What would it really take to save Narcissus, the legendary, dazzlingly beautiful, but misguided character of Greek mythology? As legend has it, the young Narcissus, scornful of all others but his own beautiful self, was the love object of the beautiful nymph, Echo. Though Echo's beauty was extraordinary, she received nary a glance from the self-obsessed young man, and this neglect caused her to brood to such an extent that nothing remained of her but her voice. For his heartlessness, Narcissus was duped into staring into his reflection in the pool of a fountain, an image that would dissipate upon too close encroachment; his conundrum, then, was that he could never possess his love object! Unwittingly obsessed with this bittersweet irony, Narcissus pined away, himself, until nothing was left of him but the flower that is his namesake. With only a ‘surface’ reflection of his outer beauty at his disposal, the young Narcissus could only be caught up in conflicting and confusing cognitions and feelings of euphoria and frustration, not unlike the personality pattern often encountered in contemporary therapy settings.
Narcissus may have easily benefited from some very basic interventions, such as a modicum of perceived ‘objectivity’ that would reaffirm his outer beauty, but this would not likely do him any long-term favors. Chances are that his next encounter with a reflection pool would bear close resemblance to the legend. Indeed, were simple comfort and restored confidence the ubiquitous goals of therapy with the narcissistic personality, these could often be achieved in but a few sessions. The therapist can hold initial interest by allowing the patient exclusive self-focus, and by further encouraging discussions of past achievements the therapist may enable the narcissist to rebuild any depleted self-esteem. Not infrequently, self-confidence in narcissists is restored by talking about themselves, by recalling and elaborating their attributes and competencies in front of a knowing and accepting person.
Merely reestablishing former levels of functioning, however, especially rebuilding the narcissist's illusions of superiority, may prove over the long run to be a disservice to the narcissistic patient. Until more realistic self-evaluation is achieved, it is not likely that narcissists will be motivated to develop competencies and socially cooperative attitudes and behaviors that would lead to more gratifying and adaptive lives. If the patient's capacity to confront their weaknesses and deficiencies is strengthened, patients may be able to acquire greater self-control, to become more sensitive and aware of reality, and learn to accept the constraints and responsibilities of shared social living. In the following review, we hope to elucidate a multifaceted, integrated approach to the treatment of this personality pattern.
The essential features of this personality style are an overvaluation of self-worth and a grandiose sense of self-importance and uniqueness. The irony, however, in this inflated self-concept is an inordinate need to be loved and admired by others; this would be a surprising necessity in a person whose elevated self-worth is entirely germane. Unlike the ravenous affectional needs of histrionic and dependent personalities, however, narcissists believe that they are entitled to tribute and praise by virtue of their ‘specialness.’ These personalities also share the antisocial features of egocentricity, interpersonal exploitation, and exaggerated needs for power and success. Unlike the anger and vindictiveness of antisocials, however, narcissists are frequently characterized by a benign arrogance and a sense that conventions and reciprocity of societal living is something that simply does not apply to a person of their stature. There is little real empathy for others but rather, a tendency to use people for self-enhancement and for indulging their desires. Those who satisfy their needs are idealized, while others who can serve no immediate purpose are devalued and even treated contemptuously. This shifting of overvaluation and denigration may occur frequently within the same relationship. There is an expectation of preferential treatment and special favors, without assuming reciprocal responsibilities.
The narcissistic personality's cognitive expansiveness, unrealistic goal fantasies, and tendency to overestimate abilities and achievements often leave the person quite vulnerable to injuries of self-esteem and pronounced feelings of unworthiness, should these grandiose self-expectations not be met. Although characteristically imperturbable and insouciant, repeated shortcomings and social humiliations may result in uncertainty and a loss of self-confidence. Over time, with the growing recognition of dissonance between self-perception and actual performance, self-disillusionment, feelings of fraudulence, and in some cases, a chronic state of dysthymia are likely to ensue. In other instances, a psychic blow generated from a single event (e.g., a humiliating defeat or a public criticism) may precipitate a brief but severe depressive episode. Such states rarely endure for extended periods, as depression is not experienced as consonant with the narcissist's self-image. The symptomatology of the narcissistic depression may be quite variable, shifting between dramatic expressions of worthlessness and self-deprecation to irritable demandingness and criticism of others. These perceptions tend to be attributed to external, ‘universal’ causes rather than to personal, inner inadequacies (Abramson et al., 1978). Consistent with this formulation, a narcissist may subtly accuse others of not supporting or caring for them enough. At other times, hostility may be directly expressed, as the narcissist becomes enraged at others being witness to his/her shame and humiliation.
The legend of Narcissus gives evidence that this constellation of personality patterns has been recognized throughout the existence of civilization and, though many on the international scene argue that it is a disorder found primarily in the western hemisphere, it has been found in a number of cultures. As a psychological construct, the narcissistic personality has enjoyed a rich history, with valuable contributions to its conceptualization emanating from many of the established schools of psychotherapy. As with any personality pattern, a review of these traditions is in order to fully understand the narcissistic pattern as a personologic system, and to gain a foundation for effective treatment.
