The diagnostic category of avoidant personality disorder (AvPD) is among those Axis II disorders classified informally as the ‘anxious and fearful’ subgroup (DSM-IV; American Psychiatric Association, 1994, see Box 26.1 for standardized criteria), and is one of the more prevalent forms of personality pathology (Ekselius et al., 2001; Alden et al., 2002). Patients who meet criteria for this chronic condition typically demonstrate the following characteristics: (1) high vulnerability to feelings of overstimulation; (2) low tolerance for physical and emotional discomfort; (3) great sensitivity to being interpersonally judged, criticized, or rejected; and (4) a propensity for engaging in avoidance behaviors as a chief default strategy when under subjective duress. By extension, persons with AvPD have underdeveloped or underutilized coping skills, as well as a relatively limited scope of life experiences borne of neglected tasks, self-handicapping strategies, and multiple missed opportunities.
A pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, beginning in early adulthood and present in a variety of contexts, as indicated by four (or more) of the following:
avoids occupational activities that involve significant interpersonal contact, because of fears of criticism, disapproval, or rejection;
is unwilling to get involved with people unless certain of being liked;
shows restraint within intimate relationships because of the fear of being shamed or ridiculed;
is preoccupied with being criticized or rejected in social situations;
is inhibited in new interpersonal situations because of feelings of inadequacy;
views self as socially inept, personally unappealing, or inferior to others;
is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing.
Avoidance is an important strategy that has survival value for humans (see Gilbert, 2002). When real dangers are recognized and sidestepped, people reduce their vulnerability to harm, and extend their lives. However, if engaged in excessively, avoidance can limit people's lives in insidious ways. The result is their feeling vaguely dissatisfied, low in self-efficacy, anxious and perhaps dysphoric in benign situations, and having a heightened sense that life is passing them by. To expound, when avoidance is a person's main ‘coping’ strategy over many years and across many situations, it can produce the following consequences (see Newman, 1999), in which AvPD patients:
Focus excessively on possible risks, and insufficiently on probable rewards. They play it too safe in life, limit their range of experiences, and reduce their amount of trial-and-error learning that would otherwise produce important knowledge and skills with which to navigate life.
Do not allow themselves to habituate to feared but otherwise safe situations, thus remaining intimidated by situations over which they could develop a sense of mastery if they were to give themselves the chance.
Miss opportunities to surprise themselves with unexpected successes such as the acceptance of respected others, and accomplishing challenging tasks that have the potential to improve self-esteem and socioeconomic standing.
Unwittingly deny themselves the kinds of peak experiences that stem from striving, persevering through difficulties and discomfort, overcoming adversity, and ultimately succeeding.
Become regretful, self-reproachful, and even embittered as they see their lives become consumed with strategies for self-protection at the expense of those for the pursuit of fulfillment and self-actualization.
Sadly earn the disapproval and disappointment of important others who they have let down due to their avoidance. For example, when a person fails to attend her best friend's opening of her art exhibit owing to ‘discomfort with crowds of unfamiliar people,’ the avoidant person erodes that friendship by putting her need for self-protection ahead of her ethic of ‘being there’ to support her friend. Ironically, this brings about the very sort of interpersonal criticism and exclusion the avoidant person fears in the first place—the classic self-fulfilling prophecy.
There has been some discussion as to whether AvPD is a separate disorder from the Axis I generalized social phobia (GSP), or simply a more pronounced or extended version of it (Heimberg, 1996; Reich, 2000; Tillfors et al., 2001). Indeed, the high rates of comorbidity between AvPD and GSP are well documented (e.g., Brown et al., 1995; Tran and Chambless, 1995; Feske et al., 1996; Rettew, 2000), and even more pronounced due to the DSM-IV's de-emphasis of nonsocial factors in the criteria for AvPD. In order to restore a useful distinction between the diagnostic categories of AvPD and GSP, Arntz (1999) suggests a reinstatement of the older conceptualization of AvPD, including such factors as intolerance of strong emotions. Indeed, in this chapter we endeavor to portray AvPD as something more than interpersonal shyness, but rather a more extensive problem of shying away from important subjective experiences (e.g., strong emotions, critical decisions), and opportunities for personal growth.
As with many Axis II disorders, AvPD often coexists with other personality disorders (Alden et al., 2002). In particular, there is a highly significant overlap with dependent personality disorder (DPD), with one study finding 43% of AvPD sufferers also meeting criteria for DPD, and 59% of DPD individuals coming up positive for AvPD (Stuart et al., 1998). There is also evidence that some individuals with AvPD abuse alcohol and other drugs in order to ‘self-medicate’ their anxiety (Stravynski et al., 1986). In addition to the problem of addiction per se, this maladaptive strategy decreases social effectiveness, thus feeding into a vicious cycle that worsens the person's low self-confidence.
Although this section presents an overview of the major psychosocial models for AvPD, it should be acknowledged that there is ample evidence for a genetic component related to the extreme shyness, reserved temperament, and overreactivity to novel stimuli often associated with AvPD (Widiger, 2001). At the same time, the ‘nurture’ part of the nature–nurture interaction provides us with potentially useful ways in which to understand the development and maintenance of AvPD, as described below.
Variations of a conceptual framework within which to understand AvPD have come from writers from a psychodynamic tradition. For example, the marked discomfort and ambivalence that individuals with AvPD experience in navigating close relationships is well captured by the term anxious attachment (Bowlby, 1973). The person who is prone to anxious attachments wants to have meaningful interpersonal ties, but simultaneously feels extremely vulnerable to the potential punishment and neglect of important others. Two subtypes of this categorization are the anxious-avoidant person and the anxious-ambivalent person. Those who are anxious-avoidant seem to correspond to those AvPD patients who demonstrate a pervasive avoidance of situations that stir up significant affect, including relationships and life tasks that require a personal investment. Those AvPD patients who seem to fit the anxious-ambivalent subtype are more likely to be those with comorbid DPD. Such individuals tend to cling to one or more significant others, all the while fearing getting too close lest they be discovered to be unlovable, leading to potential rejection and abandonment.
