ideas on theory and technique.
When one suddenly feels bored, or in a rage, or panicky, or overwhelmed with the wish to rescue, or diverted by sexual images, something is probably going on that says something important about the client’s internal state. For example, a paranoid man, in treatment with a young woman, is in a state of self-righteous indignation about mistreatment by some authority. The therapist notices that she feels weak, small, fearful of the patient’s criticism, and distracted by fantasies of being attacked. She should consider the possibility that what she is feeling is a split-off, disowned part of the patient that is being projected into her in an almost physical way. If that idea seems reasonable after some reflection, it may be therapeutic (to both parties!) for her to say something like “I know that you are in touch with feeling angry and energized, but I think there may also be a part of you that feels weak, anxious, and fearful of being attacked.”
This area of the informational value of countertransference is a tricky one. Not every passing thought and emotion that one feels in the presence of a borderline patient was “put” there by the patient. At our worst, we can do harm in the name of concepts like projective identification and co-construction; I have even heard of therapists getting into hassles with borderline clients over whose “fault” it is that the therapist is having strong reactions. I do not want to feed anyone’s rationalizations in this direction. Decades of clinical work suggests that countertransference, like transference, is a mixture of internally generated and externally stimulated material, sometimes weighted more in one direction, sometimes more in the other (Gill, 1983; Jacobs, 1991; Roland, 1981; Sandler, 1976; Tansey & Burke, 1989). In our therapeutic role we should be insightful about our own dynamics and take responsibility for our reactions, even when they are being provoked by a patient’s incursions on our equanimity. And even interpretations that we feel sure are valid should be offered in a way that invites clients to take issue if they disagree.
The extreme converse attitude, that one should regard countertransference as solely one’s “own stuff,” can also be inimical to clinical progress. Some psychoanalytic supervisors put so much stress on their students’ understanding of their own dynamics that they foster a distracting degree of self-consciousness. No emotional energy is left over for reflecting on what can be learned about the patient from one’s responses. A kind of navel gazing comes to substitute for real relatedness, and people of talent and compassion become reluctant to trust what are often excellent natural instincts because they fear they are acting something out. If in the above example, for instance, the therapist had handled her countertransference with self-examination alone, reflecting on how she has a vulnerability to feeling small and frightened in the presence of angry men who remind her of her critical father, there would be little to do therapeutically with such an insight. It might help her to contain defensive reactions, an achievement not to be disdained, but it would not guide the therapist toward what she could actively do to help the patient. The worst thing that can happen if we mistake our own feelings for a client’s is that we will be wrong, and if interpretations are made in a tone of hypothesis rather than pronouncement, the patient will be glad to point out our errors.
Different writers emphasize different aspects of tone with borderline patients. My own style, one that fits my own personality, is to be more emotionally “real” with borderline patients than with neurotic-level ones. Trying to act “neutral” with them, especially when they are self-harming, tends to sound stiff and false. For example, a therapist has been working for weeks to reduce a young woman’s tendency for self-harm and is just beginning to see progress. Then the client comes in, smiles coyly, and says, “Well, I know we’ve been working on this, but I cut myself again.” Or “I know you think I should always use condoms, but I did have unprotected sex with a guy this week that I met in a bar. I don’t think he’s HIV positive, though; he seems nice. Are you angry at me?” At such points, a hot rage may start to burn in one’s gut.
I have learned that it is not helpful to say, as if one could be dispassionate, “So tell me about your fantasies about my reaction,” as one might with a neurotic-level person who had acted out and feared disapproval. Instead, it is better to say something like “Well, you know it’s my job to try to help you be less self-destructive, so when I hear that you’ve been more self-destructive, it does get to me. What’s it like for you when I get irritated at your behavior?” As Karen Maroda (1999) has emphasized, it does not usually close the patient down when the therapist is able to show some emotion—especially borderline patients, who know they are difficult.