As is the case with many current Diagnostic and statistical manual of mental disorders (DSM) constructs, the origins of narcissism as a psychological construct and mental disorder may be traced to psychoanalytically based explorations. Perhaps the first writing on the subject may be attributed to Havelock Ellis (1898/1933), who conceptualized it as autoeroticism, that is, sexual gratification without stimulation by another person. Paul Nacke (1899), the next year, used the term to describe the perversion of being preoccupied with the sight and pleasures of one's own body in a manner usually reserved for those of the opposite sex. In 1908, J. Sadger extended the concept to other so-called perversions, notably that of homosexuality. It was in this same era that classical psychoanalysis began to recognize the construct not as a characterologic structure, but certainly as a core component of personality development.
Freud's early dream work (1900) did not use the term, ‘narcissism,’ but he commented on several patients who seemed to show personality traits consistent with this disorder. These were patients who reported being favored significantly by their caretakers (primarily, their mother) and, resultantly, exhibited a kind of inimitable self-regard and indefatigable optimism that often provided for actual success. His first explicit formulations of narcissism (1910, 1911) emphasized its normal aspects, being a phase of development standing midway between autoeroticism and object love. According to Freud, this transitory period was marked by initially diverse and unconnected autoerotic sensations that eventually fused into what was experienced as one's body, which then become a single, unified love object. Within a few years, he aligned narcissism with libido theory and proposed that it ultimately matured and diffused into object relationships. Shortly thereafter he reformulated his thinking on the developmental sequence and spoke of the autoerotic phase as the ‘primary narcissistic condition.’ This first phase became the initial repository of libido from which emerged not only the love of self but love in general. In time Freud's conception of narcissism explicated a universal developmental process that continued through life but unfolded through sequential stages.
Freud, of course, recognized that difficulties could arise in this normal, sequential progression. First, there could be failures to advance from libidinal self-love to object love, and, second, ‘peculiarities’ could occur in the way the person expresses narcissistic love. In his only major paper devoted exclusively to narcissism, Freud (1914/1975) suggested that in certain cases—notably among ‘perverts and homosexuals’—libidinal self-centeredness stems from the child's feeling that caretakers cannot be depended upon to provide love reliably. Either rebuffed by their parents or subjected to fickle and erratic attention—seductive one moment and deprecating the next—these children ‘give up’ as far as trusting and investing in others as love objects. Rather than rely on the capriciousness of others or risk their rejection, these youngsters avoid the lasting attachment they achingly desire and decide instead that it is only themselves they can trust and therefore love.
It is important to note that this early reference to the term narcissism described in Freud's chapter was not intended as a formulation of a narcissistic character structure or personality type, but rather, one of several concepts that he posited as the source of libidinal self-cathexis. Freud's interest lay in exploring and elaborating variations in both the development and the nature of libidinal cathexis. Freud wrote of a narcissistic libidinal type for the first time in 1932 (p. 249), where he described this individual as follows:
The main interest is focused on self-preservation; the type is independent and not easily over awed… People of this type impress others as being ‘personalities’; it is on them that their fellow men are specially likely to lean; they readily assume the role of leader, give a fresh stimulus to cultural development or break down existing conditions.
Most striking in this quote is the stark contrast between Freud's characterization of the narcissist's strength and confidence, in comparison with the low self-esteem and feelings of emptiness, pain, and depression that members of the psychodynamic revival (e.g., Kohut, 1971; Forman, 1975) attribute to this personality. Disparities in characterizations such as these often arise as a consequence of shifts from one period to another in Freud's formulations. In this case, it can be traced to the fact that Freud identified several origins of narcissistic self-cathexis, only one of which is the type of parental caprice and rejection that may lead to feelings of emptiness and low self-esteem. As evident from earlier excerpts, and as later elaborated further, Freud's description of the narcissistic libidinal type, brief though it is, corresponds much more closely to the current DSM portrayal of the narcissistic personality than do several contemporary characterizations that trace its antecedents to either parental rebuff or unreliability. Relevant to this issue is a quote of Freud's reproduced later in the chapter that suggests that narcissistic self-investment is more likely to be a product of parental overvaluation than of parental devaluation.
The concept of the narcissistic personality has moved forward considerably from these early psychoanalytically oriented speculations. Now a well-recognized constellation of personality attributes spanning the range from normal to pathological variants, it is well ensconced in the DSM and reflects the thinking not only of psychodynamic constructs, but of cognitive, interpersonal, and learning modalities (to name but a few); its viability is quite solidly rooted throughout the clinical psychology community.