From a general psychodynamic perspective, persons who demonstrate AvPD are theorized to have had upbringings with primary caregivers who were inconsistent at best, and perhaps absent and/or abusive. Recipients of such treatment at early stages of development do not learn to feel at ease in ‘being themselves,’ as they believe that their natural behaviors will likely elicit rebuke, withdrawal of love, or other harmful shaming responses. In adulthood, many AvPD persons will be frustrated and self-reproachful as they come to realize that they are too frightened to seek and maintain the sort of relaxed, mutually accepting relationships for which they long. Even if they are fortunate enough to find a caring, accepting, mature partner, the individual with AvPD remains insecure, and the quality of the relationship may suffer.
More recently, Gabbard (2000) has similarly described maladaptive avoidance behavior as a defense mechanism against embarrassment, humiliation, rejection, and failure. Individuals who evince this clinical problem are believed to harbor a great deal of shame, evolving from early developmental interactions. For example, adults with AvPD retrospectively reported perceiving a discouraging home climate, and receiving fewer demonstrations of love and parental pride than their control group counterparts (Arbel and Stravynski, 1991). In a similar vein, Meyer and Carver (2000) reported that their college student sample of avoidant subjects reported a significantly greater incidence of childhood rejection and isolation than control subjects, even when taking current mood level into account as a covariate.
The Core Conflictual Relationship Theme (CCRT) is a defining feature of Luborsky's (1984) supportive-expressive therapy (SE). In this psychodynamic model, AvPD patients tend to have harsh superegos and subsequently project their own unrealistic expectations of themselves on to others. As a result, the AvPD patients wish to be close to others, but view them (and expect them) to be rejecting, and so they withdraw from the start so as to pre-empt the interpersonal harm they anticipate.
Another variation on this conceptualization comes from Benjamin's (1993) Structural Analysis of Social Behavior model (SASB). In her formulation, individuals who later develop AvPD are subject in childhood to relentless control directed toward creating a favorable social image. When such children reveal or demonstrate flaws and mistakes, they are responded to with shunning, humiliation, exclusion, and banishment. This results in the AvPD sufferers’ choosing to remain alone rather than take further risks in interacting with others who are expected to judge and reject them. As they go through life, these individuals face an ongoing conflict between their wish for social contact and their extreme sensitivity to humiliation. Thus, they will try to minimize outward signs of disagreement with others, instead ‘swallowing’ their opinions and feelings. However, the resultant inauthenticity of their interpersonal encounters eventually bring about the very criticisms they fear so much. A mutual cycle of interpersonal blaming and ignoring is created, resulting (in the more severe instances) in paranoid fears of those outside the family (if not inside the family as well).
Millon's model (e.g., Millon and Martinez, 1995) similarly describes dysfunctionally avoidant persons as wanting social acceptance, but being very sensitive to perceived and anticipated social humiliation. They restrain themselves in social interactions, initially thinking that by being inconspicuous they will remain safe. However, as their desires for closeness remain unfulfilled, they no longer feel safe as much as ignored, rejected, and ostracized. Their moods are often characterized by tension, sadness, and a quiet anger (behind the facade of a smile), and they over-rely on ‘numbing’ and fantasy as defense mechanisms.
An overarching formulation that describes the phenomenon of anxiety disorders in general from a cognitive therapy standpoint is the risk-resources model (A. T. Beck et al., 1985). In this framework, individuals who tend to shy away from important tasks and relationships in life are prone to magnify the risks of a given situation they must face, while concomitantly minimizing their sense of coping resources. For example, a man with AvPD who makes a date with a female neighbor and then fails to show up may have feared that the woman would find him boring and then would tell all her friends. At the same time, he may have ignored the fact that he had already made her laugh in conversation on many occasions, and that he had a number of interesting ideas about how they could spend their time together. Unfortunately, his cognitive exaggeration of the possible pitfalls and his overlooking of his strengths led to his standing up his date—the worst outcome he could have produced in terms of fostering an unfavorable public impression.
The problematic behaviors and emotions of individuals with AvPD are well described in the DSM-IV (APA, 1994). However, the belief systems of such persons are informative as well (see A T. Beck et al., 1990, 2001). Typical beliefs held by AvPD patients include:
‘I cannot tolerate unpleasant feelings.’
‘If people get close to me, they will discover the ‘real’ me and reject me.’
‘It is better not to do anything than to try something that might fail.’
‘If I ignore a problem, it will go away.’
‘I am socially inept and undesirable in work or social situations.’
‘If I keep my expectations low, I can never be disappointed.’
‘Keeping things to myself is good, but talking things out can only lead to trouble.’
Related to the above, Young (1999) has postulated a series of early maladaptive schemas (henceforth to be referred to generically as schemas) that are related to the development of rigid, chronic mindsets (and concomitant behavioral sets and emotional patterns) that plague persons with personality disorders. Schemas that are most pertinent to those with AvPD would be incompetence, unlovability, social undesirability, vulnerability to harm, and (to a lesser degree perhaps) lack of individuation. The above beliefs and related schemas serve to perpetuate the AvPD sufferer's interpretation of the environment as demanding, hazardous, critical, and rejecting, and their own responses as inadequate and potentially shameful. Thus, their chief mode of ‘coping’ is to steer clear of as many situations as possible that they do not find familiar or comfortable, a strategy that negatively reinforces them by reducing their anxiety and bringing temporary relief. Unfortunately, such persons experience a long-term sense of low self-efficacy that has little chance of being modified naturally, as the individuals with AvPD continue to sidestep life situations that would potentially teach them valuable skills for managing the world of relationships and tasks (love and work). The consequences of this pattern for AvPD patients include a life that is lacking in richness, a mode of operation that is needlessly self-limiting, and a lack of emotionally meaningful relationships.
