This chapter explores individual supervision as a unique educational structure for psychotherapy education. Such supervision is of paramount importance in the professional formation of the psychotherapist in particular, but it is also important for all mental health practitioners regardless of whether psychotherapy plays a significant role on their professional lives or not (Mohl et al., 1990). Individual supervision as an extended form of case consultation with a focus on both the patient and consultee is also an extremely important (although apparently underutilized) form of continuing professional education for mental health practitioners. The chapter focuses on individual supervision as an educational element for developing competency in psychodynamic psychotherapy but will also address the pros and cons of individual versus group psychotherapy supervision and the similarities and differences between supervision of the psychodynamic therapies and supervision of cognitive-behavioral therapies (CBT).
The chapter begins with a brief historical review of the concept of individual supervision and what makes individual supervision a unique educational structure (Jacobs et al., 1995; Watkins, 1997). Next we focus on establishing the supervisory alliance, clarifications of goals and objectives for the supervisory relationship, and establishing mutually agreeable measurements of progress in supervision. Of particular importance in psychodynamic psychotherapy is the management of personal revelations in individual supervision. The following section of the chapter will comment upon the vulnerabilities of individual supervision that distinguish it from other types of educational experience. A section defines the various supervisory interventions, including both what the supervisor does and what is at risk for the supervisory enterprise with each intervention.
The relationship of individual supervision to assessment of competency will be explored. In most supervisory relationships there is an evaluation of both the supervisee and the supervisor, which is shared with an external entity, such as an educational program director or faculty evaluation committee. The distinction between feedback and evaluation will be reviewed as it pertains to individual supervision along with comments about how management of the power differential in the supervisory relationship influences the authenticity of evaluations. The final section will focus on the termination of the supervisory relationship with examples of useful and problematic termination processes offered as illustrations.
While ‘supervisory relationships’ take place in a wide range of educational and routine work situations, individual supervision was developed as a unique interpersonal structure for the purpose of developing competency in psychoanalysis. This unique interpersonal structure utilizes a deceptively simple form (individual meetings between a supervisor and supervisee for a specified amount of time on a regular and recurring basis) for the interaction of complex and sometimes competing aims and goals. The ongoing goal of the supervisor is the creation of a ‘safe enough’ environment in which the supervisee reports interactions between a learning therapist and a patient. Such reporting requires painstaking honesty in order to learn to apply psychotherapeutic principles and ideas to a specific and unique therapeutic dyad for which the learner has primary responsibility. Supervisors are responsible for maintaining not only safety in the supervisory relationship, but also vulnerability. The careful titration of safety and vulnerability allows the supervisee to develop professionally (with an inherent ongoing sense of personal vulnerability) while maintaining self-esteem and is accomplished through the experience of safety in the relationship with the supervisor. Learning about both patients and self is the primary goal of supervision for the supervisee. Such learning depends upon the tact, sensitivity, and knowledge of boundaries of the supervisor and also the study, courage, and trust of the supervisee. The educational product of individual supervision is new knowledge, skills, and attitudes on the part of both supervisor and supervisee. Good psychotherapy supervision regularly results in the fresh acquisition of knowledge by both parties. (Successful psychodynamic psychotherapy may be likened to participant observation in the co-creation of a novel. Successful individual supervision is subjectively quite similar.)
There are interprofessional differences in the content of individual supervision based upon both cultural and time differences in supervisory relationships. The education of mental health professionals lends itself to shifts in the content of individual supervision depending on the general professional developmental stage of the trainee. Early in professional education, the content of individual supervision may be weighted towards an in-depth discussion of cases and developing a professional relationship with the patient that can be used to implement specific treatment such as psychotherapy. The goal is predominantly to enrich the understanding of these cases beyond a focus on phenomenological diagnosis and/or pharmacological treatment. However, as the trainee begins didactic and experiential conferences about psychotherapy, the individual supervision moves towards a focus on the ongoing long-term or short-term psychotherapy cases. The structure of individual supervision varies somewhat among the main mental health disciplines. A common structure is for weekly individual meetings of about 1 hour in length each with two to four individual supervisors. Typically, new supervisors are assigned for each academic year in order to give the trainee a greater breadth of exposure. Some programs require longer exposure to a given supervisor. Supervisory assignments should take into account supervisee gender differences. These may be of particular importance for the understanding and management of intense erotic or hostile aggressive attachments of patient to therapist. Specifically, it is useful for supervisees to have supervisors of both genders, a woman supervisor is often especially sensitive to women supervisees encountering erotized negative transference with male patients, etc.
The individual supervisor is responsible for both the education of the mental health professional and the assurance of competent care for the patient. These primary aims of the supervisor may be in conflict or at least shift in balance of emphasis early in the mental health professional's development or at any time when the trainee is having difficulty and the patient is in a state of urgent need (Jacobs et al., 1995). This conflict is not limited to mental health professionals in psychotherapy. Each healthcare specialty has an analogous challenge when learners are included in the care of patients. While the apparent stakes may seem greater when moment to moment life-threatening procedures are talking place (for example, in cardiovascular or neurosurgical education), the highly personal nature of both psychotherapy and individual supervision intensifies the subjective experience of vulnerability for the learner.
Heinz Kohut's emphasis on the developmental needs of the self dramatically changed not only psychotherapeutic, but also educational cultures with a new emphasis on avoiding shame in processes requiring ongoing revision of the sense of self (Jacobs et al., 1995). Both psychotherapy and individual supervision, when successful, involve disruption of existing ways of thinking and behaving. Thus, psychotherapy education needs a special and specific educational structure to develop psychotherapy skills in the ‘translational’ arena in which concepts learned in classrooms are utilized in a specific treatment relationship. That unique educational structure is individual supervision.
The term supervisory alliance is used to describe the special relationship between the supervisor and supervisee. The supervisory alliance needs to be established and reinforced early in the relationship with each supervisee. Establishing the alliance requires specific effort on the part of both the supervisor and the supervisee and begins the new learning for both involved in the supervision relationship.
It is often helpful to begin with the supervisor taking an educational history. If the supervisee educational history in terms of formal education is unknown, that should be where the educational history begins. Specific emphasis should then be placed on the supervisee's previous experiences in individual supervision. Asking what the supervisee learned, what was helpful, what was dull or aversive, produces important information that may or may not predict the outcome of the current supervisory relationship but will certainly inform both parties about the context of their new partnership.
It is helpful for the supervisor to have an understanding of the supervisee's knowledge about psychotherapy, including any personal experience with it. However, this involves a significant boundary issue. The supervisor should convey the importance of privacy and confidentiality in psychotherapeutic relationships. Asking the supervisee ‘What do you know about psychotherapy?’ gives the supervisee an opportunity to reveal or not to reveal any personal experience with psychotherapy and may provide an opportunity for the supervisor to share his or her resources about what psychotherapy is like. For example, a supervisor who has prepared psychodynamic case formulations, process notes, or videotaped case presentations may share those materials with the supervisee along with an explanation of how it is that such personal and confidential material becomes available for dissemination.