Before reviewing the various conceptualizations of the narcissistic personality disorder, it is most important to make special note of certain crucial differences between healthy and pathological narcissism; a self-image of pride, confidence, and self-valuation is not only very common across patients seen in psychotherapy in general, it is essential for the ubiquitous goal of self-esteem and positive growth. While an overvaluation of self, be it the product of overindulgence or a compensatory strategy, runs counter to most any therapeutic goal, the individual lacking in essential ‘healthy narcissism’ is faced with a quite different set of obstacles. For healthy self-esteem and good object relations to evolve, a child must experience unconditional love. However, an overabundance of unearned accolades or highly inaccurate and/or uncritical reflections of a child's behavior or accomplishments has the potential to catalyze an otherwise healthy constellation of traits to problematic ones. Some remarks on neuropsychological stage development as formulated by the senior author (Millon, 1996) are in order here.
Feelings of omnipotence begin shortly after birth but do not take hold in a meaningful fashion until the sensorimotor-autonomy stage. Every minor achievement of future narcissists is responded to with such favor as to give them a deluded sense of their own extraordinary self-worth. Extreme confidence in one's child need not be a disservice, if it is well earned. In the case of an evolving problematic narcissistic personality, however, a marked disparity will exist between the child's actual competence and the impression he/she has of it. Failures in parental guidance and control will play an important part during the intracortical-initiative stage. The child is encouraged to imagine, explore, and act without discipline and regulation. Unrestrained by the imposition of parental limits, the child's thoughts and behaviors may stray far beyond accepted boundaries of social reality. Untutored by parental discipline regarding the constraints of fear, guilt, and shame, the child may fail to develop those internal regulating mechanisms that result in self-control and social responsibility.
Given our dominant cultural orientation toward self-enhancement, it is often difficult to determine which self-focused traits indicate a narcissistic disorder and which are merely adaptive styles that fit societal modes. Where the line should be drawn between self-confidence and healthy self-esteem versus an artificially inflated and empty sense of self-worth is not always an easy task. The healthy narcissist should demonstrate, in addition to the usual characteristics of the personality type, social concerns, and interpersonal empathy, a genuine interest in the ideas and feelings of others, and a willingness to acknowledge one's personal role in problematic interpersonal relationships. Where the disorder is present, we see a persistent insensitivity to others, a general social exploitiveness, and lack of reciprocity in everyday relationships.
Several perspectives have been brought to bear on the concept of the narcissistic personality that deviate in major regards from classical psychoanalytic approaches. However, a review of major psychodynamic orientations to this personality is in order, as their exceptional contributions to modern formulations is integral.
Analytic theorists Otto Kernberg (1967, 1970) and Heinz Kohut (1966, 1968, 1971) lit the path that has prompted revitalized interest in many modern formulations of psychoanalytic theory and therapy; their conceptions of narcissism (and borderline) served as the cornerstone of this enthusiastic revival. Kernberg, in his restructuring of a diagnostic framework for characterology, de-emphasized the psychoanalytic classification schema that has traditionally been based on libidinal development. Stage sequences are referred to as a means of identifying levels of instinctual maturation (e.g., pregenital, genital). The vicissitudes of maturation give rise to the clinical features, defensive operations, level of severity, prognosis, and, most centrally, the structural integration or organization that is likely to characterize the individual's personality. Employing his framework of levels of structural organization as a model for constructing ‘a psychoanalytic classification of character pathology,’ Kernberg (1967, p. 655) described the features of the narcissist as follows:
These patients present an unusual degree of self-reference in their interactions with other people, a great need to be loved and admired by others, and a curious apparent contradiction between a very inflated concept of themselves and an inordinate need for tribute from others. Their emotional life is shallow. They experience little empathy for the feelings of others, they obtain very little enjoyment from life other than from the tributes they receive from others or from their own grandiose fantasies, and they feel restless and bored when external glitter wears off and no new sources feed their self-regard. They envy others, tend to idealize some people from whom they expect narcissistic supplies, and to depreciate and treat with contempt those from whom they do not expect anything (often their former idols). In general, their relationships with other people are clearly exploitative and sometimes parasitic. It is as if they feel they have the right to control and possess others and to exploit them without guilt feelings—and behind a surface which very often is charming and engaging, one senses coldness and ruthlessness. Very often such patients are considered to be ‘dependent’ because they need so much tribute and adoration from others, but on a deeper level they are completely unable really to depend on anybody because of their deep distrust and depreciation of others.
Kernberg asserted that the haughty and grandiose constellation of behaviors that characterize the narcissist is a defense against the projection of ‘oral’ rage that, in turn, stems from the narcissist's incapacity to depend on ‘internalized good objects.’ In this etiologic formulation, Kernberg claimed that the experiential background of most narcissists includes chronically cold parental figures who exhibit either indifference or covert, but spitefully aggressive, attitudes toward their children. At the same time, the young, future narcissist is often found to possess some special talent or status within the family, such as playing the role of ‘genius’ or being the ‘only child.’ This quality of specialness serves as a refuge, at first only temporarily but ultimately an often returned to haven that reliably offsets the underlying feeling of having been unloved by the vengefully rejecting parent.