An additional way to conceptualize the dysfunctional cognitive processing of individuals with AvPD has been described by Newman (1999), who hypothesizes that such persons habitually overestimate and magnify the expected consequences of making errors of commission, while grossly minimizing or overlooking altogether the potential hazards of making errors of omission. This process is consistent with the AvPD person's typical belief that it is better not to do anything at all than to try something that might fail; ‘The AvPD's credo is the antithesis of the wise saying, “Nothing ventured, nothing gained”’ (Newman, 1999, p. 60). In a certain sense, this strategy is understandable. Errors of commission can be quite conspicuous, potentially leading to great embarrassment, whereas errors of omission are hidden; it is more difficult to detect the negative consequences of not having done something. Indeed, it is the rare patient with AvPD who presents for therapy complaining of ‘avoiding too many things as a way of life.’ More often, they enter treatment in an effort to reduce their symptoms of anxiety (i.e., their avoidance isn't solving their anxiety problem) and/or to address their vague sense of ennui and dissatisfaction with life. These patients begin to notice that they are ‘missing out on something’ compared with the people around them who seem to have fuller, richer, more active lives. They also sense that they lack the skills to achieve a more satisfying life, a belief that may in part represent a characteristic cognitive magnification of the negative, but may also be based in fact. Given that pervasive avoidance breeds ineffectiveness through sheer lack of trial-and-error practice, many persons with AvPD cannot suddenly increase their involvement in a range of life activities without committing a slew of mistakes—the very outcome they feared most of all from the very start. This can lead to a sense of being trapped, in that the patients feel unfulfilled if they do not change, but profoundly fearful if they do try to change.
On a broader scale, the pace of modern life in Western societies is extremely rapid. Change is ubiquitous and considered synonymous with progress. People are urged to ‘keep up with the times’ and ‘be the first on the block…’ Unfortunately, people with AvPD do not take kindly to change, as change threatens to make their well-worn strategies for maintaining safety, security, and familiarity obsolete. Thus the personal style of individuals with AvPD is in conflict with the environment. Therapists have to help their AvPD patients improve their confidence and abilities in being proactive, decisive, prompt, and future oriented, all the while tolerating the anxiety that is triggered along the way. The hope is that—all things considered—the patients will achieve more of a sense of accomplishment, contentment, and even excitement in life per unit of anxiety!
In evaluating the effectiveness or efficacy of treatments for AvPD, multiple outcome criteria can be used such as: (1) degree of social interaction; (2) levels of anxiety and dysphoria; (3) changes (improvements) in beliefs specific to AvPD; and (4) degree of AvPD symptomatology as per the DSM-IV. Given the overlap between AvPD and GSP, it makes sense to measure patient progress in terms of their social skills and related cognitions and emotions. For example, short-term social skills training combined with cognitive interventions have been found to be effective in increasing the frequency of sociable behavior and decreasing social anxiety in patients with AvPD (Stravynski et al., 1982). Additional behavioral treatments (in both individual and group modalities) that particularly focus on the AvPD patients’ social anxieties and interactional difficulties have had some success as well (Alden, 1989; Stravynski et al., 1989; Renneberg et al., 1990). Interestingly, Stravynski et al. (1994) found that the addition of four in-vivo sessions did not enhance the outcome of an otherwise successful course of social skills training; in fact, these additional sessions were associated with a high drop-out rate.
Although the results of studies on social skills approaches (individual and group) to AvPD seem positive, the statistically significant improvements indicated by many of these studies do not necessarily translate into optimally significant clinical improvements (Alden et al., 2002). Thus, many AvPD patients made gains in treatments such as those above, but not necessarily to the point of experiencing a remission of their AvPD, or being indistinguishable from ‘normals’ (Alden, 1989; Renneberg et al., 1990).
A similar result can be found in the psychodynamic treatment research literature. Barber et al. (1997) found that of those patients who completed their year-long treatment of SE dynamic psychotherapy, 39% still retained their AvPD diagnosis at the end of the program. Nevertheless, the patients (as a group) demonstrated improvements on measures of depression, anxiety, general functioning, and interpersonal problems. This study was a part of a larger project at the University of Pennsylvania that also tested the efficacy of cognitive therapy with AvPD patients, as well as the efficacy of SE and cognitive therapy for obsessive-compulsive personality disorder (OCPD). Although the outcome data from the cognitive therapy modality are unpublished, the preliminary results were promising enough that the authors of the SE treatment study above were intrigued about the question of ‘Which treatment suits which sort of patient best?’ Thus, Barber and Muenz (1996) retrospectively examined the data from the Treatment for Depression Collaborative Research Program (TDCRP: Shea et al., 1990). The authors found that the manualized form of interpersonal psychotherapy yielded more symptomatic improvement when depressed patients were more obsessive and less avoidant, while cognitive therapy was more effective with increased levels of avoidance and decreased levels of obsessiveness. The authors hypothesize that cognitive therapists may make relatively more demands of AvPD patients to be active in the session, and between sessions (e.g., therapy homework), and that this translates in some instances into more extensive therapeutic changes with this population.
In response to the above work, Strauss (2001) examined the cognitive therapy audiotapes and data set from the aforementioned University of Pennsylvania studies on the treatment of AvPD and OCPD. She hypothesized that a uniformly smooth therapeutic alliance may not be the best predictor of favorable outcome, in that the therapy would be ‘too easy,’ with less of the changes one would expect from a therapeutic experience involving more of a struggle. Indeed, the results indicate a curvilinear relationship between variability in the therapeutic alliance and outcome, suggesting an optimal range of ‘stress’ between therapist and patient as being most facilitative of change. One may hypothesize that an active, directive, collaborative approach such as cognitive therapy would be most apt to induce this sort of strain in the therapeutic alliance, especially with AvPD patients who are ambivalent about change and the discomfort of actively engaging in the process.
As an illustration of the above, a single case study of cognitive-behavioral therapy for AvPD was published by Coon (1994), who found a marked decrease in Beck Depression Inventory scores from initial session to 3-month follow-up as well as modification of schemas and four of the AvPD criteria met at intake. Treatment had initially focused on goal setting, decision making, problem solving, and identification of automatic thoughts. Later (in sessions 12–22), closer attention was paid to the patient's maladaptive schemas. However, the course of treatment had its hurdles and speedbumps, with the patient missing and canceling some of the early sessions, and having some difficulties with homework and role-playing. The therapist was nonjudgmental, but stayed the course, and helped the patient address his problems in treatment within a cognitive case formulation. The patient became more engaged in treatment, and positive changes accrued and were maintained.