Some supervisor/supervisee pairings are made with no input from the supervisee. If, however, the supervisee has to some degree ‘chosen’ the supervisor, it is important for both parties to be aware of the supervisee's motivations. Asking how the supervisee decided to choose a supervisor allows an opportunity for shared expectations to develop as well as misunderstandings to emerge. Further questions should discern what the supervisee expects to happen in supervision, what the supervisee expects to learn from it, and what the supervisee expects the supervisor and supervisee to do in order to make learning happen. Such exchanges contribute to developing the elements of a successful alliance. During this history taking, the supervisor should not only receive information from the supervisee, but also actively indicate his or her understanding of the questions asked to clarify what is expected of the supervisee. Specifying that the evaluation process will give the pair an opportunity to appreciate how the progress of their relationship will be assessed and should include a discussion of the evaluation instrument to be used and the timing of evaluations.
Individual supervision in each of the mental health disciplines should allow enough freedom to discuss any pressing matter of the supervisee. However, the supervisor should maintain a clear vision of the task of supervision (psychotherapy education) and prevent unhelpful diversions from the explicit task at hand. Excessive diversions may indicate either a general problem in developing psychotherapeutic competency or a specific problem with a patient being discussed that is either embarrassing or has evoked difficulties for the supervisee. It is helpful for the supervisor to clarify expectations about the supervisory appointments. In educational programs supervision time is ‘protected’ in the sense that it is a designated part of the educational work week, which takes precedence over anything except acute clinical emergencies. However, it is also ‘expected’ time for the trainee. Cancellations or requests to reschedule should be thoughtfully mentioned in advance when anticipatable and never promote the idea that supervision (and thereby, psychotherapy) is a casual, informal, or trivial matter.
There is no reason to assume that a junior supervisee in psychiatry, psychology, or social work knows what is supposed to happen in this novel and unique educational experience. Therefore, it is up to the supervisor to clarify the structure and expectations of the supervisee. With the current emphasis in psychiatry on phenomenological diagnosis supported by DSM-IV there is often a tendency for trainees to give rather short shrift to the developmental history or personal narrative of the patient, which is a fundamental importance for constructing a psychotherapeutic treatment plan. Thus, it is common and necessary for the supervisor to emphasize that the resident will be expected to present a developmental history with considerable attention to the patient's early interactions with his or her most significant figures. The idea that such information may be important predictors of psychopathology, current interpersonal relationship difficulties, and the therapeutic relationship itself may come as a new concept to the beginning therapist. This may be true even if that beginning therapist has already started the basic psychotherapy didactic courses of the program.
Some specific considerations of structuring the supervisory situation include the use of audiotape or videotape, the pros and cons of using process notes, and whether the supervisor will personally see the patient for whom the supervisee provides the psychotherapy. Eventually most competent supervisees present cases to their supervisors from memory with relatively few notes. For the senior psychotherapist and trainee or practitioners seeking individual supervision to enrich his or her educational possibilities from a busy clinical practice, process notes may be quite adequate. However, for the therapist-in-training or the postgraduate physician who seeks supervisory consultation because of a stalemate or crisis in a therapeutic relationship, a more thorough and systematic approach to getting started in individual supervision is generally advisable. Specifically during education in psychodynamic psychotherapy or psychoanalysis, constructing a psychodynamic case formulation is a fundamental competency. Specifically within psychiatric education, each second year resident should present several complete psychodynamic case formulations using models such as those found in standard textbooks of psychiatry or psychotherapy (Perry et al., 1987; MacKinnon and Yudofsky, 1991; Stoudemire, 1998; Gabbard, 2000).
Also as part of psychotherapy education it is extremely helpful for the therapist to have experience using process notes. Process notes refer to actual or reconstructed comments by the therapist and patient made throughout the session beginning with the first exchanges in the waiting or consulting room through the departure of the patient from the clinic or consulting room. Note taking during a session will often be seen as a distraction by both the therapist and the patient. This is particularly true with face-to-face therapies, but it may also be true for situations when the patient is lying down on a couch in an effort to increase his or her internal focus. A patient is often preoccupied by what motivates the therapist to write and may well be influenced by the therapist's note taking to the detriment of a focus on what is more salient to the person's difficulties. For the therapist, a focus on getting down exactly what is said might significantly interfere with using the self as an observing instrument in the therapeutic relationship and decrease the therapist's awareness of his or her responses to patient communications (particularly countertransference reactions) that could be of clinical or educational utility. Many trainees find it particularly helpful to reserve 10–15 minutes after the end of the session to reconstruct the sequence of exchanges that took place in the previous treatment session. With practice, the supervisee is usually able to capture adequately the flow of the communications in a way that makes for useful supervisory discussions.
For many psychotherapy educators, a report on the disconcerting concept of ‘lying in supervision’ provided a sort of traumatic disillusionment but useful reminder of the need for educational vigilance (Hantoot, 2000). It should come as no surprise that psychotherapists-in-training succumb to the all too human propensity for lying, and the biggest determinant of lying may be to protect the supervisee from disruption of ‘narcissistic equilibrium.’ A developmental basis for lying may be reawakened by separation and individuation efforts on the part of the student. Supervisors should be aware of the problem, sensitive to the emotional elements of the supervisory relationship, avoiding supervisor complacence, and be educated about their educational challenge.
One way to manage omissions and distortions by the supervisee is some form of recording of the sessions. Of course, audiotape is less intrusive than videotape and does not require as much technical support. The problem with audiotaping and videotaping is that some degree of editing is necessary in order for the supervision to involve more than just observing the sessions. In our experience it is unusual for more than about 15–20 minutes of a therapy session to be adequately discussed in a 50-minute supervisory session. Nonetheless, early in the development of psychotherapeutic competency, it is extremely valuable for a supervisor to have unedited information about the supervisee in action with a patient. Many things will simply go unobserved or unrecognized by even a very good supervisee early their professional development. This is particularly true regarding the way in which the supervisee makes transitions between topics or uses facilitatory language. The difference between ‘ok’ and a curious nonverbal grunt or simple exclamatory remark, for example, can be quite significant for the patient and the process (Havens, 1978).
The decision of the supervisor to meet personally with the patient being supervised is a significant one. Of course, such an interview will have an effect on the relationship between the supervisee and the patient, but that effect can be positive or negative. Influenced in part by billing requirements, supervisors in some clinics participate in the first 10 or 15 minutes of psychotherapy sessions predominantly conducted by a trainee therapist. While this would be a very poor arrangement for the entire psychotherapy education experience of the trainee, it does provide an interesting and sometimes valuable educational experience early in the development of the psychotherapist. Of course, it greatly informs the supervisor about the patient. It can also help the supervisee to both see what the supervisor would actually do with a particular patient and also (for better and worse) affects the idealization of the supervisor by the supervisee. Even as a limited structure for therapists early in training, this arrangement can be damaging to the establishment of a psychotherapeutic relationship. The physical presence of a designated higher authority can undermine the trust or confidence of any patient and may facilitate unhelpful ‘splitting’ with devaluation of the junior therapist with borderline or narcissistic patients.
In summary, the goals of the supervisory alliance are to overcome the obstacles to learning, to provide nonjudgmental feedback and evaluation, and to explore anxiety on the part of the supervisee as an impediment to learning—both learning from the patient in psychotherapy and from the supervisor in supervision. In subsequent sections of this chapter, more about managing anxiety of the supervisee will be developed. However, an important basic distinction is that a supervisor explores supervisee anxiety as an impediment to learning not as a consequence of a personal history of conflicts. The latter is the domain of personal therapy, which has analogies to supervision but significant boundary differences.