Kohut, on the other hand, rejects the traditional Freudian and Kernbergian thesis that narcissistic self-investment results from a defensive withdrawal of object love attachments following a pattern of chronic parental coldness or vengeful spite. This classical view contends that narcissism is a result of developmental arrests or regressions to earlier points of fixation. Thus, the future narcissist, according to standard analytic metapsychology, regresses to or fails to progress through the usual developmental sequence of initial undifferentiated libido, followed by autoeroticism, narcissism, and, finally, object love. It is not the content as such but the sequence of libidinal maturation that Kohut challenges. His clinical observations have led him to assert that the primitive narcissistic libido has its own developmental line and sequence of continuity into adulthood. That is, it does not ‘fade away’ by becoming transformed into object-libido, as contended by classical theorists, but unfolds into its own set of mature narcissistic processes and structures. In healthy form, for example, these processes might include behaviors such as humor and creativity; similarly, and most significantly, it is through this narcissistic developmental sequence that the cohesive psychic structure of ‘self’ ultimately emerges.
Kohut contended, through much of his career, that narcissistic pathology occurs as a consequence of failures to integrate one of two major spheres of self-maturation, the ‘grandiose self’ and the ‘idealized parental imago.’ Confronted by realistic shortcomings that undermine early feelings of grandiose omnipotence, or subsequently recognizing the equally illusory nature of the idealized powers they have attributed to their parents, these children must find a way to overcome their ‘disappointments’ so as not to ‘fragment.’ If disillusioned, rejected, or experiencing cold and unempathic care at the earliest stages of self-development, serious pathology, such as psychotic or borderline states, will occur. Trauma or disappointment at a latter phase will have somewhat different repercussions depending on whether the difficulty centered on the development of the grandiose self or on the parental imago. In the former, the child will fail to develop the sense of fulfillment and self-confidence that comes from feeling worthwhile and valued; as a consequence, these needs will ‘split off’ and result in the persistent seeking of ‘narcissistic’ recognition through adulthood. Along the second line of self-development, children who are unable to ‘idealize’ their parents because of the latter's indifference or rejection will feel devastated, depressed, and empty. Through adulthood they will seek idealized parental surrogates who, inevitably, will fail to live up to the omnipotent powers the narcissists hoped to find within them. As they desperately seek an ideal that is ‘greater’ than themselves, they are often led to behave in a weak and self-effacing manner, a style that will enable others to overshadow them.
Late in his career, Kohut recognized a third sphere of self-maturation; this component, which he termed the ‘twinship transference’ (Kohut, 1984), represented an important addition to his thinking, though this addition was only described posthumously in work completed by his students. To Kohut, this sphere represented a third opportunity for self-cohesion, and arose in his thoughts as a result of a misinterpretation made in session; he originally felt that a patient's conjured, mythical figure was a transferential representation of him as the therapist, but this notion was rejected and explained lucidly by the patient. It appeared that this patient was experiencing the figure (a ‘genie in a bottle’) as a twin of herself, and needed only to remain as a presence she could talk to, but who did not have to respond. Kohut recognized an association between this phenomenon and the many pronounced silences he witnessed in therapy with her as well as other patients. This twin figure represented, to the patients, an opportunity to be self-validated, that is, to be understood and accepted by an entity just like the self. Also, it served the function of acquiring self-skills through the experience of sameness or likeness.
Kohut's is a developmental theory of self and not a personality characterization. Nevertheless, it leads to a clinical picture that is at variance with those of Freud, Kernberg, and the DSM-IV. The features that emerge from Kohut's descriptions have been summarized by Forman (1975). Listed among the more prominent are: (1) low self-esteem; (2) tendencies toward periodic hypochondriasis; and (3) feelings of emptiness or deadness. To illustrate their contrasting views, for example, the episodic depression that Kohut finds so characteristic of narcissistically injured persons is not seen by Kernberg to be a true depression at all. Rather, Kernberg contends that when ‘narcissists’ feel seriously disappointed or abandoned they may appear depressed on superficial examination, but they are, in fact, smoldering with constrained anger and revengeful resentment.
Kohut's model encourages the therapist to assume a sympathetic and accepting stance, while addressing the objective need for the patient to accept personal limitations. Short-term methods may be especially useful for crisis intervention and to establish a bridge to more long-term treatment procedures. Binder (1979) reports on the use of a brief treatment method for increasing self-esteem, also in preparation for a longer-term program. The hope here is to increase the patient's awareness of his/her vulnerability to shame and disappointment, as well as to increase the capacity to moderate intense affects, such as irritability and rage.