It is important to look at the interpatient differences within the diagnostic territory covered by the designation of AvPD, as such differences may account for why some of these patients improve more than others. For example, Alden and Capreol (1993) found that the AvPD subjects demonstrated differences in their interpersonal problems and that these differences influenced their response to treatments. Specifically, ‘cold-avoidant’ patients who had interpersonal problems related to distrustful behavior (implying a strong ‘mistrust’ schema) benefited from gradual exposure but not from skills training. By contrast, the ‘exploitable-avoidant’ patients who experienced problems being coerced and controlled by others (implying strong ‘vulnerability to harm’ and ‘lack of individuation’ schemas) benefited from both graduated exposure and skills training, particularly training focused on the development of intimate relationships.
The data seem to indicate that retention of patients with personality disorders in general (and AvPD in particular) for a complete course of treatment is difficult, yet quite important for success. For example, Greenberg and Stravynski (1985) found a link between avoidant patients’ fear of ridicule and premature termination. The authors suggest that cognitive interventions should especially target this area of avoidant patients’ concern in order to increase the effectiveness of treatment. In a study by Persons et al. (1988), more than half of the 70 patients met diagnostic criteria for a personality disorder, and—as a whole—these patients were significantly more likely to drop out of treatment early than their counterparts who did not have an Axis II diagnosis. However, those patients with concomitant personality disorders who succeeded in staying in treatment until completion showed substantial improvements that were statistically equivalent to the patients who did not have personality disorders. Similarly, Sanderson et al. (1994) found that those among their sample of patients with generalized anxiety disorder who also had personality disorders tended to leave therapy early. However, those who completed at least a reasonable short-term course of cognitive therapy showed a significant decrease in both anxiety and depressive symptoms. This phenomenon of early drop-out from therapy was dramatically demonstrated in the Barber et al. (1997) study, in which only 13 of the original 24 patients being treated for AvPD remained for the entire course of treatment (a year of weekly sessions). It makes sense that persons with avoidant habits who also fear change will have difficulties in staying in treatment. Being able to cope with the demands of therapy may be one of the most important exposures that the AvPD patient can experience on the road to recovery. Later, we will suggest some methods for engaging these patients in the process of treatment.
The SE approach to AvPD puts great emphasis on giving the patients empathy for their humiliation, embarrassment, and shame surrounding interpersonal situations, and on pointing out how anxieties occurring in the transference with the therapist may provide useful information about similar anxieties in other relationships (Gabbard, 2000). Therapists help their patients explore important etiological and developmental factors pertinent to their expectations for failure, rejection, and loss of nurturance. While some focus is placed on the patient's actual past interactions with primary caregivers, additional attention is paid to the patient's unconscious impulses and fears that have led to avoidant behavior. For example, a patient may harbor an unacknowledged expectation that he will lose control in social situations, revealing primitive feelings that will lead to shame and rejection (e.g., expressing sexual interest in an inappropriate love object), and/or threat of retaliation and harm (e.g., expressing heretofore hidden anger toward a parental figure, such as an employer, mentor, or therapist).
The SE model utilizes a central concept—the Core Conflictual Relationship Theme (CCRT)—to shed light on the patients’ interpersonal style over the course of their development and life (Luborsky, 1984). The AvPD patients’ penchant for wanting but fearing the seemingly risky process of getting emotionally close with others is expected to manifest itself in the therapeutic relationship. For example, the patients may respond quietly or with superficial responses (e.g., a giggle) following a heartfelt demonstration of support from the therapist, or may avoid a session out of fear that their otherwise kindhearted therapist will be harshly critical. The therapist focuses the patients’ attention on these acts of avoidance in order to show them how their unconscious, automatic responses to relationship situations keep them distant and unengaged, even when the objective situation is relatively safe and secure.
Interestingly, psychodynamic approaches dovetail with cognitive-behavioral methods in emphasizing the importance of patients’ gaining exposure to feared situations (Gabbard, 2000). This ‘exposure’ includes the in-vivo work involving the therapeutic relationship, where the AvPD patients may otherwise be hesitant to discuss highly emotional material, to discuss serious topics, to think about planning for the future and making personal changes, and to settle into a comfortable, open, trusting relationship with the therapist.
One of the distinguishing features of the SASB approach (Benjamin, 1993) is its emphasis on the complementary nature of social interactions, and the resultant exacerbations and polarizations in interpersonal behavior that may occur. For example, the therapist may try earnestly to encourage the AvPD person to talk about emotionally powerful material, or engage in everyday activities that involve manageable risks and potentially high rewards (e.g., going out to dinner with friends). The AvPD individual outwardly agrees with these prescriptive interventions, but then retreats and fails to follow through, owing to fears of being overwhelmed with out-of-control emotions, and of being the object of silent, social ostracism, respectively. The therapist then tries more assiduously to move the patient to make the therapeutic changes described above, which is secretly interpreted by the patient as a sign of reproach and excessive demands from the therapist. Again, the patient agrees politely in order to avoid conflict, but then does not discuss meaningful topics or follow through with the treatment plan. The therapist then becomes even more directive, and before long the two parties have unfortunately ‘danced’ into opposite corners where they have much less of a chance of working together. Once identified, this pattern becomes fodder for in-session discussion of the AvPD patient's typical socio-emotional interactions.
Extrapolating from the findings of Barber and Muenz (1996) and Strauss (2001) above, it may be necessary for the therapist to be moderately directive, and for AvPD patients to have the responsibility of being more goal oriented in order for the patients to move forward in therapy. If the treatment is too unstructured or exploratory without concomitant time limits, the patient's avoidant style may be given too much free reign to play itself out, session after session, thus bogging down the process of change and leading to the loss of much valuable time. It may be necessary for therapists to be more active and confrontive of the patients’ avoidance (see Davanloo, 1999). The following, fictitious sample dialog serves as a brief illustration:
Therapist: What was your experience when your husband told you that he ‘didn't want to hear another word’ about your work stress, and that you should just ‘shut up and give it a rest?’