A detailed focus on the patient being presented in individual supervision is a necessary but not sufficient perspective for developing psychotherapeutic competence. Such a focus would unhelpfully limit the supervisory dialog. The supervisory dialog should include discussions of the therapist's feelings, ideas, and images that produce or inhibit therapeutic activity. Such conversations often begin when either the supervisor or supervisee become aware that the supervisee did not act on available information with a therapeutically appropriate question, confrontation, interpretation, or empathic intervention. Curiosity of either the supervisor or supervisee often leads to recognizing a subjective reluctance of the supervisee, which is helpful to name or identify. Commonly, the supervisee was anxious, irritated, sexually aroused, or had some other thought, feeling, or idea which resulted in the withholding of therapeutic activity. The supervisory goal is to help the supervisee contain such uncomfortable experiences without diminishing awareness of them. The capacity for containment in the therapist is similar to the capacity for equanimity espoused as one desirable capacity of physicians by Osler and others (Osler, 1947). While it is important for both the supervisor and supervisee to keep in mind how unusual it is to have an ongoing relationship in which emotions are discussed without leading to a behavior, good supervision involves mutual exploration of exactly such situations in the service of producing therapeutic competence. The supervisor and supervisee should attempt to relate the emergence of the difficult emotion to the specific provoking event in the therapeutic process. Together the supervisor and supervisee should review potential precipitants in the therapist/patient relationship to determine if a substantive connection between the feelings and precipitant can be established and understood. Sometimes the supervisee will be embarrassed by a curiosity that seems ‘voyeuristic’ and unusual to pursue in most social contexts. Just as psychoanalysis is a relationship for which there is ‘no model in the rest of human experience’ (Freud, 1958), supervision shares some of this uniqueness, but the focus is on anxiety, which limits therapeutic activity rather than the history of personal adverse relationships or internal conflicts such as is the focus in psychotherapeutic and psychoanalytic relationships.
Good supervision engenders the development of a therapeutic curiosity to review hypotheses in the supervisory relationship and then independently in psychotherapeutic relationships outside the ones being supervised. This curiosity allows the supervisee to reflect upon the nature of the connection being made between any one reaction to a patient and similar reactions in other psychotherapeutic encounters. It often leads the supervisee to appreciate patterns of therapeutic inhibition, which become clues guiding his or her therapeutic conduct. In a somewhat oversimplified way, the therapist-in-training learns to make accommodations based on self-knowledge about what impedes or enhances therapeutic activity. For many therapists, this curiosity and pattern recognition leads the therapist-in-training to pursue personal therapy. For example, in supervisory discussions about two patients with unexpected negative outcomes, it became clear that the therapist had been reluctant to make an observation about evidence of an emerging erotic transference. The supervisory discussion about the pattern of therapeutic inhibition led the supervisee to seek a consultation that led to a recommendation of personal psychoanalysis.
What is different about individual supervision than other types of teacher–learner relationships is that it makes a very personal self-examination a public matter. Such self-examination is not a part of many other professional exchanges and is actively avoided in some. For example, it will be the unusual physician therapist who has experienced these opportunities for reflection in his or her exchanges with surgical and medical attendings in other specialties.
The principle for the supervisor to keep in mind is that the supervision should focus on examining material relevant to the treatment of patients and be pertinent to the educational needs of the supervisee. The examination is not for the personal needs of the trainee or the supervisor. Such examination requires security and predictability of a secure enough consultative relationship. Supervisory tact and timing also are quite important. Especially early on in supervisory relationships, the supervisor may have an idea about the supervisee that is too far ahead of supervisee's psychological development, self-reflecting capacity, or introspective ability. An important question is whether a particular observation of the supervisor is discussible at this point in time. Sometimes, humor can be helpful, but humor at the expense of the supervisor in a somewhat self-depreciatory tone is preferable to any indication that one is laughing at the dilemmas of the therapist-in-training. At times, it is rather clear that a supervisee would benefit from personal therapy. It is important that a supervisee who brings highly personal material into a supervisory relationship be encouraged to seek personal therapy while clarifying the focus of the individual supervision. Once one gets started talking about things in supervision that belong in personal therapy, it is very hard to extricate oneself gracefully. Helping a supervisee ‘wonder’ whether anxiety limiting therapeutic activity could be addressed in personal therapy is generally better than telling a supervisee that he or she should seek treatment.
The supervisor has a wide variety of available interventions ranging from active listening and clarification to role playing to interpretation of parallel process (Doeherman, 1976). Each intervention has a particular use and will be employed differently depending upon specifics of the supervisee, the stage of the two relationships involved, the salience of any current crisis, and the opportunity to deal with enduring themes in either (treatment or supervisory) relationship. Each intervention also has potential for both positive and negative consequences for the supervisee and the educational alliance. This section defines and elaborates some of the fundamental supervisory interventions (Jacobs et al., 1995).
Active listening on the part of the supervisor involves simultaneous reception and ordering of information about both the patient being discussed and the supervisee doing the presenting and developing a conceptual model of the relevant clinical and educational issues at hand for both the patient being discussed, the supervisee, and the supervisee/supervisor relationship. A constellation of individual and relational perspectives was recently termed ‘The Triadic Match’ (Kantrowitz, 2002).
Early in psychotherapy learning, the supervisee is especially likely to appreciate modeling of therapy interventions on the part of the supervisor. Such demonstrative teaching can promote identification of the supervisee with the supervisor by providing a vivid example utilizing the greater experience of the supervisor. Such modeling is best done in a somewhat tentative format such as ‘I can imagine myself saying…’ or ‘Early in therapy I would be more inclined to say ——, but later ——’ (for example, when responding to the question of whether to respond to a direct request for advice on the part of the patient). On the downside, modeling can come across as a constricting directive to the supervisee claiming that there is one ‘correct’ response. It is helpful to remember that the best answer to the novice therapist question by the supervisee of ‘What would you say in this situation?’ is ‘I don't know.’ Of course, this response should be followed by the explanation that individual factors prevent a fixed correct response that is inevitably correct. However, it is also helpful to provide examples of ‘one way’ of responding to the novice therapist with the caveat that whatever is said or done must be done in the language and style of the supervisee in order to be perceived as authentic on the part of the patient.
Didactic instruction has a significant place in individual supervision, especially early on in any supervisory relationship. It is important to review diagnostic criteria and how diagnosis relates to psychotherapeutic strategies. Every supervisee needs the opportunity to do case formulations. Each training program should ensure that opportunity is available in a systematic fashion. It is also helpful to discuss identifying and assessing different types of defense mechanisms for the psychodynamic psychotherapies. One purpose of this discussion is to help the supervisee understand that the predominance of certain defenses predicts suitability to different types of psychotherapeutic interventions. Such didactic instruction is an invaluable orientation and also often helps titrate supervisee anxiety thereby building the foundation of the alliance. Supervisors should advise early and whenever patient safety is a question. Explanation, as opposed to directives or pronouncements, is preferable. On the downside, excessive didactic instruction can result in a kind of dogmatism and defensive, mutual laziness for both supervisor and supervisee. The supervisor can bask in an aura of supervisor authority at the expense of learning from his supervisee. Security gained by excessive didactic instruction can come at the expense of growth, change, and the capacity to make useful generalizations.