Differing significantly from the traditional views of psychoanalytically oriented concepts, the cognitive school has followed its model for treating the dysfunctional thoughts frequently seen in cases featuring clinical depression, and recognized that these cognitions regarding the self, the world, and the future also extend to the complex personality matrix beyond immediate clinical symptoms. Contributing the insightful analysis of the narcissistic personality from a cognitive point of view, Beck et al. (1990, p. 50) provide the following proposals concerning this individuals’ distorted belief system:
The core narcissistic beliefs are as follows: ‘Since I am special, I deserve special dispensations, privileges, and prerogatives,’ ‘I'm superior to others and they should acknowledge this,’ ‘I'm above the rules’.
Their main strategies consist of doing whatever they can to reinforce their superior status and to expand their personal domain. Thus, they may seek glory, wealth, position, power, and prestige as a way of continuously reinforcing their ‘superior’ image.
Their main affect is anger when other people do not accord them the admiration or respect that they believe they are entitled to, or otherwise thwart them in some way. They are prone to becoming depressed, however, if their strategies are foiled.
The narcissistic personality, according to Beck and his colleagues, can be conceptualized as stemming from a combination of dysfunctional schemas. The early foundation of these schemas is developed by direct and indirect messages from parents, siblings, and significant others, and by experiences that mold beliefs about personal uniqueness and self-importance. Narcissists regard themselves as special, exceptional, and justified in focusing exclusively on personal gratification; they expect admiration, deference, and compliance from others, and their expectations of the future focus on the realization of grandiose fantasies. At the same time, beliefs about the importance of other people's feelings are conspicuously lacking. Behavior is affected by deficits in cooperation and reciprocal social interaction, as well as by excesses in demanding, self-indulgent, and sometimes aggressive behaviors.
The various techniques of dysfunctional thought modification, cognitive reframing, and similar techniques espoused by Beck (and many other cognitively oriented thinkers, e.g., Sperry, 1999) are well-known and highly validated components of contemporary clinical practice. More recently, Young (1999) has provided insightful cognitive schema-focused inroads to the challenges of personality pathology. Young's approach represents an integration of cognitive therapy with intrapsychic and gestalt modalities, and expands significantly on traditional cognitive approaches by giving special attention to the therapeutic relationship, early experience, and affect. Although he does not explicate personality-specific treatment regimens, his approach is very much in concert with the ideals set forth in a later discussion within this chapter regarding systematic integration of differing modalities; it differs, however, in its use of a modality within the boundaries of psychology proper (that is, cognitive theory) as the central, binding construct, rather than seeking organizing principles from the overarching natural sciences.
Timothy Leary (1957), a disciple of Horney and others of the social and interpersonal school of thought, pioneered what may be termed the ‘interpersonal’ approach to the problem of personality pathology, and extended their notions to what he terms ‘adjustment through competition.’ Leary (1957) spoke of this pattern as demonstrating a competitive self-confident narcissism, which he captures well in the following series of quotes:
In its maladaptive extreme it becomes a smug, cold, selfish, exploitive social role. In this case the adaptive self-confidence and independence become exaggerated into a self-oriented rejection of others…
These individuals feel most secure when they are independent of other people… The narcissist puts… distance between himself and others-wants to be independent of and superior to the ‘other one’. Dependence is terrifying.
p. 332
The second group of… patients… are those whose self-regard has received a decent defeat. They often report the most colorful and fearful symptomatology… The superficial impression of depression or dependence is deceptive. Psychological testing or perceptive interviewing will reveal that the patients are not as anxious or depressed as they appear. What becomes evident is a narcissistic concern with their own reactions, their own sensitivities. The precipitating cause for their entrance to the clinic is usually a shift in their life situation, which causes frustration or a blow to their pride.
p. 335
A number of interpersonally oriented theorists followed Leary's interpersonal perspective and drafted their models of various personality disorders in highly fruitful work. Perhaps most notable among this group is Lorna Benjamin (1993) who has formulated a complex analysis of the narcissistic character. In her recent work she describes this personality as follows:
There is extreme vulnerability to criticism or being ignored, together with a strong wish for love, support, and admiring deference from others. The baseline position involves noncontingent love of self and presumptive control of others. If the support is withdrawn, or if there is any evidence of lack of perfection, the self-concept degrades to severe self-criticism. Totally lacking in empathy, these persons treat others with contempt, and hold the self above and beyond the fray.
p. 147
[The narcissist] expects to be given whatever he or she wants and needs, no matter what it might mean to others. This does not include active deception, but rather is a consequence of the belief that he or she is ‘entitled’. For example, the narcissistic personality disorder would not set out to con a ‘little old lady’ out of her life savings; however, if she offered them, the narcissistic personality disorder would accept such a gift without reflection about its impact on her. [He/She] will expect great dedication, overwork, and heroic performance from the people associated with him or her—without giving any thought to the impact of this pattern on their lives.
