The application of psychotherapy to older adults began with much skepticism. Sigmund Freud believed that psychological treatment of individuals over the age of 50 was ineffective (Freud, 1904/1959). To substantiate this view he put forth claims that older adults have limitations in ego or cognitive functioning; analysis would have to deal with a relatively longer lifetime and thus would go on indefinitely; and analysis would occur at a time when it was no longer essential to be psychologically healthy. Although Abraham (1919/1927) was the first psychoanalyst to acknowledge and convey optimism about the psychological treatment of older adults, the views of Freud dominated clinical thinking at that time. However, in 1929 Lillien Martin pioneered the provision of psychotherapy to older adults at the San Francisco Old Age Counseling Center (Martin, 1944). This was the first psychotherapy program for older individuals in the USA. Martin's directive and inspirational techniques centered on overcoming pessimism by adopting the ‘will-to-do’ attitude.
In 1959, Rechtschaffen provided a landmark review of psychotherapy with older adults. In addition to providing a thoughtful summary of anecdotal and case report data, he argued that older adults are heterogeneous in terms of both their internal and external strengths and resources, as are young adults, and challenged the widely held notion that older adults could not benefit from psychological intervention. Since Rechtschaffen's review, this line of work has continued to grow with a number of key summaries of the then current state of the psychotherapy field (Brink, 1986; Knight, 1986; Gallagher-Thompson and Thompson, 1995). Two reviews stand out for their comprehensiveness (Teri and McCurry, 1994; Gatz et al., 1998). In particular, Gatz et al. (1998) categorized psychological treatments for older adults in terms of empirically validated criteria developed by the American Psychological Association's (APA) Division of Clinical Psychology and offered important guidance for empirically-based practice.
In addition to the accumulation of general scientific knowledge of the psychology of older adults (i.e., cognitive functioning, stress, and coping, etc.; for a historical review of the growth and development of the psychological study of older adults, see Cook et al., 1998), the field of geriatric mental health intervention research has blossomed, particularly in the area of depression. The completion of randomized and quasi-randomized controlled trials of psychotherapy with older adults represents an excellent step forward in the direction of more effectively serving the elderly population. Furthermore, there is a strong federal push in the USA for the geriatric mental health intervention field to move away from the traditional clinical trials model towards a more public health model of treatment (Lebowitz and Harris, 2000), and to place greater emphasis on treatments that are more broadly accessible and acceptable, rather than confined to the select samples of older adults that have been studied in clinical trials in specialty settings.
Demographic projections estimate that the number and proportion of older adults in the population is increasing in industrialized countries. In North America, the proportion of the population over 65 years of age is predicted to grow from 12.3% in 2000 to 20.2% in 2035 with the population over 80 years of age rising from 3.2% in 2000 to 6.0% by 2035. (All demographic data provided by United Nations, 2003). Among those over 65 years of age in 2035, women will out number men in an approximate ratio of 1.7:1. The elderly dependency ratio, the number of older adults to working adults, was 19 to 100 in 2000, and is predicted to grow to 33 to 100 by 2035. By 2035 there will be an estimated 261 000 people over 100 years in North America.
Europe has more of a demographic crisis than North America. In the UK in 2035, for example, the elderly dependency ratio will be 37 to 100 adults of working age. In all industrialized countries, however, the trend towards an increasing elderly dependency ratio fizzles out in 2035 with the proportion of over 65 years old stabilizing by 2050. Over the next 30 years, the aging population will create a significant rise in the number of dependent older people. By 2035 in North America there will be 85 million older people. Approximately 10% are expected to need institutional care. The 30–40% living alone are expected to have an increased need for social and medical services (Grundy, 1989). This translates to an extra 4 million nursing or residential homes and approximately 15 million additional older people living alone. It is essential to plan ahead for these changing demographics, whose greatest acceleration towards an aging population will be between 2015 and 2025 before gradually reaching a static position in 2050.
Western societies have only recently begun to identify ageism as a source of prejudice and discriminatory practice. On the surface this is surprising given that aging is universal, although demographically, older people have traditionally been a minority group. Denial-based psychological defenses may serve the purpose of separating the self from an unrealistically idealized concept of older people in an attempt to avoid the realities of one's own aging (Hepple, 2003a). There are numerous stereotypes about older adults, which can adversely affect a psychotherapist's attitude and behavior. Namely, that older adults are: (1) a homogeneous group; (2) generally alone and lonely; (3) sick, frail, and dependent on others; (4) living in segregated housing for the elderly or nursing homes; (5) often cognitively impaired; (6) often depressed; (7) difficult and rigid; and (8) not coping well with the physical and intellectual decline associated with aging (APA Working Group on the Older Adult, 1998). Overidealized stereotypes of older adults can similarly be unhelpful by minimizing the challenges of aging (‘You are only as young as you feel,’ for example). On the contrary, older adults are a heterogeneous group who, in general, maintain close contact with family, live independently, and adjust well to the challenges of aging (APA Working Group on the Older Adult, 1998). Usually, older adults’ personalities stay consistent throughout the life span, with proportionally few suffering from major mental health problems (APA Working Group on the Older Adult, 1998). Although there may be some decline in intellectual abilities, debility is typically not severe enough to cause problems in daily living.
In this section, theoretical perspectives and relevant empirical evidence are briefly summarized. For those general therapeutic orientations that are well known, the actual description of the therapy is limited. For those treatments that are primarily or only used in older adults, a more detailed account is provided.