Socratic questioning can facilitate supervisee creativity and learning if it is done in an atmosphere of genuine curiosity and exploration, e.g., an emphasis on ‘wondering’ together. Such questioning encourages imagination if the supervisor does not have ‘the correct answer’ too firmly in mind. The downside of such questioning is that it leads to a sort of demeaning interrogation when it devolves into an exercise of ‘Guess what I am thinking.’ Such interrogation can be especially damaging to the therapeutic alliance if a supervisee is prone to shame and not a good guesser about what the supervisor is thinking.
Encouragement and permission are very important elements of the typical supervisory relationship. For the most part, mental health practitioners are individuals with temperaments characterized by reward dependence and persistence. We tend to embark cautiously on new activities while looking for the approval of those in authority or with more experience. Encouragement and permission giving facilitate experimentation. Experimental learning is often impeded when the supervisee is unhelpfully afraid of making a patient angry, sad, sexual aroused, dependent, etc. In this situation, there may be a mutual reluctance on the part of the patient and supervisee to disturb a familiar pattern of adaptation or comfortable defensive posture. Conflicts over voyeurism may lead a supervisee to avoid seeking details where specific information is critical, i.e., the masturbatory fantasies of a patient conflicted about sexual orientation. The goal of encouragement and permission is to provide a therapeutically optimal balance of internal freedom with professional restraint. The downside of encouragement and permission-giving interventions is that they can become a burden or demand to perform. The supervisee needs to be ready (or at least almost ready) to inquire, and the supervisor can judge readiness very imperfectly. Exhortations to ask specific questions on the part of the supervisor are generally ill advised and specifically ill advised when they specify the form or language of the therapeutic interventions.
Clarifications and confrontations about explicit but unacknowledged aspects of the supervisee's observable attitudes or behaviors are the beginnings of a shift in emphasis in the supervisor/supervisee relationship. Clarification involves summarizing congruencies among supervisee reports of a particular case or cases or inquiring about unreported subjective feelings of the supervisee regarding a patient/supervisee interaction. Confrontations involve highlighting expressed inconsistencies in supervisee comments (‘You had established a policy that you would charge the patient for cancellations given without 24-hour notice and yet you volunteered to not charge for the session missed because of a possible thunderstorm’). Such confrontations are important steps in helping the supervisee to understand and contain affects in the patient/therapist relationship. Both understanding and containment are facilitated when supervisee affects become the focus of attention. However, this shift from a focus on the patient to a focus on the supervisee inevitably increases the tension in the supervisory relationship and creates a potential for narcissistic injury on the part of the supervisee. The supervisory relationship is inherently unequal and should not be exploited to force a supervisee to reveal highly personal information about the supervisor's personal history or private mental life. Supervisee readiness to embark on such self-reflection should be considered when the safety of a patient is not at stake.
Supervisory interpretations include interpretations of feelings, psychodynamic factors, motivations, and defenses. Interpretation of negative affect (embarrassment about one's acting on curiosity, feeling insecure as a therapist when being devalued by a patient, etc.) can both add depth to learning and decrease the tension in the supervisor and supervisee relationship by placing something ‘on the table’ that had been important but not discussed. Interpretation of a motivation, ‘I think you were afraid of making the patient angry.’ if correct can often lead to an important discussion of an inhibition to therapeutic action that can be overcome with assistance. Interpretation of a defense by a supervisor (‘I wonder if you changed the topic because you were intimidated by the patient's deepening sadness and grief?’) can help the supervisee both to self-monitor changes and also begin to explore a potential countertransference problem. However, interpretation of defense generally increases supervisee anxiety and is best done after a workable educational alliance has been established.
A particular form of interpretative activity in supervision is the interpretation of ‘parallel process.’ This extraordinary event in supervision was first described in the late 60s and refers to the situation in which a conflict in a patient is reproduced by the supervisee in the supervisory relationship (Ekstein and Wallerstein, 1958). In some psychotherapy education programs, students are introduced to the concept of individual supervision, which can include a specific example of parallel process such as the following:
A second year male resident was discussing a 21-year-old woman patient who became transiently psychotic while watching a movie, The Exorcist. While the patient had a somewhat turbulent adolescence, she never had identified psychopathology before experiencing a sudden intense panic attack while watching the scene where the little girl protagonist masturbates with a crucifix. The patient had returned to a fairly stable anxiety symptoms and no psychotic symptoms about 3 months later when she was referred for dynamic psychotherapy. The resident was a competent and thorough man, somewhat obsessionally organized, and had been presenting the patient's twice a week psychotherapy to his admired, competent, and quite attractive supervisor. In the supervisory session in question, the resident was complaining that the patient seemed reluctant to deepen the therapy and, in fact, was resistant and ‘acting out’ by coming late, offering important personal revelations only at the very end of the session and was generally slowing down the process. Summing up his observations at the end of the supervisory session, he grossed ‘It is as if she does one thing or another to test the therapeutic boundary and to block my vision of her inner life.’ The supervisor smiled sweetly and said in a measured tone ‘I wonder if what she is doing with you is like your placing your overcoat on top of my clock so that I cannot see when supervision is over?’ The resident's hot and reddened face suggested that indeed there was a connection. There was not much more discussed about the resident's enactment of a parallel process in that session.
Nonetheless, the resident was emboldened to confront and eventually interpret his patient's acting out. Together, the resident and patient eventually learned why that scene caused her such grief, but the supervisor never made the resident confess how his supervisor's attractiveness influenced his choice of her for supervision.
This reported supervisory session is offered both to illustrate how interpretation of parallel process added a depth to learning that could not have been obtained by reading or lecture and also to confirm that supervision may include embarrassing but useful educational development. It is an example that with the right supervisee, enough information, and an adequate alliance the interpretation of a parallel process can capture a defense of the supervisee, which was analogous to the patient's obfuscating behavior. The supervisor's comment increased the supervisee's anxiety but the alliance was good enough for it to be a productive anxiety that promoted learning.
Interpretations are the riskiest form of interventions and can become a sort of ‘patient making’ of the supervisee. In academic settings, this would be making the supervisee the equivalent of an involuntary patient as supervision is a required assignment. As in the example, the supervisor should not make the supervisee confess too much personal material. For one thing, the supervisor usually has a much weaker data base than a therapist. There is also great potential for misuse because of the power imbalance in the relationship. Nevertheless, an interpretation of parallel process often assists in getting something important into the supervisory discussion. The capacity to make such interpretations is considered by some to be a developmental marker of competency of supervisors (Rodenhauser, 1994).
Role playing is a form of supervisory interaction that can be a source of considerable learning. It is also rather fun. The supervisor and supervisee can take the part of either the patient or the therapist in the role playing once adequate information about the patient is presented. While playing the part of the patient, the supervisee often achieves a new level of empathic appreciation of the patient. Role playing also provides the opportunity to observe in vivo modeling on the part of the supervisor. Additionally, when playing the therapist, the supervisor often is presented with new information about the kinds of problems the patient presents in psychotherapy as the supervisee enacts those problems.