p. 150
Benjamin's (1993) interpersonal approach suggests that achieving the first crucial therapeutic objective, the patient's recognition of problematic interpersonal patterns, is particularly challenging with narcissistic patients. While the therapist's empathic understanding is necessary in facilitating this process, the form of therapist statements needs to be carefully considered to prevent encouraging narcissistic tendencies inadvertently. Benjamin provides examples of more and less therapeutically effective statements in discussing a narcissistic patient and his dissatisfied wife. An example of a response that probably encourages a narcissistic schema is ‘You have been trying so hard to make things go well, and here she (your wife) just comes back with complaints.’ Benjamin notes that such a therapist response would probably enhance the patient's pattern of externalizing and blaming. A preferred alternative would be, ‘you have been trying so hard to make things work well, and you feel just devastated to hear that they aren't going as perfectly as you thought’. The advantage of this latter response is that it encourages the patient to examine internal processes and reaction patterns.
Present habits become clearer when their functional significance is grasped. To this end, the patient's pattern of emotional reactions such as envy and feelings of entitlement can be traced to early interactions with significant others. Internalized representations of these early figures continue to guide present functioning. As the patient comes to recognize which attitudes and behaviors are motivated by earlier ‘internalizations,’ he may become freer to modify them. An example provided by Benjamin considers a patient that expressed anger and envy about a friend's receipt of public acknowledgment of success. The therapist shifted the patient's focus to issues underlying the envy by asking the patient how his mother would react to such news. Further discussion helped clarify to the patient that his concern about her reaction of disappointment (real or internalized) supports his unpleasant envious feelings. Such insight can help the patient resolve to detach from internalized representations of such figures. Finally, it is noted that once the patient accepts that unattainable ambitions and maladaptive behaviors need to be given up in favor of more realistic and fruitful cognitive and interactive habits, the bulk of the therapeutic challenge may be well on its way; new learning may be a relatively easy undertaking thereafter.
The modalities described above are but a few of the best known and most often utilized in interventions with the narcissistic personality. All have been considered as serious contenders for ‘definitive’ status, and all have been criticized for various shortcomings, which may be summarized as a whole by the following: each contributes valuably by focusing on an area of treatment that is necessary, but each falls short in neglecting other important treatment aspects. To this we may add: efforts at using each others’ techniques is by no means a new idea, but what remains lacking is a comprehensive, coherent set of principles that allows true synergistic, integrative therapy to take place. In an earlier publication, the senior author (Millon, 1999) outlined a method for addressing these shortcomings.
As stated previously, despite their undeniably brilliant contributions throughout their rich history, no single school of psychological thought may lay claim to a full contextual understanding and process of treating any personality pathology, inclusive of the narcissist. The very nature of personality precludes this; as the senior author has stated in numerous other places (e.g., Millon, 1990, 1996, 1999; Millon and Davis, 1996), personality is a naturally-occurring system encompassing the spectrum of modalities represented in the virtuous though unilateral psychotherapy schools. As these phenomenological, behavioral, intrapsychic, and biophysical entities bind together and reinforce one another in their perpetual and reciprocal organization, it is virtually impossible for any unidimensional school's approach to effectively modify dysfunctional personologic processes. For a therapy to be effective, it must be as tenacious as the personality system itself, approaching difficulties from a broad-based paradigm that incorporates all the modalities present in the personality.
In the last decade of the twentieth century, Millon (1990) reformulated his biosocial-learning model of personality (Millon, 1981) to align with the greater principles of natural sciences. According to Millon, only through the perspective of the naturally occurring world could principles be derived that provided for a comprehensive, synergistic science of personology. This science would include an overarching theory, a means of classification for the various phenomena found as a result of the theory, a method for objectively identifying and assessing those phenomena, and a system for intervention, or modification, that followed logically from these three prior elements. Furthermore, the science needed to address the disparate elements (e.g., cognitions, intrapsychic structures, etc.), which had, over the history of personologic intervention, presented themselves in clinical settings. Finally, this system needed to interface with and augment the extant classification methods (i.e., DSM-IV-TR, 2000) used by the community of contemporary research and practice-oriented clinical professionals.
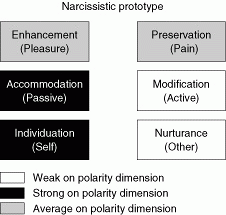
The most germane and generative source for conceptualizing the constellation of patterns that comprise the Axis II personalities, according to Millon, was the established science of evolutionary biology. Here, he felt, was a sister science whose principles were closely in alignment with the expressions of personality, and were also shared with the myriad of other sciences (e.g., particle physics, organic chemistry) that were well-grounded in terms of organizing principles. In examining the tenets of evolution, Millon deduced that all organisms (and specifically, personality) were possessed of three motivating aims that may be expressed as bipolarities, as illustrated in Figure 23.1: existence (pleasure-seeking versus pain avoidance), adaptation (active modification versus passive assimilation), and reproduction (self versus other nurturing). While a full explication of the derivation of these polarities is beyond the scope of this chapter, a basic understanding is key to conceptualizing the narcissistic personality in preparation for treatment. Their primary qualities are reviewed in context with the structure of the narcissistic personality.