Cognitive-behavioral therapy (CBT) has been one of the most widely studied and efficacious treatments for older adults. Though it includes a variety of interventions ranging from the cognitive work of Beck et al. (1979) to the behavioral work of Lewinsohn et al. (1976), its most common application is a blend of both cognitive and behavioral techniques. The conceptualization underlying CBT is that much of psychopathology is learned and maintained by a combination of distorted, dysfunctional thinking about oneself and the world and reduced behavioral or environmental reinforcement. Thus, therapeutic intervention seeks to change unhelpful thinking, increase positive behaviors, and reduce negative actions. CBT is typically highly structured, directive, time-limited, and focused on current problems.
The CBT model has been widely used for many disorders in older adults and reported in case reports and empirical investigations. A series of studies by Gallagher-Thompson et al. have shown that CBT is highly efficacious for depression (Thompson et al., 1987; Gallagher-Thompson and Steffen, 1994; Thompson et al., 2001; for a more thorough summary see Teri et al., 1994). In particular, there is evidence for its efficacy with depressed outpatients and inpatients, the medically ill as well as healthy, in individual or group format, and when delivered by a trained therapist or self-taught through bibliotherapy (Scogin et al., 1987, 1989, 1990). Relative to the stringent criteria of the APA Task Force on empirically supported treatments, CBT was identified as ‘probably efficacious’ for treatment of depression in community residing older adults who are cognitively intact, have minimal comorbidities, and are not suicidal (Gatz et al., 1998). In addition, cognitive-behavioral forms of therapy have demonstrated efficacy for alleviating sleep disturbances (for review see Morin et al., 1994 and Gatz et al., 1998), generalized anxiety (Wetherell et al., 2003), and behavioral problems associated with dementia (Teri et al., 1998; Allen-Burge et al., 1999). A case example illustrating the use of CBT with a depressed elder is presented later in this chapter.
A wide variety of treatments are offered under the rubric of psychoanalytic/dynamic therapy, including insight-oriented and supportive approaches. Many of them concern the historical causes and larger patterns of current behavior, restoration of healthy defenses and positive self-perception, and examination of the client–therapist relationship. This treatment is typically less directive, and often seeks to help identify and resolve unsettled issues from earlier in development and explore their impact on current functioning.
From a psychodynamic perspective there are some unique developmental tasks and transferences to be addressed in therapy with older adults. These age-appropriate themes include grieving for losses, fear of physical illness, disability and death, and guilt and despair over past failures (Pfeiffer and Busse, 1973; Hildebrand, 1995). One specific developmental tension that is beautifully illustrated in Shakespeare's King Lear and The Tempest, is the dialectic between the decline and sense of impending death that is associated with aging versus growth and liberation (Deats, 1996; Hildebrand, 2000). Transference issues are atypical, but may reflect concerns related to one's family of procreation (i.e., spouse and children) rather than one's family of origin; while countertransference may be influenced by unresolved issues with parents, one's own fears of aging and/or negative cultural stereotypes regarding aging (Gallagher-Thompson and Thompson, 1996).
Unfortunately few empirical investigations have examined the efficacy of psychodynamic therapy for use in older adults. A study by Thompson et al. (1987) demonstrates that brief psychodynamic psychotherapy is equally efficacious in the treatment of major depressive disorder in older people as behavioral and cognitive interventions. Seventy percent of subjects showed remission or significant improvement after 16–20 treatment sessions compared with minimal spontaneous improvement in a delayed-treatment control group. Although it has an extremely small sample size and no control group, the work of Lazarus et al. (1984, 1987) provides some promise that psychodynamic therapy is useful for older adults (for an excellent though less current review, see Newton et al., 1986).
One time-limited integrative therapy with a heavy influence on psychodynamic conceptualization and technique is cognitive analytic therapy (CAT; Ryle, 1990). This structured therapy has two primary influences, as its name implies, cognitive-behavioral and psychoanalytic. CAT is gaining popularity in the UK and Europe, and its application with older adults has recently been discussed (Hepple, 2002). Its premise is that experience about oneself in relation to others becomes internalized in early development as a repertoire of reciprocal roles that act as templates for subsequent interactions. Insight and change are promoted through the exploration of these experiences in the here and now, particularly the therapeutic relationship, using a variety of cognitive, behavioral, interpretative and creative tools and techniques. CAT has not yet been formally evaluated, but has been suggested as potentially beneficial for treatment-resistant depression or dysthymia, stable personality difficulties with traumatic or abusive antecedents, and somatization disorders (Hepple, 2002).
Interpersonal psychotherapy (IPT) has multiple theoretical underpinnings, including psychodynamic, and has received empirical support with older adults (Klerman et al., 1984). This treatment is manual-based, highly structured, and short term. Its underlying premise is that regardless of the etiology of psychopathology, understanding and renegotiating relationships plays a key role in reducing symptoms, restoring function and possibly preventing future disturbance. IPT focuses on current relationships in four general problem areas: role transition, role dispute, abnormal grief, and interpersonal deficit.
Monthly IPT sessions demonstrated efficacy as a monotherapy and in combination with antidepressant pharmacotherapy as a maintenance treatment strategy to prolong recovery and prevent recurrence of major depression (Reynolds et al., 1999). The older patients in this randomized clinical trial had had current major depression and at least one prior episode during the past 3 years. Combination of IPT and antidepressant medication not only improved duration of recovery but social adjustment as well (Lenze et al., 2002).
In addition to a review of IPT as applied to late-life depression, Miller et al. (2001) have reported preliminary findings on IPT combined with antidepressants in cognitively impaired depressed elders. Uncomplicated bereavement-related depression also responds well to IPT (Miller et al., 1994). Additionally, this type of counseling has been shown effective in the treatment of subsyndromal depression in postsurgical patients following hospital discharge (Mossey et al., 1996).