Patient: Well, that's just my husband, you know. He doesn't like to be distracted from his reading in the evening.
Therapist: That's all well and good for him, but I asked you what your experience was when he made those comments to you.
Patient: He really has had to put up with my complaining about work for a long time, and he doesn't want to talk about it anymore, because he says I never do anything about it anyway.
Therapist: Do you notice that I asked you twice about your experience, but both of your answers focused squarely on your husband? I am interested in hearing about you.
Patient: (Nervously laughing) Well, you've had to hear my complaints about work too! I'll bet you're as sick of the topic as my husband is!
Therapist: So now we're talking about me? (pauses and then speaks quietly, with a friendly smile) You seem to be the missing person in all of this. It's as if you don't count. But you do count. Yet you're finding it very difficult to talk about your feelings. I have some thoughts about what you must be going through, especially because you just laughed in a tense way when you said that I must be as sick of your complaints as your husband is. I heard that. We need to talk about that. What is this whole line of questioning like for you? Can you tell me what you're going through, right now? I'm listening.
In some respects, the cognitive-behavioral treatment of AvPD looks very similar to the cognitive-behavioral treatment of GSP, a situation that reflects the conceptual and diagnostic overlap that has been found to exist between these two diagnostic entities (Alden et al., 2002; Reich, 2000). Targets for intervention typically include the patients’ inhibited social performance, their aversion to growth-related discomfort, their tendency to engage in marked procrastination, and their expectations for interpersonal censure and rejection, to name a few. Additionally, cognitive-behavioral therapists will assess, highlight, and try to facilitate the modification of the AvPD patients’ specific beliefs and related schemas that maladaptively shape their perceptions of themselves and their interactions with others. For example, much attention will be paid to the patients’ schemas of incompetence, social defectiveness, and vulnerability to harm (see Young, 1999), as well as such harmful beliefs as, ‘If I don't think about a problem it will go away,’ and ‘If I never try then I can never fail’ (cf. A. T. Beck et al., 2001). Interestingly, cognitive therapy also focuses on the patients’ avoided emotions (Newman, 1991), and thus bears some similarity to alternative models such as focused-expressive psychotherapy (Daldrup et al., 1988). Imagery techniques are commonly used to heighten affect in the hope that ‘hot cognitions’ (see Greenberg and Safran, 1984) will be accessed that are most relevant to the patient's problems—emotion-laden thoughts that the patients usually do not notice, acknowledge, or reveal easily.
A cognitive conceptualization of a typical AvPD case often reveals that the patients demonstrate strong approach-avoidance conflicts about closeness with other people, leading to high anxiety, shying away, loneliness, and reduced opportunities to learn social skills. They have a low sense of self-efficacy—reinforced in part by their lack of practice in volunteering for challenging tasks and interpersonal engagement—along with a strong belief that others will punish them for their failures. They compensate for these problems by reducing stimulation and risk (as they see it) as much as possible. They minimize their exposure to social situations, academic/ vocational tasks, interesting and novel life experiences, and even their own most important thoughts, emotions, and memories. In short, these patients fail to show up for their own lives (Newman, 1999), and become very dissatisfied with the relatively empty results.
A combination of these methods is a central aspect of cognitive-behavioral intervention. Talking about the patient's difficulties is part of the process (e.g., in order to help patients address important issues), but is not considered to be a viable substitute for between-sessions interacting with others, and actively managing important but difficult tasks in everyday life. Thus, homework is an essential part of treatment. For example, therapists and AvPD patients can work to identify and document some of the latter's most salient examples of avoidance at home (e.g., procrastinating in writing a paper for school, in paying bills, or in washing the dishes), work (e.g., not answering e-mail memos from a supervisor, or declining a promotion with higher pay but more responsibilities), and personal relationships (e.g., not showing up for a relative's birthday party, or being ‘too embarrassed’ to say genuinely endearing things to a friend when the situation begged for it). Being able to face these situations and respond proactively is a vital part of the process of ‘recovery’ from AvPD.
At the same time, AvPD patients are hypothesized to be handicapped by negative beliefs and schemas that make it difficult for them to incorporate new information of the sort that they would gain by engaging in the situations described above. Thus, even if they succeed in dealing actively with situations they would ordinarily avoid, individuals with AvPD may have cognitive responses that will not likely reinforce their apparent therapeutic successes. For example, they may decide that they were ‘lucky’ this time, but that they should not push their luck by trying again, that the other people were ‘just pretending to be nice,’ or that the situation was so stressful that it ‘isn't worth trying to do anymore.’ These sorts of cognitions need to be identified and modified in order for the AvPD patients’ gains to be something more than short-lived aberrations. Thus, even when the patients complete their homework (or otherwise report therapeutic changes between sessions), therapists must ask them what they think of their new behaviors, and how much they believe they are benefiting from such changes. The goal is to help the AvPD patients ‘own’ the changes, to continue to engage in these new behaviors so that they learn them better, and to learn to focus on the psychological gains of such changes, rather than the concomitant anxiety.
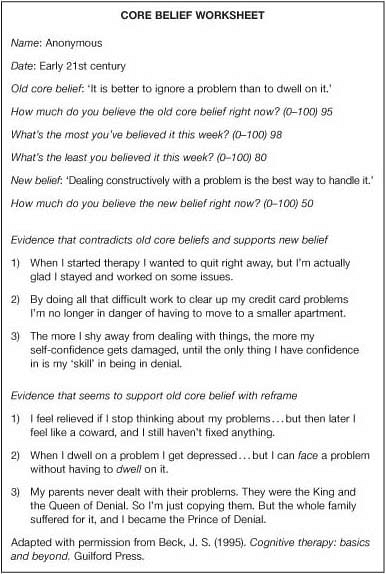
Standard techniques such as thought-monitoring and rational responding via Dysfunctional Thought Records (DTRs: J. S. Beck, 1995) can be used to address the AvPD patients’ magnified fears about errors of commission, anticipated consequences of trying to learn new things, social rejection, and the like. Similarly, DTRs and related written methods such as the Core Belief Worksheet (J. S. Beck, 1995) can be used to evaluate the patients’ AvPD-related beliefs and schemas directly. In Figure 26.1, a patient uses the Core Belief Worksheet to re-examine his belief that ‘It is better to ignore a problem than to dwell on it.’
|
|
Fig. 26.1 Cognitive-behavioral model. |
In order to manage the anxiety that accompanies therapeutic changes, cognitive-behavioral therapists assist their patients in structuring tasks that are graded from easiest to most challenging. In other words, patients learn that therapy generally does not involve dramatic ‘breakthroughs’ as much as gradual improvements. Behavioral changes and cognitive changes reinforce each other in a virtuous cycle, and the patient's emotional and interpersonal life improves in the process.