Supervision in CBT is considerably more structured than psychodynamic therapy supervision. Most of the CBT writing on supervision comes from practitioners of Beck's cognitive therapy. In cognitive therapy the supervision session echoes the design of a typical therapy session (Newman, 1998), so it includes key elements such as agenda setting, bridge from the previous supervision session, use of capsule summaries and request for feedback from the supervisee (Liese and Beck, 1997). Structuring supervision in this way models skills the therapist will be using in sessions with patients. Supervisees often comment on how this approach helps them structure their own therapy sessions. Applying this format to supervision also encourages the best use of the time available, particularly if the supervision is in a group. Supervisor and therapist(s) decide together at the beginning of the session which patients are to be discussed and what is the key supervision question. A bridge is made between this and the previous session to remind the participants of the context and promote continuity in case management. Another important structural element is the use of summaries and feedback. Therapists always go away having been asked to outline what they have learned from the meeting and how they will apply this in their next session with the patient. Just as in therapy, there is flexibility within this scaffolding allowing supervisor and therapist to follow other paths and renegotiate the agenda if necessary.
As in psychodynamic therapy, there is an expectation that the therapist will take responsibility for his or her own learning experience. Again, this is made more explicit in cognitive therapy. At the beginning of the supervisory relationship, the therapist is asked about his or her previous experience of cognitive therapy and of therapy in general, and encouraged to think about the strengths and weaknesses in their cognitive therapy skills. This helps towards the construction of some specific learning objectives. For instance, in a 6-month supervision placement on a CBT course participants identified two main skills they wished to develop: (1) case conceptualization, and (2) dealing with patients who find it hard to be focused and just want to talk.
The therapists were then asked to consider these overarching goals when bringing a case to supervision, i.e., is there any material that might be relevant to the skill they are trying to develop. Therapists are expected to prepare for supervision by listening to an audiotape of their therapy session and selecting a 10-minute segment that illustrates their supervision question. Novice therapists often frame their question as ‘What do I do next?’ but with time and practice they can make the questions they ask more precise and focused, e.g., ‘How can I devise a behavioral experiment to help this patient test her fear of social situations.’ This approach is very different from psychodynamic therapy supervision, which usually asks the therapist to relate an account of the session as a whole.
Supervision can focus on a number of different areas. Padesky (1997) suggests that the session can address skills acquisition, case conceptualization, the client–therapist relationship, therapist reactions, and supervisory processes. There are a number of methods for addressing these including case discussion, videotape, audiotape, live observation, and role play. Case discussion is probably most useful when issues of conceptualization are raised, because it allows for a general consideration of the patient's history and early experiences, target problems, thoughts and beliefs elicited, etc. Although this is the traditional mode of operating in much supervision it may be less helpful in developing skills or looking at the therapeutic relationship. Cognitive therapists routinely audiotape or videotape their sessions. Listening to a tape of a session is invaluable for identifying skills deficits and observing difficulties in the therapeutic relationship. Therapists are initially a little nervous about presenting tapes for supervision. This can be overcome by the supervisor discussing his or her own experience of training and supervision and the universality of these fears. The therapist's automatic thoughts about taping sessions can also be examined. We often work on the assumption that our tapes must be perfect, forgetting that the whole purpose of supervision is to learn new skills. Group supervision can be useful in this respect, because supervisees soon realize that they are all in the same boat. Listening to others’ tapes usually demonstrates that they have similar areas where they need to improve.
Role play is used increasingly in CBT supervision, and this again lends itself well to a group setting. Listening to a tape can help the supervisor to identify an area where the supervisee needs to practice skills. Then a role play can be set up. Perhaps the supervisor begins by demonstrating how to use the technique with the supervisee playing the patient. Then the therapist can practice the technique with the supervisor or another trainee as the patient. John was a novice therapist who was having difficulty setting an agenda with one of his patients. The patient wanted to talk about what had happened during the week and would launch into a blow by blow account of every encounter and irritation that had occurred since they last met. This was taking up a good part of the session and preventing them from getting down to much problem-focused work. John role played the patient and the supervisor modeled how to gently interrupt and remind the patient that this was just the beginning of the session—the therapist and patient needed to decide what it would be most helpful to discuss in the following 50 minutes. This worked well. However, when John then took the role of therapist with another group member as the patient, he failed to prevent her from going on and on. Observing the role play allowed the supervisor to see that John was very good at facilitating emotional expression in his patient. He would nod and show an interest and say ‘aha’ thus encouraging the patient to talk even more. John then practiced giving less facilitating responses at this agenda setting stage and determined to try this out in his next session.
John's difficulty in intervening with his patient proved to be a result of an underlying belief that if he interrupted a patient he would be seen as rude. Once this belief became clear, the therapist asked the other supervisees if they had similar beliefs. They all confessed to ideas such as ‘If I stop a patient talking, they will be upset and won't come back’ or ‘If I interrupt a patient, they will be angry with me.’ John felt less alone in his problem, and we were all able to acknowledge how difficult it can be to act in ways that we know are therapeutic but may not seem ‘nice.’ As a group we then came up with an alternative belief: ‘If I interrupt, it will help me and the patient get more out of therapy.’ Identifying and testing therapists’ beliefs like this can greatly aid their development as cognitive therapists. Paolo (1998) gives an account of how her own experience of cognitive therapy supervision allowed her to discover her assumption that she had to keep things calm, smooth, and rational so that the patient did not get too emotional. With the help of her supervisor she created alternative beliefs, such as ‘I can handle emotional arousal in myself and others. Genuineness involves intentionally attending to the affect of the given moment. The risks are worth taking,’ that she was then able to test in subsequent work with her patient.
Discussion of transference and countertransference is obviously one of the main concerns in psychodynamic therapy supervision. While these issues are given less attention in cognitive therapy, they are by no means ignored. As Liese and Beck (1997, p. 119) remark:
For more complicated patients, especially those with personality disorders, the therapeutic relationship becomes a central focus in therapy as therapists help patients identify and modify distorted thoughts and beliefs about the therapist (and they are helped to generalize this learning to other relationships). Supervisors encourage therapists to pay careful attention to the interpersonal processes that occur during treatment (i.e., transference and countertransference) and to resolve any therapeutic difficulties as directly as possible.
Transference can often be conceptualized as a compensatory interpersonal strategy that the patient uses with the therapist and with other important people in his or her life. For instance, patients who have experienced significant neglect, abandonment, or rejection, their life may develop beliefs that people cannot be trusted and that the best strategy is to not let anyone get close. This may cause problems in the therapeutic alliance when, for instance, the cognitive therapist asks the patient to record automatic thoughts as a homework assignment. Revealing intimate feelings may be too threatening for the patient, and they may respond by failing to do their homework. If the therapist's countertransference feelings are of irritation and frustration, there is a danger that these will be picked up by the patient and perceived as yet more evidence for their belief that no one can be trusted. The supervisor can identify these problems when the therapist reports these difficulties in case discussion, through listening to the tape of the session or through role play. The transference and countertransference thoughts, feelings, and behavior can be located within the cognitive case conceptualization. A number of options for handling the situation are then available (all framed as ways to test the transference hypothesis):
The therapist can elicit the patient's negative thoughts about homework and use guided discovery to relate them to the conceptualization.
The therapist can use standard techniques to help the patient test the belief that the therapist cannot be trusted.
Recording thoughts and feelings can be formulated as a behavioral experiment to test whether or not it is safe to reveal feelings in therapy.