Reminiscence therapy (RT) involves recalling the past as a way to increase self-esteem and social connection. RT typically occurs in a group format in which individuals are encouraged to remember and share memories of the past, with personal artifacts, newspapers, and/or music often used to stimulate memories. These sessions are frequently structured with the therapist picking the topic. This very popular counseling tool is regularly used with well elderly to gain perspective on their lives and thus is popular in senior centers, residential settings, and retirement communities rather than as clinical intervention for those older adults with major mental health or personality disorders (Thorton and Brotchie, 1987; Gatz et al., 1998).
Life review therapy (LRT: Butler, 1963), a more intense type of RT, involves the reworking of past conflicts in order to gain a better understanding and acceptance of the past. These types of therapies are based on the work of Erik Erikson (1959, 1982) and his eight-stage model of psychosocial development. The underlying premise is that an older adult can be helped through the last stage of Erikson's model, ego integrity versus despair. It is thought that if older adults can satisfactorily formulate and accept personalized answers to existential questions such as, ‘Who am I?’ and ‘How did I live my life?’, they will achieve integrity. As this treatment is so individualized, it is difficult to manualize; however, Haight and Webster (1995; Webster and Haight, 2002) have done so. Although LRT involves various therapeutic approaches, not all of which are clearly defined (Haight et al., 1997), effect sizes of 1.05 have been reported for LRT versus no treatment in controlled therapy studies of geriatric depression. However, superiority over a no treatment comparison condition does not demonstrate specific efficacy for the particular brand of therapy. A case series of older trauma survivors with posttraumatic stress disorder successfully treated with LRT was recently reported (Maercker, 2002); thus, this may be a good therapy for clients that need to focus on/confront past trauma issues.
Unfortunately, the application of family therapy with older individuals remains underdeveloped, and research investigating its efficacy is virtually nonexistent (Qualls, 1995; Knight and McCallum, 1998). One area in which there may be an increased demand and relevance is therapy with families caring for a cognitively impaired elderly member (Bonjean, 1988; Qualls, 2000). Individual and family therapy for spouse-caregivers and families of Alzheimer disease patients was efficacious in postponing nursing home placement. Family therapy may be used as a separate modality or to elicit family members’ involvement as facilitators of individual therapy for older individuals.
Another area in need of further investigation is the application and provision of psychotherapeutic services to those with cognitive impairment. A significant minority of the elderly population experience limitations in their cognitive abilities due to progressive dementia, and many of these individuals also experience comorbid emotional distress. Owing to their cognitive deficits, such as memory loss or decreased capacity for judgment and problem solving, persons with dementia are usually not considered to be good candidates for traditional psychotherapy. However, the symptoms and behaviors of persons with dementia should not be viewed solely as manifestations of biology, but rather, as being affected by social, psychological, and environmental contexts as well (Kasl-Godley and Gatz, 2000). Thus, patients with dementia are able to derive some benefit from psychological interventions. Various CBT, environmental, and supportive interventions may help cognitively impaired older adults reduce disruptive behaviors and excess disabilities, increase or maintain positive behaviors, improve memory or learn coping skills to manage loss of cognitive skills, increase quality of life, reduce excessive burden on health-care delivery systems, alleviate symptoms of depression or anxiety, or help adjustment to multiple losses (Gatz et al., 1998; Kasl-Godley and Gatz, 2000). Research on the degree to which cognitive deficits operate as moderators to limit their use (e.g., within what ranges of cognitive dysfunction traditional talk therapies can be used effectively, and with what modifications) is needed.
Many psychosocial interventions currently in use with older adults with dementia are based on uncontrolled case studies and anecdotal reports. However, there are some studies examining the feasibility of conducting therapy or the effectiveness of therapy for particular purposes with older adults (for reviews, see Cheston, 1998; Gatz et al., 1998). Use of behavioral and environmental treatments for behavior problems and memory and cognitive retraining for some forms of late-life cognitive impairment may be effective. However, there is much dispute about cognitive training, in particular. Support groups and CBT can assist those with early-stage dementia to foster coping strategies and reduce distress. RT may provide mild to moderate stage individuals with interpersonal connections. Behavioral approaches and memory training target specific cognitive and behavioral impairments and help to optimize remaining abilities.
One intervention that is often used with memory-impaired older adults is reality orientation (RO), which involves exposing cognitively impaired patients to stimuli that facilitate orientation to time or place (for a manual, see American Hospital Association, 1976). The most widely used type of RO takes place anywhere from once a week to several times a day and involves the rehearsal of basic orientation facts such as the day, date, time, and the weather. In 24-hour RO, patients are reoriented on the nursing home units throughout the day, either by staff or environmental cues such as big clocks and calendars.
Other types of therapies such as problem-solving therapy and eclectic approaches are also being applied to older individuals. For more information, the interested reader might seek Duffy (1999) or Frazer and Jongsma (1999).
As previously noted, the most widely researched disorder in the geriatric mental health field is depression. In 1991, the US National Institute of Health convened a panel of experts from the biomedical and behavioral sciences to address the diagnosis and treatment of depression in late life (National Institutes of Health Consensus Development Panel on Depression in Late Life, 1992). Since then, an update from the consensus conference has been published (Lebowitz et al., 1997) as have numerous reviews, including Areán and Cook (2002). Despite widespread knowledge of the efficacy of major treatment modalities for some disorders or problems occurring in old age, there are still numerous areas in the field in need of further investigation. A brief review of the noteworthy areas follows.