The first polarity, that of existence, does not suggest a strong proclivity for either pleasure seeking or pain avoidance in basic drives. These qualities may vary considerably across situations and among narcissistic individuals, especially when characteristics of other personalities are present (as is frequently the case; see discussion on subtypes in the case examples, below). What is more central in the polarity matrix of the narcissist is the primacy of both passive/accommodation and self/individuation. What this translates into is the narcissist's focus on self as the center of one's existence, with a comparable indifference to others (nurturance). According to Millon, and in contrast with many of the classic psychodynamically oriented conceptions of the narcissist, the etiology of this personality pattern is owed to an unusual developmental background in which others overvalued the narcissists’ self-worth by providing attention and tribute unconditionally. As a result, they fail to develop the motivation and skills ordinarily necessary to elicit these tributes. To them, merely being who they are is sufficient; one does not have to do anything, no less achieve, to elicit signs of admiration and high self-esteem. Narcissists are passive, therefore, because they expect the rest of the world to do their bidding without reciprocal efforts.
|
|
Fig. 23.1 Narcissistic personality disorder, in accordance with the Millon Evolutionary Model. |
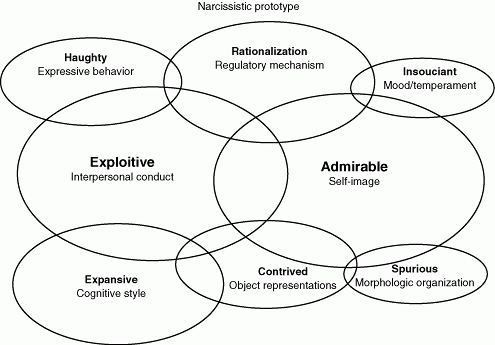
With these basic motivating aims in mind, it is now possible to examine the expression of the narcissistic personality across the various functional and structural personologic domains outlined by the theory (see Millon and Davis, 1996). As noted previously, these domains suggest representation of behavioral, phenomenological, intrapsychic, and biophysical elements of personality that coincide with a myriad of therapeutic traditions. The relative salience of these domains in the prototypal narcissistic personality, as conceived by Millon, are represented graphically in Figure 23.2.
This behavioral domain holds that it is not uncommon for narcissists to act in an arrogant, supercilious, and disdainful manner. There is also a tendency for them to flout conventional rules of shared social living. Viewing reciprocal social responsibilities as being inapplicable to themselves, they show and act in a manner that indicates a disregard for matters of personal integrity and an indifference to the rights of others. When not faced with humiliating or stressful situations, narcissists convey a calm and self-assured quality in their social behavior. Their seemingly untroubled and self-satisfied air is viewed, by some, as a sign of confident equanimity. Others respond to it much less favorably. To them, these behaviors reflect immodesty, presumptuousness, pretentiousness, and a haughty, snobbish, cocksure, and arrogant way of relating to people. Narcissists appear to lack humility and are overly self-centered and ungenerous. They characteristically, but usually unwittingly, exploit others, take them for granted, and expect others to serve them, without giving much in return. Their self-conceit is viewed by most as unwarranted; it smacks of being ‘uppity’ and superior, without the requisite substance to justify it.
Also a part of the behavioral domain, but in concert with interpersonal approaches, narcissists feel entitled, expecting special favors without assuming reciprocal responsibilities. Not only are they unempathic, but they take others for granted, are shameless in the process, and use others to enhance their own personal desires. Unfortunately for them, narcissists must come to terms with the fact that they live in a world composed of others. No matter how preferred their fantasies may be, they must relate and deal with all the complications and frustrations that real relationships entail. Furthermore, and no matter how satisfying it may be to reinforce oneself, it is all the more gratifying if one can arrange one's environment so that others will contribute their applause as well. Of course, true to their fashion, narcissists will seek to accomplish this with minimal effort and reciprocity on their part. In fact, some narcissists assume that others feel ‘honored’ in having a relationship with them, and that others receive as much pleasure in providing them with favors and attention as the narcissist experiences in accepting these tributes.
|
|
Fig. 23.2 Salience of personologic domains, narcissistic personality. |
This phenomenological domain notes that narcissists exhibit an undisciplined imagination, and seem preoccupied with immature and self-glorifying fantasies of success, beauty, or romance. Although nondelusional, narcissists are minimally constrained by reality. They also take liberties with facts, embellishing them, even lying, to redeem their illusions about their self-worth. Narcissists are cognitively expansive. They place few limits on either their fantasies or rationalizations, and their imagination is left to run free of the constraints of reality or the views of others. They are inclined to exaggerate their powers, to freely transform failures into successes, to construct lengthy and intricate rationalizations that inflate their self-worth or justify what they feel is their due, quickly depreciating those who refuse to accept or enhance their self-image.