Therapist and patient can collaboratively agree that it is too early in the therapy for the patient to reveal these feelings, and try other, less threatening homework.
A good supervisor uses guided discovery as well as direct advice to help the therapist understand and generate strategies. The supervisory relationship, like therapy, is collaborative, so there would be an open discussion of which of these approaches the therapist thinks would work with the patient as well as which feel most comfortable.
Supervision has always been recognized as a vital aspect of training in CBT, but research in this area has lagged behind research into therapy outcome. Much of the research that has been done can be found in the behavioral therapy and learning disability literature (Milne and James, 2000). Reviewers have concluded that the evidence supports systematic interpersonal skills training as more effective than ‘traditional’ supervision that focuses on case reports and discussion (Lambert and Ogle, 1997; Milne and James, 2000). Some support for this use of structured learning comes from an unexpected source. Binder and Strupp (1997) when reporting the experience of training therapists in their time-limited dynamic psychotherapy recommend the use of tape recording to aid skills development, and teaching ‘precise case conceptualizations, anchored in the patient's experience’ and giving ‘precise communications about concepts, principles and evaluative feedback.’ Their research showed that a trainer who used a rather general supervisory style was less effective than one who was much more specific (e.g., stopped the tape and asked specific questions, confronted therapists when they went ‘off-model’). The therapist with the more focused approach achieved a group effect size pre-post training of 3.58 for adherence to the model as opposed to 0.46 for the less focused therapist (Henry et al., 1993). There was also a difference in quality of general psychodynamic technique (effect size 1.29 versus 0.24). A small amount of evidence exists in the cognitive therapy literature supporting the effectiveness of supervision. Beck found that the skills learned in a 3-month training were lost after 9 months. However, if the training was followed up by regular supervision, there was a cumulative increase in competence. Similarly, cognitive therapists showed a training effect over the course of supervision in a trial of psychotherapy for substance misuse. Supportive-expressive therapists and drug counselors on the other hand did not.
In summary, supervision in CBT has characteristics in common with psychodynamic therapy (interest in case conceptualization, an assumption that therapists will take personal responsibility for their work, attention to the therapeutic relationship and focus on therapists’ beliefs). The main differences are in the style and format of therapy. CBT supervision sessions are structured and focused and utilize a number of methods that are not routinely used in psychodynamic therapy supervision (listening to tapes of session and role play). The field is open for research investigating whether or not these specific supervision techniques facilitate learning in the way that cognitive therapists believe.
Documenting the determination of competency has become increasingly critical in mental health professional education. Therefore, most mental health training programs have revised or are in the process of revising evaluation tools to better assess trainees’ competence in multiple modes of psychotherapy. Most training programs are also implementing strategies to make programmatic changes in teaching psychotherapies based on accreditation requirements, program feedback, and/or trainee performance trends as evidenced by trainees’ individual evaluations. Individual supervision provides an excellent opportunity to follow trainees’ progress in attaining the psychotherapy knowledge, skills, and attitudes consistent with being competent in multiple modes of psychotherapy.
By definition, individual supervision occurs on a regular and recurring basis (usually two supervisors weekly for an entire year during every year of psychiatry residency training). This construct of individual supervision is ideal for assessing competency because therapist trainees’ knowledge, skills, and attitudes can be followed, and hopefully directly observed, repeatedly by the same person over an extended period of time. Individual supervision (multiple observations by the same person over an extended period of time) provides useful information that is not available from most other existing standard assessment methods [multiple choice tests, clinical attending evaluations, oral examinations, Objective Structured Clinical Evaluation (OSCE), etc.]. As good assessment is a form of learning and should provide guidance and support to address learning needs (Epstein and Hundert, 2002), individual supervision is designed to accomplish exactly such learning and guidance. Few validated strategies to assess actual clinical practice exist in all of medicine or mental health training. Individual supervision seems to come very close to assessing trainee competency as evidenced in actual clinical practice, at least for the practice of psychotherapy. To enhance further its usefulness in the competency assessment of psychotherapy knowledge and skills, individual supervision should include some form of direct observation. This could include actual contact with patients that the therapist trainee sees for therapy, or videotaped or audiotaped recordings of actual psychotherapy sessions, or less ideally, carefully taken process notes. To improve interrater reliability among supervisors, standardized rating forms might be helpful for supervisors to use when viewing videotaped or audiotaped psychotherapy sessions of supervisees.
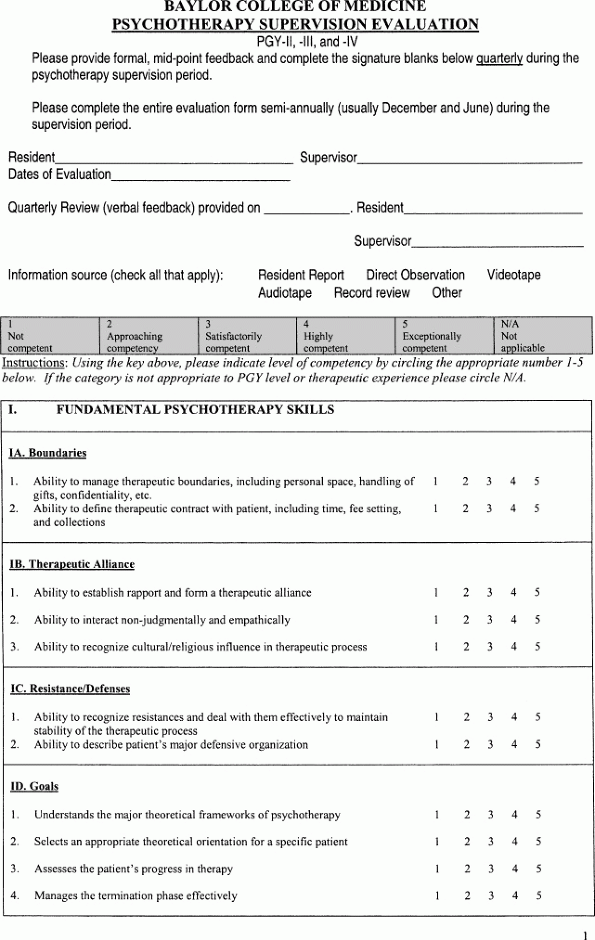
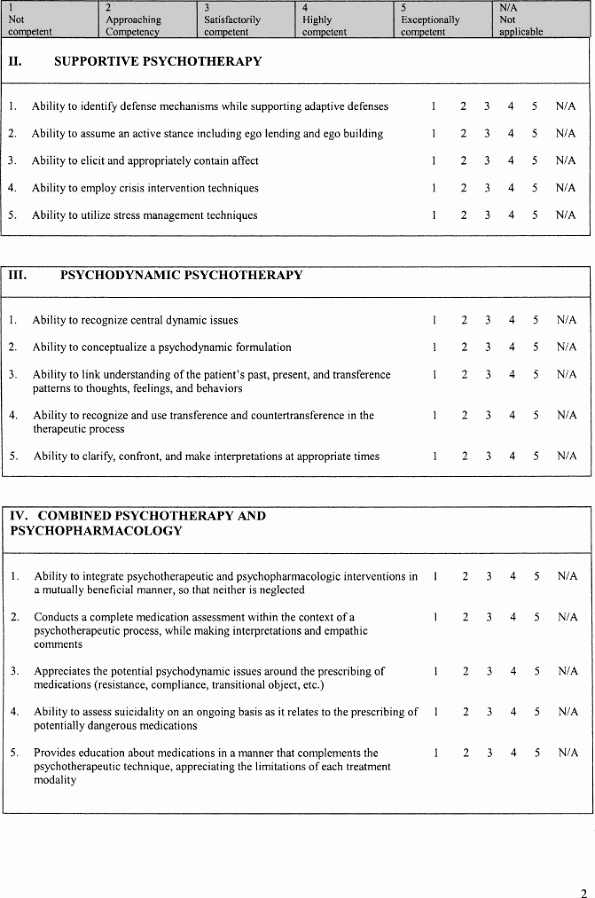
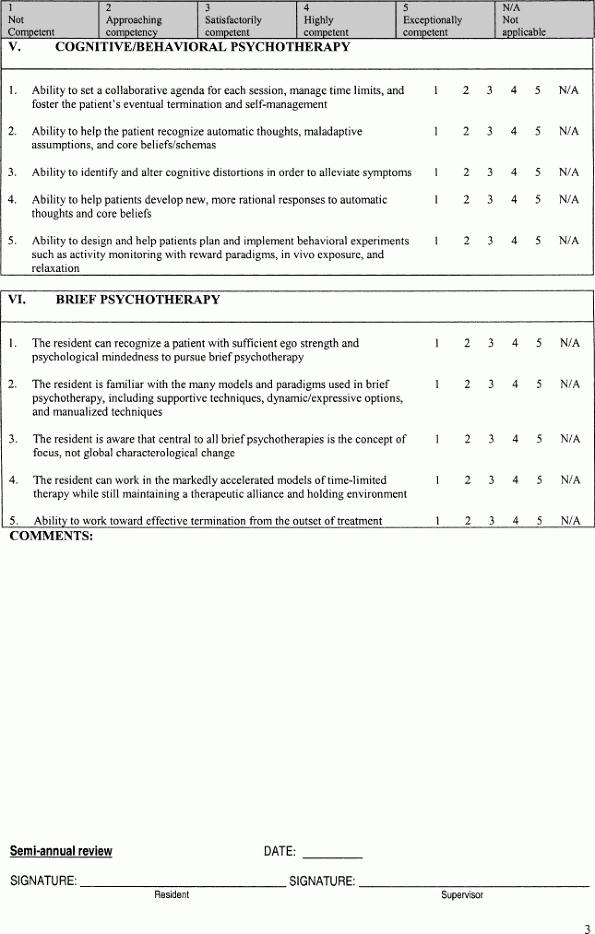