Most industrialized countries report that suicide rates rise increasingly with age, with the highest rates occurring for men age 75 and older (Pearson and Conwell, 1995). In a comparison of age differences in suicidal intent in psychological autopsy studies, older adults were more likely to have avoided intervention and taken precautions against discovery and were less likely to communicate their intent to others, as well as less likely to have a history of previous attempts (Conwell et al., 1998). These distinctive features present a challenge to detecting and treating high-risk elderly. Although suicide in older adults is a major public health problem, there are as yet no effective interventions for reducing suicidal behaviors in this population (Pearson and Brown, 2000). However, given the strong relationship of depression as a risk factor for suicide, improving the detection and treatment of late life depression in primary care settings, where older adults often seek treatment for emotional difficulties, seems to be a promising approach (Brown et al., 2001).
Studies of bereavement-related distress, now referred to as complicated or traumatic grief reactions, have begun (Frank et al., 1997). Clinical researchers at the University of Pittsburgh's Western Psychiatric Institute and Clinic have completed an open treatment trial of traumatic grief therapy conceptualized and treated similar to exposure therapy for posttraumatic stress disorder (e.g., reliving the moment of death, saying goodbye to the deceased, and in vivo exposure to situations that clients have been avoiding since the death) (Shear et al., 2001). This protocol appears to be a promising intervention for debilitating grief in older adults.
Alcohol abuse is common among older adults, with roughly 12% of older women and 15% of older men regularly drinking in excess of limits recommended by the National Institute of Alcoholism and Alcohol Abuse (i.e., no more than one drink per day; Adams et al., 1996). Hazards of drinking among older adults may include increased risk for falls, accidents, and interference with medications. Alcohol abuse may also present differently in the elderly, as the level of drinking necessary to be considered hazardous is lower than the level for younger people, and many late-onset alcoholics do not develop dependence (Levin et al., 2000). However, there is reason to hope that elder-specific interventions can lead to reductions in alcohol consumption (Blow and Barry, 2000). Several large-scale projects have shown promising outcomes with interventions of varying length, most notably Project GOAL—Guiding Older Adult Lifestyles (Fleming et al., 1999), the Gerontology Alcohol Project (Dupree et al., 1984), and the Michigan Outcomes Study (Barry et al., 2001). Project GOAL demonstrated that 15–20 minutes of physician provided advice and education about the negative consequences of excessive drinking can significantly reduce frequency of excessive drinking. More lengthy interventions utilize motivational interviewing techniques (Miller and Rollnick, 1991) and/or skills training (Dupree and Schonfield, 1999). Structured nonconfrontational techniques that reinforce values incompatible with drinking (e.g., maintaining good health) and teach coping skills for avoiding alcohol in high-risk situations (e.g. bereavement) have shown comparable outcomes among older and younger adults (Blow and Barry, 2000). More effort is needed to bring these interventions into primary care and community settings.
Techniques for treating certain mental health problems, such as anxiety disorders, prescription medicine misuse (i.e., benzodiazepine), personality disorders, and psychoses, have been sorely lacking (Gallo and Lebowitz, 1999). Epidemiological evidence indicates that anxiety disorders are more prevalent than either depression or severe cognitive impairment among older adults (Regier et al., 1988). However, despite its prevalence, very little psychotherapy intervention research has been conducted on anxiety (for reviews, see Niederehe and Schnieder, 1998; Wetherell, 1998).
One noteworthy investigation was the randomization of older adults with generalized anxiety disorder (GAD) to the CBT group, a discussion group organized around worry-provoking topics, or a waiting period (Wetherell et al., 2003). Older adults in both active conditions improved relative to the waiting-list; however, CBT showed large effects while the discussion group showed medium-sized effects. These results provide limited support for the superiority of CBT to a comparison intervention.
Additionally, a version of CBT that targets the needs of older adults with GAD in the primary care setting was preliminary tested against usual care (Stanley et al., 2003). Outcome data suggested significant improvements in worry and depression after CBT relative to usual care.
Mohlman et al. (2003) are the first to test the efficacy of CBT as compared with an enhanced version (ECBT) that included learning and memory aids such as homework reminders and troubleshooting calls, and a weekly review of all concepts and techniques for treatment of late-life GAD. ECBT resulted in improvement on more measures and yielded larger effect sizes than standard CBT, when each was compared against a wait-list control group. These findings provide evidence that content and procedural modifications may be necessary to maximize the effectiveness of CBT therapy with older people with mild cognitive impairments.
Prescription medication misuse may be a particular problem for older adults, in particular the use of benzodiazepines (Gallo and Lebowitz, 1999). Anxiolytic medications are the most common treatment for anxiety in older adults and benzodiazepines figure prominently (Blazer et al., 1991). In addition, benzodiazepines are commonly prescribed and used for depression, insomnia, and other sleep disturbances in older individuals. Despite the expressed concern of the American Psychiatric Association (1990) Task Force Report on Benzodiazepine Dependency regarding the ‘appropriate therapeutic use, toxicity, abuse and risk of inducing a drug-dependent state’ in older adults, there are reasons to believe that use is high and often inappropriate (Hanlon et al., 2002). The serious negative side-effect profile, including associations with significant morbidities such as sleep disturbance, cognitive difficulty, impairment in activities of daily living, motor vehicle crashes, and problems with gait (e.g., accidental falls and fall-related fractures) has been well-established (Bertz et al., 1997; Hemmelgarn et al., 1997; Hanlon et al., 1998; Ray et al., 2000). Though pharmacotherapy has been successful in reducing or eliminating benzodiazepine misuse, CBT has also been shown effective in helping older individuals successfully discontinue or reduce inappropriate use (Gorenstein et al., in press; Morin et al., 1995).