One of the overarching strategies of the cognitive-behavioral therapist is to help individuals with AvPD improve on their areas of weakness and deficit. Owing to their customary low-key behavior, aversion to change, and magnification of risk, AvPD patients often have difficulties with setting and striving toward goals, being decisive, and taking the necessary steps to grow and advance in life. Thus, therapists typically emphasize the importance of AvPD patients learning how to specify personal goals for treatment, identifying the graded steps that are required to achieve them, weighing the pros and cons for various ways of approaching these steps, cognitively and behaviorally rehearsing the enactment of these steps, and making cognitive changes so that inhibitions that might otherwise interfere with goal attainment would be minimized.
At times, cognitive-behavioral therapists (as their psychodynamic counterparts) will examine the therapeutic alliance in the immediacy of the session. Among the goals are: (1) to access ‘hot cognitions;’ (2) to address the patients’ sense of safety, trust, and confidence in interacting with the therapist; and (3) to highlight the process of patients’ communication. For example, a patient may laugh nervously when he acknowledges that he did not follow through on his assignment. Below is a sample dialog that may follow:
Therapist: You're laughing, but I wonder what you're thinking right now.
Patient: (Keeps chuckling, but in a muted way, and looks away).
Therapist: Seriously, what are you thinking right now?
Patient: I'm kind of hopeless (keeps smiling).
Therapist: Not a pleasant thought. Not the thought I would have about you. I don't think that a homework assignment determines whether someone is hopeless or not… but do you? Tell me more about your thoughts about yourself.
Patient: (Long pause). This feels a little bit silly. I'm sorry I didn't do the homework. I'll try next time. What's the next agenda item (laughs)?
Therapist: This is really uncomfortable for you. You're practically leaving skid marks trying to get away from this topic… or these topics. This is not just about homework, which is important, but doesn't determine a person's worth. But this is also about how you view yourself when you have difficulties, and how you expect others—in this case, me—to view you. It's also about what to do when you feel uncomfortable. Do you get to the bottom of the discomfort and try to solve it, or do you try to get away as fast as you can? This isn't silly at all. It's real central stuff for your therapy. Can we talk about this further?
Patient: (Looking downcast). You're not going to let me get away with this, are you?
Therapist: Does it feel like a punishment, or like a criticism?
Patient: I just didn't do the homework. Can we go on to the next subject?
Therapist: (Takes some time to think). What's happening right now is so important I hope we can discuss it. I really want to know how you're feeling and what you're thinking. Even more so, I hope you can learn more about what you're thinking and feeling. This is not just about homework. It's about feeling badly about yourself, and expecting that others think badly about you to, and then not wanting to think about it at all. If we can talk about this, I think you can get something useful out of the discussion. I'm willing to try and see. How about you?
Another important technique is role-playing, most often involving social situations requiring assertiveness, congeniality, or general conversational skills. Patients with AvPD often need considerable practice in acquiring or reinforcing such skills, and the therapist's office provides a unique opportunity to rehearse these behaviors without the threat of social faux pas. Unfortunately, AvPD patients often fear making mistakes in front of their therapists, and may even be sufficiently ashamed that they do not want to do role-plays even if nobody but themselves is around to judge. Thus, AvPD patients frequently decline to take part in role-playing, which becomes a therapeutic issue. After all, the therapy setting (arguably) is a less threatening venue than real-life situations. Thus, if the patients cannot bring themselves to engage in behavioral rehearsal exercises in session, it is unlikely that they will do so in everyday life where it is most important. Therapists cannot force their patients to take part in role-plays, but they can address the latter's fears of failure, and continue to encourage them to try the role-plays a little at a time.
Similar to more experiential psychotherapies (e.g., Daldrup et al., 1988), cognitive-behavioral therapists also recognize that persons with AvPD often demonstrate a restricted range of emotions—frequently being superficially humorous, bland, or quietly anxious (and perhaps resentful as well). In other words, the patients are avoiding their emotions as well, and would benefit from expressing them more openly, directly, and constructively in order to increase the immediacy of their interpersonal relationships as well as giving them access to greater degrees of joy and enthusiasm. In order to increase the patients’ access to a broader range of meaningful emotions, cognitive-behavioral therapists sometimes employ evocative imagery exercises (Newman, 1991).
For example, a woman who presented with panic attacks and an avoidant personality style admitted that she had never properly grieved for her mother, and that she had tried ‘not to think about’ her guilt about how poorly she had treated her mother in her final months of life. The imagery intervention that dealt with this involved a relaxation exercise followed by the therapist guiding the patient through an imaginal trip back to her mother's hospice so she could tell her mother that she loved her and to say goodbye. During the exercise, the therapist asked the patient (whose eyes were closed) to imaginally communicate with her mother in a way that would counteract her views of herself as a ‘bad daughter.’ In the image, the patient was uncharacteristically emotionally demonstrative with her mother, took responsibility for having been absent during her illness, promised to treat her own kids as well as her mother had treated her, and to honor her memory in a loving way, but not with too much guilt. Postintervention debriefing suggested that the ‘ocean of emotion’ (as the patient described it) helped her to ‘really believe’ her own promises to her mother in the image. The patient reported a high degree of motivation to improve her life, and to ‘be there’ for others. Most important, in the coming months, this patient reported that she was not allowing her fear of panic attacks and social interactions to stop her from spending time with friends and family.