A book on diagnosing individuals takes by definition a one-person perspective of trying to understand what is consistent about the patient in any relationship. And I have argued, contra some relational arguments, that this is a valuable perspective (cf. Chodorow, 2010). But in treatment, it is important to remember the psychological equivalent of the Heisenberg principle: When we are observing something, we are part of what is being observed. When we are with a patient, we are relating to a person as he or she exists in the situation of being with us. What we are learning about the emotional brain, about right-brain-to-right-brain communication, about the intersubjective nature of all interaction, reveals that the image of any person as an autonomous individual whom one is “objectively” observing is a fiction (Wachtel, 2010). The fact that all relationships are co-constructed means that one must own one’s own contribution to whatever goes on. Attunement to that fact may be particularly important with borderline clients, who struggle with humiliation and may be relieved by the therapist’s sharing responsibility for what goes on in the dyad.
This concludes what I can say in a primer about implications of developmental level for treatment. I have only scratched the surface. If this were a treatise on technique per se, each level would merit at least a chapter, or better yet, would be the subject of its own book. And as if the above issues were not complex enough, let me now introduce the topic of the interaction of developmental and typological categories of personality structure and their complex relationship.
INTERACTION OF MATURATIONAL AND TYPOLOGICAL DIMENSIONS OF CHARACTER
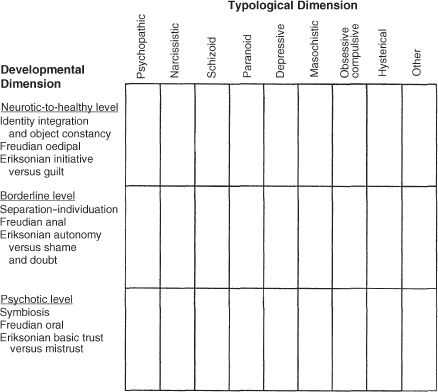
Figure 4.1 sets out visually the ways in which many analytically oriented therapists implicitly map out their patients’ personality structures. The developmental axis, though divided into the three main categories of organization, is actually a continuum, with differences of degree that gradually become great enough to warrant conceptualization as differences of kind. We all fluctuate in terms of our maturational state; under enough stress an optimally healthy person can have a temporary psychotic reaction; and even the most delusional schizophrenic has moments of utter lucidity. Many of the typological categories that cross the maturational axis should be familiar, even though they will not be discussed systematically until later in this book. In Chapters 5 and 6 I cover in detail the concept of defense, since the personality configurations on the typological axis represent the habitual use of one defense or one cluster of defenses.
In every category on the horizontal axis, there is a range of character pathology from the psychotic to the neurotic–healthy areas. Yet people are not evenly distributed along all points of each continuum. Those categories that represent the habitual use of a more primitive defense will “load” more toward the psychotic end of the continuum; paranoid people, for example, who by definition depend on denial and projection, will be more common at the lower rather than at the upper end of the developmental axis. Those typological categories representing reliance on more mature defenses will load more toward the neurotic pole; a greater proportion of obsessional people, for example, will be at the neurotic end of the obsessive dimension than at the psychotic pole. Most character patterns that are maladaptive enough to be considered a DSM personality disorder, rather than just a personality style, are likely to be in the borderline range.
Anyone’s life experience with a diversity of human beings gives evidence that it is possible for someone to have a high degree of ego development and identity integration and still handle anxieties with a primitive defense. Again taking the case of people with significant paranoia, most of us can think of individuals whose personalities are distinctly paranoid but who have good ego strength, clarity about their existence as individuated human beings, an elaborated and consolidated identity, and enduring relationships. They often find a home in professions like detective work or covert operations in which their paranoid tendencies work to advantage. The fact that healthier paranoid people do not usually seek psychotherapy (a fact intrinsically related to their paranoia) does not mean that they are not out there. The frequency with which people seek therapy and thereby get into mental health statistics is not the same across different types of personality because the categories reflect important differences in areas like one’s disposition to trust, inclination to hope, willingness to part with money for nonmaterial benefits, and so forth.