As in younger populations, older adults with personality disorders may be less willing to engage, adhere, and benefit from traditional mental health interventions (Lynch et al., 2003). Although to date no outcome study has specifically focused on treating personality disorders in older adults, evidence from case reports and data on effects of personality pathology on treatment of depression suggests that this is a worthy area of future investment (for a recent review, see DeLeo et al., 1999). Pilot data provides preliminary evidence for the feasibility of applying dialectical behavior therapy (Linehan, 1993) to depressed older adults, a significant minority of whom meet criteria for a personality disorder (Lynch et al., 2003). It has been suggested that the increase in life events and disability found in later life may ‘unmask’ maladaptive personality traits that have been dormant in mid-life; the concept of reemergent borderline personality traits (Hepple 2003b for a review of this area). Distress and behaviors arising from this can often be misconstrued as resulting from organic pathology. A clinical case example is presented later to help illustrate this point.
Although there is a large scientific knowledge base on schizophrenia among younger adults, much less is known about late-life schizophrenia and its treatment (Palmer et al., 1999). What is known about its treatment is mainly pharmacological, the use of conventional neuroleptics and the newer serotonin–dopamine antagonists (Jeste and McClure, 1997). However, recently Patterson et al. (2003) developed and evaluated a psychosocial intervention to improve everyday living skills of older patients with schizophrenia and other chronic psychoses. Preliminary findings suggest that older patients with longstanding psychotic disorders may benefit from participation in this skills-training program.
There are a growing number of older individuals who reside in long-term care settings. A US network termed Psychologists in Long-Term Care has developed standards for psychological practice in long-term care facilities (Lichtenberg et al., 1998). Other guidelines and resources for professionals exist, such as information on competency determinations, work within the structure of an interdisciplinary team, and staff development (US Department of Veterans Affairs, 1997; Gallagher-Thompson et al., 2000b; Zeiss and Gallagher-Thompson, 2003).
There are numerous physical, psychological, cognitive, social, developmental, and environmental factors that can impact the choice and delivery of psychotherapy to older adults. Most older adults have at least one chronic medical illness, some degree of functional impairment/disability, an increasing frequency of loss events, and a decrease in controllability of these losses (e.g., financial limitations, diminished sensory capacities, decreased mobility, retirement, widowhood, and change in residence). The complexity of these intermingling influences often merit special therapeutic consideration.
Although some mental health interventions are comparable with those used with younger individuals, it is often necessary to adapt therapies to address special considerations unique to older adults. For example, psychotherapy with older adults often occurs at a slower pace due to possible sensory problems and slower learning rates (Gallagher-Thompson and Thompson, 1996). This means that repetition is very important in the learning process, and information should be presented in both verbal and visual modalities (i.e., on chalk boards and hand-outs) in order to help older patients encode and retain information. Older clients should also be encouraged to take notes to help aid memory retention and thus increase efficacy of therapy (Knight and Satre, 1999). Assignments may need to be in bold print or sessions tape-recorded for review. Additionally, psychotherapy with older adults often requires a collaborative style with few clearly outlined goals and a more active or task-focused approach (Gallagher-Thompson and Thompson, 1996).
The goals of psychotherapy with older adults should be continually highlighted to reinforce the purpose and facilitate the direction of treatment. It may also be necessary to facilitate therapy for those with sensory problems, particularly hearing and vision impairments. Thus, adaptations such as pocket talkers to assist in hearing or eliminating glare for the sight impaired should be made available. Rather than giving suggestions or expecting the client to infer answers, Knight and Satre (1999) suggest that as there is a normal age decline in fluid intelligence, therapists may need to lead the older adult to conclusions.
When determining if and which modifications are needed, it is important to separate the effects of maturation from the effects of cohort (Knight and Satre, 1999). Maturational effects include similarities that are developmentally common or specific to older adulthood, such as adjusting to chronic illness and disability, or loss of friends and family due to death. Cohort effects are specific to a certain birth-year-defined group. For example, in the USA, early-born cohorts have lower educational levels and less exposure to psychological concepts (Knight and Satre, 1999). Psychotherapists working with older people need to be aware of maturational and cohort differences in the expression and treatment of psychological problems. Additionally, therapists working with older adults should learn about chronic illness and its psychosocial impact, management of chronic pain, factors influencing adherence to medical treatment, rehabilitation methods, and assessment of behavioral signs of negative medication effects (Knight and Satre, 1999).
Assessment should always include current mental and cognitive status (for further information on modifications of assessment techniques for use with older adults, see Zarit and Zarit, 1998). A brief screen of cognitive functioning, such as the Mini-Mental State Exam (MMSE; Folstein et al., 1975), can measure suitability for treatment, as well as identify patients in need of more extensive neuropsychological testing. It is also imperative to consider the medical status of and social support available to older adults, as these may affect presentation and treatment of pathology (APA Working Group, 1998). Formal testing, such as the MMSE, requires normative data specific to older adults in the reference group of the person being tested (e.g., education, race, gender). Without such normative data, ‘normal’ aging processes are impossible to distinguish from pathology or impairment (Dougherty and Chamblin, 1999).
Providing psychological services to older adults often requires flexibility in scheduling, location and collaboration. Older adults often have a greater chance of hospitalization or reduced mobility, responsibility to care for infirm relatives, or a reluctance to travel in bad weather conditions, all of which may necessitate missed therapy sessions (APA Working Group on the Older Adult, 1998). Thus, brief, occasional hospital visits, telephone sessions, or letters may need to be made at times to maintain contact. Access to building and acceptable transportation services should be made available (Hepple, 2002). Additionally, because older adults often have concurrent physical and social problems, consultation and coordination with other health service providers is often necessary (APA Working Group on the Older Adult, 1998).