Group models of psychotherapy (e.g., Yalom, 1980, 1995) tend to focus more on the process of treatment in the here-and-now of the group session than on the individual etiologies of the group participants. Depending on the theoretical orientation and training of the group leader, the explanations for each group members’ AvPD characteristics may focus on such factors as early-life rejection, humiliation, and shaming, schemas of incompetence and social undesirability, magnified sense of risk coupled with minimal confidence in personal resources, and the negative reinforcing value (and life inhibiting results) of avoidance. However, the purpose and function of group therapy is to use the group dynamic to test participants’ expectations for negative judgment and rejection, to connect with others in a meaningful way, and to learn interactional skills that can improve interpersonal performance in everyday life. In the meantime, group members learn to tolerate the experience and expression of affect, both within themselves and in front of others.
The group therapy model arguably treats the phenomenon of AvPD as synonymous with GSP. Many groups define themselves as ‘social anxiety’ groups, but few ever self-label as treating AvPD (for an exception, see Renneberg et al., 1990). In a group therapy model, treatment works because the opportunity for the patients to escape easily from interpersonal situations as soon as they feel anxious is greatly minimized (unless they precipitously drop out of treatment, which is a hazard in treating AvPD across all modalities, as we will touch upon below).
Group therapists (e.g., Yalom, 1995) note that as AvPD patients are fearful of socially demanding situations, they will be difficult to engage in group therapy. More specifically, they may profess to want to join such a group, but may be apt to change their minds and not show up, or drop out quickly. However, their typical problems in interacting can come to the fore quite readily in a group setting, such as when the individual thinks that everyone else in the group (including the therapist) uniformly thinks critically of them. Yalom points out that such patients fail to see others as individuals, each of whom has different preferences, opinions, and styles. Instead, the AvPD patients project their self-denigrating feelings on to all the other group members as if they were a single-minded, critical mob. One of the goals of treatment is to highlight, discredit, and change this projected ‘group-think’ in favor of actual interactions and authentic communication with others, each one at a time.
One of the unique challenges for the group therapy leader is to resist the temptation to ‘fill in the spaces.’ In other words, a group of AvPD patients may tend (collectively) to be reticent, passive, and loath to stir up an emotional or otherwise stimulating discussion. Group leaders—especially those who have been trained in a cognitive-behavioral model where being directive is often an asset—may slip into ‘didactic mode’ at such times, thus depriving the group of its potential to become a dynamic, interactive force among themselves. Although some groups are deliberately structured as psychoeducational in nature, this may not be the optimal approach with AvPD group members who often are all too relieved to sit back and let the therapist teach the class. On the other hand, as we have said, demanding too much role-playing and other forms of exposure to anxiety may precipitate flight from the group. Thus, finding the right balance is very important, and most likely involves building a graded-task methodology into the program.
For example, the lead author once ran an all-male GSP/AvPD group in which its participants first worked on identifying their anxiogenic thoughts in facing social and otherwise demanding situations. Next, the group members took turns practicing social interactions with each other. Finally, the group leader invited a series of female colleagues to come to successive group sessions to engage in role-play scenarios with the men, thus providing a bit of an ‘in-vivo’ flavor to the social demand. Though it was sometimes difficult to get each of the patients to take part in these role-plays, not one of the group participants dropped out. However, this positive result is not always the case, as noted below.
Not surprisingly, persons with avoidant personality characteristics will have an increased tendency to avoid therapy itself. While it is certainly true that engaging in therapy is usually a voluntary activity, and therapists should respect their patients’ autonomous choice to be in treatment or not, it is also important to be aware of the maladaptive aspects of AvPD patients’ propensity for dropping out of therapy in an untimely way. The following are questions to consider:
Does the patient often say, ‘I almost didn't come to today's session’ or otherwise express ambivalence about having shown up for the appointment?
Has the patient overtly voiced concerns about the direction of treatment, and/or his or her progress in therapy, or (by contrast) have these thoughts and feelings been kept secret from the therapist?
Did the patient cancel or fail to show up for an appointment directly following a therapy session that the therapist thought signified great progress?
Has the patient planned for termination and/or attended an official, final session, or has he or she simply failed to show up for an appointment, and failed to return follow-up calls and letter(s) from the therapist?
In general, therapists should not blithely assume that their AvPD patients will keep their next appointment, at least not while their avoidant characteristics are still markedly active. It is wise to consider the likelihood that such patients have one foot in and one foot out of therapy at any given time during the therapeutic venture. Thus, therapists should take special care to ask their AvPD patients for feedback—about how they feel at the end of each session, how therapy is progressing in their view and how it compares with what they expected, and whether they have any doubts or misgivings about continuing. Sometimes patients are not willing to voice their complaints or problems with therapy, and thus give their therapists the superficial response, ‘Everything is fine.’ Still, it is worth putting out feelers of this sort, thus giving the patients overt permission to address their mixed emotions about being in treatment.
Following a particularly arduous session with an AvPD patient—the sort that might cause sufficient discomfort to dissuade him or her from returning—therapists may choose to touch base with the patient via a short phone contact. The following is a sample voicemail message that a therapist can leave so as to support the continuation of the therapeutic relationship:
Therapist (phone message to patient): Hi Mr Q, this is Dr F I was thinking about our most recent meeting and how it was very stressful, but that you did some excellent work. I really look forward to continuing our discussion next Tuesday at 2:00 p.m. as we agreed. I just wanted to check in with you to let you know that I truly appreciate the effort you are making, and that I know it's going to pay off for you. Take care and I'll see you real soon.
Even when AvPD patients reliably show up for their therapy sessions, it may sometimes seem that they are not really attending to what is going on. They may appear distracted or disengaged, and have relatively little to say. Therapists notice that this phenomenon is occurring when they feel as if they have to ‘pull teeth’ to get the patients to contribute to the therapeutic agenda and dialog, or are met with the ubiquitous answer, ‘I don't know’ in response to their clinical queries. Therapists can become quite frustrated with patients who respond in this way, believing that their AvPD patients are painfully lacking in insight, or are engaging in deliberate stonewalling. The hazard in such situations is that the therapists’ behavior will go to one extreme or the other—either becoming too quiet and passive, allowing the sort of uncomfortable silences that the patient may interpret as rejection and punishment, or escalating the questioning to the point of sounding like an interrogator. Either way, the therapeutic alliance (such as it is) will likely be strained, thus offering ‘confirmation’ to the AvPD patients that they will be judged harshly if they allow themselves to be present in a conspicuous manner.