Correspondingly, ordinary life experience also suggests that it is possible for people to rely centrally on a “mature” defense like intellectualization and nevertheless have poor reality testing, inadequate separateness, limited identity integration, and unsatisfying object relationships. Thus, whereas healthier obsessive people may be easier to find than those with psychotic leanings, any intake worker in an inpatient facility has seen people whose penchant for intellectualizing has crossed the line into delusion.
It is often more important clinically to have a sense of a client’s overall developmental level than it is to identify his or her most appropriate typological descriptor. Since flexibility of defense is one aspect of psychological health, people in the higher ranges rarely exemplify one pure personality type. But both areas of assessment are important, as will be exemplified in certain instances of differential diagnosis that I cover in Chapters 7 through 15.
FIGURE 4.1. Developmental and typological dimensions of personality.
SUMMARY
The subject of this chapter has been the implications for therapy of whether a given client is mainly neurotic, psychotic, or borderline characterologically. Neurotic-level people are usually good candidates for either psychoanalysis or traditional exploratory therapies; their ego strength also makes them responsive to many other kinds of intervention.
Patients at a symbiotic–psychotic level usually need supportive therapy, characterized by, among other things, an emphasis on safety, respect, honesty, education, and attention to the effects of particular stresses.
Patients at a borderline level are most helped by modes of working in which boundaries are fastidiously maintained, contrasting ego states named, and primitive defenses interpreted. The patient’s help may be solicited to resolve impasses. Interventions that are useful to borderline patients discourage regression and support individuation. The therapist builds understanding during periods of quiescence and respects information contained in countertransference.
Finally, character structure was diagrammed on two axes in order to illustrate graphically the principle of appreciating both developmental and typological dimensions of personality.
SUGGESTIONS FOR FURTHER READING
The standard text on classical psychoanalysis with neurotic-level people is still Greenson’s The Technique and Practice of Psychoanalysis (1967). Schafer’s The Analytic Attitude (1983) articulates aspects of therapy that conventional books leave out. Among the texts on therapy that try to be generic across levels of character organization, I recommend those by Fromm-Reichmann (1950), Hedges (1992), Pine (1985), Charles (2004), and my own text (McWilliams, 2004). The most readable book on therapy across developmental levels from an object relations perspective is probably Horner’s Psychoanalytic Object Relations Therapy (1991). E. S. Wolf’s Treating the Self (1988) gives a particularly useful self psychology perspective. Good relationally oriented texts include Maroda’s Psychodynamic Techniques (2010) and Safran’s research-based primer (in press).
The best writing I know of about working with psychotic-level patients—and good sources in this area are much scarcer—includes work by Arieti (1955), Searles (1965), Lidz (1973), Karon and VandenBos (1981), Selzer and his colleagues (1989), and Geekie and Read (2009). The text by Alanen and colleagues (2009) is a good overview of psychotherapy with schizophrenia. The long-standing need for comprehensive books on supportive therapy has been filled by Rockland (1992) and Pinsker (1997). For a moving account of recovery from schizophrenia from the patient’s perspective, see the classic I Never Promised You a Rose Garden, by Hannah Green (1964), the pseudonym of the still-healthy Joanne Greenberg, who was treated by Freida Fromm-Reichmann.
The literature on the therapies for borderline personality organization is confusing because of the diversity of approaches to conceptualizing borderline clients. Hartocollis’s (1977) edited volume is useful for the historical context of the concept. Among the more classic psychoanalytic contributions to technique, Masterson’s work, which has the virtue of being gracefully written, is perhaps best summarized in his 1976 book. G. Adler’s (1985) contribution is a readable overview of a more self psychologically influenced way of understanding and treating people in this group.
Kernberg’s research group (Clarkin et al., 2006) has published a comprehensive manual on transference-focused therapy, with emphasis on primitive defenses, especially splitting. Bateman and Fonagy’s Mentalization-Based Treatment for Borderline Personality Disorders (2004) similarly synthesizes knowledge gleaned from a long program of research and practice, with emphasis on cognitive and attachment deficits. Linehan’s cognitive-behavioral work (e.g., 1993), which emphasizes the affect dimension of borderline experience, is accessibly written and clinically useful by therapists of all orientations.