At times, when an older adult becomes temporarily dependent upon a caregiver for assistance, it may be crucial to engage the caregiver in aspects of the treatment. An example of this is the pivotal work by Teri et al. (1997) of treating depression in older dementia patients via training caregivers in behavioral interventions. An excellent case example, which describes in detail a systematic course of CBT for a depressed female caregiver of an Alzheimer's disease patient, is described elsewhere (Dick and Gallagher-Thompson, 1995). Goals of that treatment, not uncommon to other caregiver stress experiences, included setting limits and making time for personal needs. Treating the caregiver in individual or group, dyadic or brief educational sessions can be directly beneficial to the caregiver and indirectly helpful to the care recipient. If a caregiver is taught to understand and more effectively cope with emotions such as frustration and anger, they may be less distressed and better able to provide effective care (Gallagher-Thompson et al., 1992).
Because many older adults have experienced increased loss of family members or friends compared with younger individuals, clinical lore suggests that the therapeutic relationship becomes a vital source of support as well as information. For this reason, it has been suggested that rather than traditional termination, ending sessions be spread out and booster sessions be offered (Gallagher-Thompson and Thompson, 1996). A suggested acronym to help therapists working with older adults provide respectful and appropriate therapy is MICKS: ‘a) use Multimodal teaching, b) maintain Interdisciplinary awareness, c) present information more Clearly, d) develop Knowledge of aging challenges and strengths, and e) present therapy material more Slowly’ (Crowther and Zeiss, 1999).
Clinical lore also suggests that many older adults hold negative stereotypes about mental health and psychotherapy, which may result in reluctance to accept or engage in therapy, limitations in self-disclosure and endorsement of symptoms. Some of these myths follow: only crazy people seek mental health treatment; psychological problems indicate moral weakness; therapy constitutes an invasion of privacy; adults, especially men do not share their feelings or show weakness to strangers; adults do not need to ask for help; and therapy has no relevance (Glantz, 1989). Thus, one additional adaptation for therapy with older adults may be to have an introductory orientation/socialization into psychotherapy. Here incorrect assumptions or fallacies can be corrected, and roles and expectations established. It is important to remember that there is much more commonality between the young and the old than there are differences, and that older people have a huge diversity of life experience having matured in a world of unprecedented change, where wars, mass migration, and rapid technological development changed many aspects of life beyond recognition for many individuals. Psychotherapists, although benefiting from the specialized skills and approaches utilized in work with older people, need to bear in mind that what is shared with their older clients is humanity and that what is different may take some understanding.
How best to choose an optimal form of psychotherapy for an older adult patient is influenced by a number factors, including diagnosis, cognitive functioning, and psychological-mindedness. Choice of therapy is often based on therapist awareness of and training in available therapies. However, considerations impacting the choice and delivery of intervention include knowledge of efficacy of intervention with older adults, likelihood of effectiveness for the particular patient (e.g., skills), severity and timing of problem (e.g., acute versus chronic), timing of intervention, patient preference and motivation, and ethnic and cultural considerations (Hepple et al., 2002). Other factors to consider are previous treatment history and response. Two case illustrations are presented here from two different theoretical orientations, CBT and CAT.
Although several excellent examples of CBT and its application to older adults have been presented elsewhere in case report form (Dick and Gallagher-Thompson, 1995; Crowther and Zeiss, 1999; Karel et al., 2002), a brief highlighted review of a treatment case is described here to help illustrate the applicability of CBT conceptualization and practice with older individuals. A manual that describes this approach is available for both therapist and client (Dick et al., 1995; Thompson et al., 1995). Additionally, Coon and Gallagher-Thompson (2002) utilize case vignettes to illustrate CBT homework challenges and successful approaches to address adherence barriers.
Mrs W was a 79-year-old, widowed, retired, Caucasian woman who sought treatment for depression at the Older Adult and Family Center at the VA Palo Alto Health Care System. Her symptoms at this time warranted a diagnosis of major depressive disorder and dependent personality features. Mrs W's husband had passed away about 2 years prior and her two sons had moved to a different state. She reported intense feelings of loneliness, disappointment, and frustration that her physical ailments (i.e., congestive heart failure with edema and shortness of breath) had made her less mobile and more dependent on others.
A program of individual weekly CBT was initiated beginning with an introduction to the CBT model and Mrs W was encouraged to apply the skills learned in session outside of therapy (i.e., via homework assignments). In order to help reduce depressive thoughts about herself, she was taught to use a daily thought record, and trained in challenging negative beliefs. In order to increase engagement and enjoyment in pleasant events, the client was taught to the use mood monitoring and activity tracking.
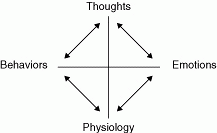
The first session, included thorough history taking, a description of current problems, and completion of assessment measures, such as the MMSE (Folstein et al., 1975), and the Beck Depression Inventory (BDI; Beck and Steer, 1987). At the end of the first session, the therapist presented an introduction to the cognitive-behavioral model of depression on a whiteboard (e.g., how thoughts and behaviors affect functioning, see Figure 32.1) and using materials the client had talked about gave examples of the antecedent, belief, and emotional consequences. The client was easily able to summarize the model and was asked to read material on CBT.