Therapists can respond to the above by being willing to say to their AvPD patients, ‘I can see that this sort of discussion is not something that comes easily or naturally for you, and you may believe there are some serious drawbacks to thinking and talking about important matters in your life; I can understand that.’ If empathy and a relaxed atmosphere in session are insufficient to inspire the AvPD patients to become more active, the therapist may try to offer a ‘multiple choice’ listing of potential topics or hypotheses to pursue. The goal is to jump-start a dialog in session, not to take sole control of the direction that therapy takes. Sometimes the patients will be responsive to such a soft sell approach, and will gradually warm to the task. However, if the AvPD patients remain excessively passive, therapists should not jump to the conclusion that therapy cannot proceed. Rather, therapists can model a comfortable reaction to silence, occasionally expressing interest in discussing any number of issues, and nicely inviting the patients to offer their ideas and feedback. If the patients often say, ‘I don't know,’ therapists can explain that they do not have to know for sure in order to offer some educated guesses, and that the patients’ life issues are important enough to merit some thought and consideration, even if at first the patients do not know what to say. In other words, ‘I don't know’ should not be the end of the story; rather, it should signal the beginning of an exploration.
One of the hypothesized active ingredients in cognitive therapy is homework (Persons et al., 1988). Thus, when patients habitually neglect to do their homework, they are likely inhibiting their potential progress in treatment, as well as their prospects for long-term maintenance of newly learned coping skills. Unfortunately, the notion of doing homework often triggers the AvPD patients’ fears of failure and censure. Thus, they opt to bypass the homework (an error of omission, whose consequences they characteristically minimize), rather than take the risk of exposing their incompetence by making mistakes on between-sessions assignments (an error of commission, whose consequences they typically magnify).
When AvPD patients avoid their homework, this needs to become a therapeutic issue, as much for an exploration of their incompetency schema as the potential implications for slowed and truncated therapeutic progress. Therapists can reassure their AvPD patients that even undone homework can be useful, as long the patients’ problems surrounding the homework are explored and discussed in an atmosphere of acceptance and hope for change. This is an argument for the continuation of the assignment of therapy homework, even when the AvPD patients rarely comply. As a caveat, therapists should temporarily back off from giving homework if the patients repeatedly fail to do it, openly state that they do not want to talk about it, and indicate (through various aspects of their demeanor) that there is a therapy-threatening rift in the therapeutic relationship.
Nevertheless, therapists can comment from time to time about the importance of patients learning to rely more upon themselves, and relatively less on the therapist. Homework is one way to facilitate this process, but therapists can also bolster their patients’ self-confidence by gradually turning over control of the agenda to the patient. Further, therapists can shift from an educational style (e.g., ‘Here is the method by which you can change’) to a consultative style (e.g., ‘Tell me how you would go about making a therapeutic change’).
Patients who meet criteria for AvPD often evince other personality disorders such as DPD, typically look similar to patients who present with GSP or other anxiety disorders, sometimes use alcohol and other psychoactive substances in order to ‘self-medicate’ and otherwise avoid their experiences, and are prone to drop out of treatment as a characteristic defense. Although there is strong evidence that an avoidance-prone temperament is inherited, it has also been found that persons with AvPD experience particular difficulties during their formative years that are associated with the development of ambivalence in getting close to others. Experiences of shaming, neglect, rejection, and harsh criticism (or the chronic perceptions of such) can lead AvPD individuals to pursue an inconspicuous existence as a way to stay out of trouble. Although this strategy may indeed prevent overt harm, its overuse prevents the formation of self-efficacy across a wide range of life tasks, including the establishment and maintenance of open, trusting relationships. As a result, such individuals are left in a chronic state of dissatisfaction, self-reproach, and anxiety as they realize that they lack the confidence and sense of security they believe is necessary to pursue their goals.
Therapeutic modalities such as cognitive-behavioral therapies, psychodynamic therapies, and group approaches have much in common in that they recognize the importance of exposure to feared situations. Therapists utilize role-plays, emotionally evocative exercises (e.g., imagery), in-vivo interpersonal experiences, homework, and processing of the patients’ hot cognitions and experiences in the therapeutic relationship in order to provide this exposure. It is also important to change the AvPD patients’ maladaptive beliefs and schemas that are otherwise maintained when they fail to test them actively in session, and in everyday life.
The therapeutic relationship with AvPD patients is also very important across modalities, in that the patients often expect to be criticized, scolded, and rejected, and will typically have approach-avoidance conflicts about bonding and sharing private information with the therapist. If the therapeutic relationship is ‘too easy,’ it is likely that the important work is not being done. If the therapist is too directive or confrontational, the patient may abandon treatment. Finding the middle ground, in which there is a strong alliance, but also some anxiety, tumult, and exposure to high affect may be the key.
Although there have been some promising results from a limited number of outcome studies on social skills training, cognitive therapy, and short-term psychodynamic psychotherapies, it has been difficult to achieve therapeutic changes that reliably make AvPD patients indistinguishable from ‘normals.’ Part of the problem is the high rate of drop-out found in the literature—when AvPD patients succeed in completing their treatments they tend to do as well as patients who did not present with personality disorders. Even those who still meet criteria for AvPD at termination frequently show clinically significant reductions in anxiety and dysphoria—meaningful changes in a population that often demonstrates comorbid anxiety and mood disorders at intake.
There are indications that cognitive therapy may be particularly well-suited to treat AvPD, though more tests of this approach need to be executed and published in order to evaluate the hypothesis. In the meantime, results from trials on GSP provide some clues about what is needed to maximize positive outcomes for people whose avoidance has become an unnecessarily limiting force in their lives.