An example of a specific written psychotherapy evaluation tool is included at the end of this chapter (Appendix 42.1). Key elements of this evaluation tool include the following: (1) an expectation and reminder to faculty to provide mid-point feedback to the therapist trainee being evaluated; (2) a space for faculty to indicate information sources used on which to base their evaluation (trainee report, direct observation, videotape or audiotape review, record review, or other); and (3) a Likert scale to evaluate knowledge and skills in five forms of psychotherapy, which is designed to be as effective of an evaluation tool for trainees beginning to learn psychotherapy as for the most experienced trainees. Beginning therapists would be expected to receive evaluations of 1, 2, or 3, depending on their native empathic abilities and previous experiences. More experienced trainees would be expected to receive evaluations of 3, 4, or 5, again depending somewhat on their native empathic skills. Remediation programs (didactic and clinical) would need to be designed to raise the level of competency in any areas of knowledge of skills consistently evaluated as not competent. Programmatic changes (didactic or clinical) would need to be made if many or most trainees were consistently evaluated as not competent or approaching competency in any single knowledge or skill area or for any given type of psychotherapy.
Use of this type of psychotherapy evaluation tool may alter the supervisor–supervisee relationship. The expectation that supervisors evaluate supervisee competency, rather than only providing feedback to help teach the knowledge and skills of psychotherapy, expands the role of individual supervision and ‘ups the ante’ of the supervisory alliance. In addition to teaching psychotherapy and to assuring that competent patient care is being provided, supervisors will now be expected to assess competency in doing psychotherapy. One might assume that ‘assuring competent care’ is equivalent to ‘assuring trainee competency in doing psychotherapy’. It is the authors’ contention that these are, in fact, two different supervisor tasks or responsibilities. Training program directors will likely need to demonstrate that they have structures in place to adequately train supervisors to fulfill all three of their key responsibilities (education, clinical care, and competency assessment). Such structures might include new supervisor training sessions, supervisor workshops or retreats, or systematic evaluation of supervisors.
Feedback and evaluation are critical components of any educational endeavor; however, they are all too often given only very cursory attention and handled in a haphazard fashion. As an academic mental health professional providing supervision, one is obligated to dedicate sufficient time, reflection, and energy to the process of feedback during the supervisory process so that appropriate behavioral changes can occur in trainees. In this section, the differences between feedback and evaluation will be discussed and some barriers to their effective implementation considered.
Though the terms are often used interchangeably, there are important differences between feedback and evaluation that have earned significant recent attention in academic psychiatry and education in general. Frequently, we as teachers are guilty of utilizing evaluative terms and techniques when feedback would be more in order. Consistency in this separation is much trickier than might first be imagined and requires continuous practice and thoughtful, self-reflection to master.
In short, feedback is intended to be formative, while evaluation is summative in nature. In this sense, formative relates to an ongoing process of growth and development while summative is defined as a conclusion or final assessment. There are important differences in the manner in which a supervisor provides feedback and evaluation that help to maintain this separation.
Feedback, when used properly, molds and improves behavior in the future by identifying strengths and correcting weaknesses or deficiencies. To do so, feedback must be exquisitely specific, down to the finest of details. Though this might seem to be ‘nit picking’ and impossibly tedious, it is only with specificity that desired modifications of behavior can be recognized and internalized effectively. Evaluation provides subjective judgment about behavior that has already happened with a final assessment of the quality of that behavior. Feedback ideally employs neutral statements of observed fact with little use of adjectives, whereas evaluation defines the acceptability and quality of a performance compared with a known or presumed benchmark. Feedback should be provided throughout a learning experience and in innumerable, small aliquots, while evaluations are intended for use after educational experiences have been completed and generally in a single, comprehensive format.
It is probably of value to illustrate some comparative examples of feedback statements compared with evaluation statements.
Feedback: You collected information about the patient's developmental history (fact), but I did not hear you discuss the provocative relationship he mentioned with his cousin (fact).
Evaluation: Your interview skills are quite good (judgment) and you develop solid (judgment) rapport with patients, but you do not explore sexuality as much as I would like to see at your level of training (judgment).
Feedback: It is important for you to recognize that your strong emotions in this case may arise from the difficult and competitive relationship with your father that (fact) you told me you anticipated when you first received the referral.
Evaluation: You have an excellent (judgment) grasp of the theoretical basis and implementation of the ideas of transference and countertransference and are beginning to translate them into an appropriately chosen long-term therapy case.