At the beginning of every session, Mrs W completed the BDI to monitor depressive symptomatology. In the second session, the collaborative nature of the relationship between the therapist and client and the importance of practicing new skills learned in session (e.g., homework) were discussed, specific goals of therapy were outlined, and the CBT model was revisited. Mrs W was reminded that CBT was a short-term treatment and that goals must be manageable within the time allowed. Her target complaints were she would like to be cured of her depression and would like to find more satisfying things to do with her life. In session 3, Mrs W was taught how to notice and monitor ‘unhelpful thoughts’ following stressful events. This involved introducing her to an unhelpful thought diary (three columns: antecedent, belief, and emotional consequences). In order to help Mrs W understand the impact and strength of her thoughts on her mood, she was taught to assign a belief rating from 0 (not strong at all) to 100 (completely true) to each thought. A useful analogy was used to help her understand the effects of unhelpful thoughts on mood: listening to a radio station with a headset. It was explained that if the headset is clear, if it is correctly connected to the radio receiver and positioned securely on one's head, then the station will come in clearly (Thompson et al., 1995). It was further explained that if the headset is not on properly, there may be misinterpretation of the signal or information from the radio. A list of unhelpful thoughts entitled ‘Signals from your negative headset’ was given to Mrs W and the therapist explained negative distortions such as attaching negative labels of oneself, having unrealistic expectations for oneself, viewing a situation in terms of extreme outcomes, and tendency to blow events out of proportion. The therapist and Mrs W worked together to identify examples from the patient's current life. Over the next several sessions, Mrs W was taught how to challenge her unhelpful thoughts (e.g., challenging their validity). She was given a list of techniques entitled ‘Fine tuning your signal’ that included challenges such as engaging in specific behaviors to obtain additional information in challenging unhelpful assumptions, considering alternatives, and weighing the advantages and disadvantages of maintaining a current thought, emotion, or behavior.
|
|
Fig. 32.1 Cognitive-behavioral model. |
Through individual sessions and homework assignments, Mrs W was able to challenge her own thinking as well as allow the therapist to provide her with new information that challenged her unhelpful thoughts. Mrs W was able to recognize that she was recognizing only negative aspects of her current situation and discounting positive accomplishments (see Box 32.1 for partial completion of homework assignment). She was attaching a negative label to herself and sending herself negative messages, such as ‘I'm dumb,’ because of age-associated impairments. Attributing these limitations to aging and not to self was a step toward recovery for Mrs W.
‘I'm dumb.’
Where's the evidence?
What are alternative explanations?
1A. I have trouble opening bottle caps, fastening doors, putting cartons together, folding maps. Things just about anyone can do.
1B. I am not mechanically inclined. My hands are also stiff, sore, and fingers are bent and misshapen. It is hard for me to get a good grip on jar and bottle caps. Also reduced strength. Also the anemia makes me weak.
2A. I don't have a VCR because I have no idea how to hook one up or even play it. I'd like to have one too! I had to have my son hook up my TV and hi fi because I couldn't understand the instructions. The same with telephones, clocks, etc. When my husband was alive, he always did it.
2B. Again, I am and never have been mechanically inclined. I've always depended on my sons and husband to do things. I think I will have to be more patient and take more time reading and following the instructions.
3A. I had a beautiful brand new sewing machine that I couldn't use because I couldn't understand the directions for doing all the stitches, or for putting the various attachments on. I could do straight stitching but that's all.
3B. Much the same as the above. I went to the store for lessons on how to do these things. However, the instructor did the exercises and just let me watch. I do better with hands on experience and I should have told them to let me do it while they watched and guided me. I have to do the maneuvers as well as the instructions.
4A. I never was able to knit or crochet or do any kind of fancy work. I can't even get the ‘hang’ of sewing any more.
4B. Knitting, crocheting, or fancy work were just not too interesting. I just couldn't get the feel for them. I do or did a lot of other kinds of artwork. Flower arranging, beautifully decorated gift packages, Resin art. I could sew pretty well. I was an excellent cook, not good at baking, but I could do many other kinds of cooking. I kept my family well fed, and they always enjoyed my cooking. So did my friends. I gave beautiful dinner parties, holiday parties, etc.
Mrs W did not drive and since her husband's death had abandoned pleasant activities due, in part, to transportation problems. It was important to get her reactivated behaviorally. Mrs W completed the Older Person's Pleasant Events Schedule (OPPES; Hedlund and Gilewski, 1980; Gallagher and Thompson, 1981) a self-report measure designed to measure frequency of engagement in pleasant activities and perceived enjoyment of the activities regardless of whether or not they had been undertaken. She was encouraged to take part in events that once gave her pleasure in which she was no longer engaging (i.e., take an art and computer class) and to increase socialization by broadening her opportunities for social contact. The therapist helped Mrs W arrange transportation to a local senior center to better occupy her daytime hours, a time during which she was home alone. She reported that doing so lessened her feelings of loneliness and her dependency on other care providers. Additionally, Mrs W was encouraged to reconnect with friends from her childhood via telephone and postal mail. Mrs W completed a 15-session course of CBT for depression. At the end of treatment she noted that she had made significant gains in reducing her depression and had regained previously forgotten hobbies.
Mrs S was a woman in her late seventies who presented to mental health services in the UK for the first time following the death of her husband. She complained of feelings of depression, panic, ‘nameless dread,’ and a variety of unexplained physical symptoms. She felt suicidal at times and had taken an overdose of sleeping tablets on two occasions. She found it very difficult to be alone at home and her nocturnal calls to neighbors, her daughter, and emergency services had become problematic. After two admissions to an older persons’ psychiatric inpatient unit the team felt at a loss as to how to help Mrs S. She did not show signs of pervasive depression and often acted as the ‘life and soul’ of the unit, entertaining other patients with her dramatic and musical skills. Her mobility deteriorated, however, although staff felt this was under ‘voluntary control’ and she needed a great deal of staff time and attention for physical care.
As discharge approached, her physical abilities seemed to deteriorate and she became more anxious, depressed, and in need of reassurance. Attempts at discharge to her home resulted in a rapid escalation of suicide threats and emergency phone calls, resulting in readmission.
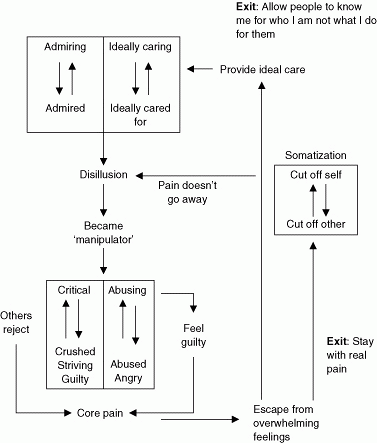
Following a series of individual sessions with a psychologist using a CAT approach, it became clear that Mrs S had a borderline personality constellation that had reemerged following the death of her husband whom she had nursed for many years. She was the oldest of five siblings and had to become a ‘parental child’ towards her siblings to avoid her mother's criticism and physical abuse. In session 3 she disclosed sexual abuse occurring over many years by her father (which she had not disclosed to anyone before). Disclosing this material was very upsetting for Mrs S but staff noticed that her physical problems and dependency improved and she was more likely to talk about real feelings rather than physical symptoms or ‘nameless dread’. By processing the core pain of the abuse, even at this stage of her life, Mrs S was able to gain insight into her patterns of somatization and becoming ‘the manipulator’ to escape from the distress of helplessness, anger, and guilt. Figure 32.2 highlights this pattern.
The emotional pain had been uncovered in late life due to her husband's death and the breakdown of Mrs S's defensive procedure in which she behaved ‘as if’ she were an ideal care provider to her husband (and deny her own needs). After the sessions ended Mrs S was able to choose to move into a residential home setting and did not re-present to services in the following 5 years.
There are numerous areas in need of further investigation in the treatment and provision of services for older adults with mental disorders, including issues of ethnicity and cultural diversity and how and where psychotherapeutic services can best be provided to older adults.
Relatively little is known about ethnic and cultural diversity in older individuals and how these factors may influence psychotherapy engagement, adherence, and outcome. This is particularly important as the number of ethnically and culturally diverse elders is projected to increase (US Department of Health and Human Services, 2001), and the significant minority in need of mental health services have not been well represented in mental health clinics or in psychosocial research (Areán and Gallagher-Thompson, 1996). Several authors have discussed psychotherapists’ need for cultural competence in the provision of clinical services to these elders and the barriers to recruiting and retaining them in treatment (Areán and Gallagher-Thompson, 1996; Lau and Gallagher-Thompson, 2002). One innovative culturally-competent intervention for older adults is a program for caregivers of culturally diverse backgrounds (e.g., African American, Hispanic American, Asian American, and Native American/Alaska Native) who are caring for a relative with Alzheimer's disease or another form of dementing illness (Gallagher-Thompson et al., 2000a).
|
|
Fig. 32.2 Mrs S's diagram. |
Certainly there may be modifications or adaptations of treatment based on ethnic and cultural considerations, but specific changes leading to increased effectiveness have not been determined. Improved treatment for these individuals undoubtedly requires an understanding of the context of their lives, including historical events that have impacted them. Baker (1994) reminds the geriatric mental health field that within ethnicities, there is diversity and that it is important to seek specific information about life circumstances rather than make assumptions based on group stereotypes.
Preliminary research suggests that ethnic elders are much less likely than Caucasians to seek or participate in psychotherapy (Yeo and Hikoyeda, 1993). Despite limited knowledge, there is a great need for more information. One area that may affect mental health practice in need of further investigation is assessing and improving social supports, usually through extended family and organized religion communities. Though not typical terrain for psychotherapists, these areas are often important to ethnically and culturally diverse elders.
Epidemiological studies indicate that older individuals in need of psychiatric services are often underserved. In the UK and the USA, referral to and delivery of psychotherapeutic services to the elderly is low (George et al., 1988; Murphy, 2000). Older adults are less likely to seek mental health services than younger adults, and they typically present symptoms of emotional distress in their physicians’ office (Goldstrom et al., 1987). This may be due to a host of influences, including accessibility and reimbursement patterns. One opportunity and challenge to the field is how and where psychotherapeutic services can best be provided to this population. Innovative ways of improving the availability of mental health services for older adults, such as telehealth or telephonic use of therapies, mental health treatment in managed primary care (Gallo and Lebowitz, 1999), home and community-based interventions (Rabins et al., 2000), and the inclusion of psychotherapists on integrated teams (Zeiss and Gallagher-Thompson, 2003) are vast. Hopefully, the geriatric mental health intervention field will continue to flourish in their provision of services to older individuals, and will be joined by more colleagues in the future.
The older adult segment of the populations in industrialized countries is becoming larger and more diverse. This may translate to increased need for services for this age group. Psychotherapy, once thought fruitless for older adults, has been shown effective for an array of mental health disorders and problems in this population. The majority of therapists lack formal training in geropsychology and perceive themselves as needing additional training (Qualls et al., 2002). Although there are many commonalities in working with younger and older adults, there are also certain distinctive factors about older individuals that affect prevalence of mental health conditions, risk factors, assessment, and treatment. Psychotherapists who are interested in working with older individuals should familiarize themselves with the myths and actualities of aging, including understanding maturational and cohort differences, understand which therapies are empirically supported, and become familiar with and attentive to the potential modifications of assessment and treatment.