In psychotherapy supervision, as in any educational venture, feedback and evaluation must be bidirectional, with flow of corrective comments from learner to teacher as well as the other way around. As mentioned elsewhere in this chapter, the supervisee's goals and expectations for the supervisory work should be explicit from the beginning and the supervisee must feel free to adjust supervisor behavior to steer continuously toward these ends in a fashion that is tolerable to the trainee. Only in a state of mutual respect, safety, and openness can this give and take occur appropriately. If the process has become too intense or stimulating for the leaner, it must be acceptable for him/her to temper the relationship to a more suitable level. This presents some risk for narcissistic injury on the part of the supervisor, in contrast to the supervisee injuries mentioned previously in this chapter, but the more experienced supervisor will have well-developed resources to manage this challenge.
This last situation, that of a wounded party in the supervisor–supervisee dyad, segues well into a discussion of some potential barriers to effective feedback and evaluation. Paramount among these perhaps is the fear within both teacher and student that feedback will have consequences beyond those that were intended (Ende, 1983). This is most often the fear when one is forced to provide feedback that is critical and negative in nature. Few people enjoy being told of their deficiencies, but most tolerate it with reasonable grace. There is often great fear, however, that even well-intentioned comments have the potential to elicit a powerful, emotional reaction on the part of the person receiving the feedback/evaluation. Anger, defensiveness, hurt, sorrow, self-deprecation, and other difficult responses might manifest in the recipient of feedback, whether or not the information was provided in an untoward manner. Trainees and teachers alike can experience feedback as a comment on personal value or worth, leading to great risk for narcissistic injury. In situations where evaluations play a role in promotion or awards, these emotional reactions can sour the process of fair assessment and lead to detrimental results for faculty or student. Finally, the relationship might be fractured irreparably and the popularity of the supervisor might be diminished. While the extreme among these responses are relatively rare, the fear of these unexpected and unintended outcomes conspires within supervisors and supervisees both to foster collusion to avoid feedback and evaluation altogether. The result then is often a perfunctory and grossly inadequate, ‘Great job,’ or ‘You're doing fine, just fine.’
A second impediment to effective feedback and evaluation is the increasing absence of directly observed behavior within training settings. Mechanisms of observation (videotape, audiotape, process notes, sitting in for a session, etc.) have been discussed for their advantages and drawbacks elsewhere in the chapter. It is important, though, in the context of feedback and evaluation to expand on the necessity of direct observation in providing the all important data that will be used during comment on trainee behavior. Particularly in our very subjective field, it is a must to be aware of the literature on trainee self-assessment of interpersonal skill. A number of studies have (Donnelly et al., 2000; Stewart et al., 2000; Zonia and Stommel, 2000; Tulsky et al., 2001; Davis, 2002; Millis et al., 2002) demonstrated the inability of resident trainees in various specialties to self-assess their own interpersonal skill while confirming attending physicians ability to judge accurately these same interactions with patients, both real and standardized, on identical interpersonal measures. This has tremendous ramifications for the supervisory process, essentially demanding that the supervisor directly observe the psychotherapy in some fashion so as to confirm a supervisee's reports of rapport and therapeutic alliance. Only then can accurate and useful feedback be provided.
Some final barriers to effective feedback and evaluation are the significant amount of time, stamina, and organizational skill required to take advantage of the many opportunities for comment on a supervisee's behavior. It is much easier, and often much more intriguing, to passively allow the very titillating stories encountered in supervisory work to evolve unhindered by pauses to address therapeutic technique, countertransference, and the like. Likewise, it is easier to forego the difficult task of formulating specific and thoughtful individualized feedback for each trainee, not to mention the thoroughness required to complete the lengthy evaluation forms currently required by most psychotherapy training programs. Educational efforts are crippled, though, without accurate, specific, bidirectional feedback and thoughtful evaluation, creating a potent argument for persistence in overcoming the many barriers to their provision. We as clinicians owe this a duty to our patients, specifically those that we manage from afar within the supervisory process.
In a manner somewhat similar but perhaps less pronounced than in psychodynamic psychotherapy, the termination phase of the supervisory relationship presents its own opportunity for new learning. In ‘good enough’ supervision, the supervisor becomes internalized by the supervisee. In a thoughtful termination, there is some discussion of the terms of future availability for the supervisor in either the same or a different relationship. Separation, like attachment is a powerful motivator and evokes new and often deeper feelings. It is also an important opportunity in which implicitly or explicitly, knowingly or unknowingly, the supervisor provides powerful modeling for the supervisee. It is important to set a specific date for the last supervisory session, which should be determined at least a month in advance. That date should be specific and the termination of supervision should not be minimized. Although previous formal and considerable informal feedback is likely to have taken place, there should be some use of a final supervisory session as a time of mutual evaluation. The supervisor should help the supervisee evaluate what has been learned in this supervision and what needs to be learned in future elements of psychotherapy education. Termination is a good time to review the initial supervisory goals and to specify what were disappointments, any unanticipated positive products, and what contributed to both the disappointments and serendipitous outcomes. It is also important that the supervisor ask for a genuine evaluation. However, as the power differential and administrative reporting line continue to exist, this is often the most difficult challenge. Asking for advice on how to become a better supervisor may be somewhat more productive as will discussions in which the supervisor broaches supervisor limitations that he or she knows about in advance.
Both parties should attend to absences during the time of the identified termination process. Absences will often reflect defensively minimized importance of the separation and the prior supervisory relationship. It is a particularly important time to be vigilant about ‘countertransference’ type responses both as supervisor and supervisee. Occasionally, the termination phase will produce phenomena analogous to the psychotherapeutic concept of ‘acting out’ in the form of a crisis or a rationalization for continuing the relationship in some other form.
When discussing disappointments of the supervisory relationship, it is important that both parties recognize that every relationship has its disappointments, but also that some people are more prone to disappointments than others. A particular question is structuring the final supervisory session and whether or not there will be some form of ‘gift.’ There is frequently a tendency to want to end the supervisory relationship with a celebration of some sort as opposed to a ‘typical session.’ It is best to avoid extremes. The terms of continuing engagement between supervisor and supervisee are generally more variable than that between patient and therapist. A compromise that is often satisfactory is some sort of informal lunch meeting. If that is done, the more evaluative and feedback portions of the termination phase are best done in advance of the lunch.
The terms of continuing engagement between supervisor and supervisee vary widely. Supervisors have written books on supervision with a supervisee. On the other extreme, there was an unfortunate incident of another prominent analyst omitting to tell a supervisee about a published report of their relationship, which resulted in unhappy feelings and litigation.
The authors wish to conclude with a reminder that psychotherapy supervision is both art and science and best done when it is experienced as a calling as opposed to an obligation. It is also a source of enormous professional gratification and joy. As is unfortunately the case in psychiatric, psychology, and social work education, this chapter has not given deserved attention to the education of psychotherapy supervisors. It is somewhat beyond the charge of the chapter, but it also reflective of how unevenly our major psychotherapy disciplines prepare senior members for roles as supervisors. Almost all of us support (at least in theory) psychotherapy education for new faculty, more psychotherapy supervision research, and for regular meetings of supervisor faculty to discuss the challenges, joys, and academic perspective on supervision. At a time when medical psychotherapy education takes place in an atmosphere of increasing emphasis on financial accountability and productivity, such valuable and important educational support of supervisors is achieved only with great effort on the part of departmental leadership. We support this effort enthusiastically. The support of competence in supervision will be a major determinant of the future of psychotherapy as a core element of the identity of our professions.