Another phenomenological domain, this one observes that the narcissist feels justified in claiming special status, and has little conception of the objectionable, even irrational nature of his or her behavior. It is the narcissists’ belief that they are special, if not unique persons that deserve great admiration from others. Quite frequently they act in a grandiose and self-assured manner, often without commensurate achievements. Although they expect to be seen as meritorious, most narcissists are viewed by others as egotistic, inconsiderate, and arrogant. Their self-image is that they are superior persons, ‘extraspecial’ individuals who are entitled to unusual rights and privileges. This view of their self-worth is fixed so firmly in their minds that they rarely question whether it is valid. Moreover, anyone who fails to respect them is viewed with contempt and scorn.
The final phenomenological domain holds that internalized representations of past experiences are deeply embedded and serve as a template for evaluating new life experiences. For the narcissist, these object representations are composed far more than usual of illusory and changing memories. Problematic past relationships are readily refashioned so as to appear entirely consonant with the narcissist's high sense of self-worth. Unacceptable impulses and deprecatory evaluations are quickly transformed so as to enable this personality to maintain his preferred and contrived image of both himself and his past. Fortunately for most narcissists, they were led by their parents to believe that they were invariably lovable and perfect, regardless of what they did and what they thought. Such an idyllic existence could not long endure; the world beyond home is not likely to have been so benign and accepting. As a consequence, the narcissist must transform the less palatable aspects of his past so they are consistent with what he wishes they were, rather than what they were, in fact.
This first intrapsychic domain poses the question: What happens if narcissists are not successful, if they face personal failures and social humiliations? What if realistic events topple them from their illusory world of eminence and superiority? What behaviors do they show and what mechanisms do they employ to save their wounds? While they are still confident and self-assured, narcissists are facile at the art of self-deception, devising plausible reasons to justify self-centered and socially inconsiderate behaviors. With an air of arrogance, narcissists are excellent at rationalizing their difficulties, offering alibis to put themselves in the best possible light, despite evident shortcomings or failures on their part. If rationalizations fail, dejection and feelings of emptiness are likely. Narcissists will have little recourse other than to turn for solace to their fantasies. Failing to achieve their aims and at a loss as to what they can do next, they are likely to revert to themselves to provide comfort and consolation. It is at these times that their lifelong talent for imagination takes over. These processes enable them to create a fanciful world in which they can redeem themselves and reassert their pride and status. As narcissists are unaccustomed to self-control and objective reality testing, their powers of imagination have free rein to weave intricate resolutions to their difficulties.
Narcissists hold a sanguine outlook on life that is founded on an unusual set of early intrapsychic experiences that only rarely are duplicated in later life. They suffer few conflicts; their past has supplied them, perhaps too well, with high expectations and encouragement. As a result, they are inclined to trust others and to feel confident that matters will work out well for them. Therefore, the structural organization of the narcissist's inner world for dealing with life tends to be quite flimsy and transparent, in contrast to the common misperception of a more substantial and dynamically orchestrated personality organization. Owing to the misleading nature of their early experiences, this personality has never developed the inner skills necessary to regulate impulses, to channel needs, or to acquire contingency strategies for frustrations, routine failures, and problem resolution. Consequently, even the routine demands of everyday life may be viewed as annoying incursions by narcissists. Such responsibilities are experienced as demeaning. Driven by their need to maintain their illusion of superiority in the face of conflict, some may turn against others, accusing them of their own deceptions, selfishness, and irrationalities. It is at these times that the fragility and pathology of the narcissist becomes clearly evident. ‘Breakdowns’ in the defensive structure of this personality, however, are not too common. More typically, the exploitive behaviors and intrapsychic maneuvers of narcissists prove highly adaptive and provide them with the means of thwarting serious or prolonged periods of dejection or decompensation.
This last, biophysically oriented domain predicts that narcissists are generally roused by the facile workings of their imagination, and usually experience a pervasive sense of well-being, a buoyancy of mood, and an optimism of outlook—except when their sense of superiority has been punctured. Normally, however, affect, though based often on their semigrandiose distortions of reality, is generally relaxed, if not cheerful and carefree. There is a general air of nonchalance, an imperturbability, a feigned tranquility. Should the balloon be burst, however, there is a rapid turn to either an edgy irritability and annoyance with others or to repeated bouts of dejection that are characterized by feeling humiliated and empty. Shaken by these circumstances, one is likely to see briefly displayed a vacillation between rage, shame, and feelings of emptiness.
The following represents the senior author's (T.M.) synergistic therapeutic approach for the narcissistic personality patterns that fully integrates the traditional psychotherapy schools reviewed in earlier sections.
The most salient narcissistic dysfunctions are manifest in the self-image and interpersonal conduct domains, and are expressed in the form of an admirable self-concept and unempathic, even exploitive treatment of others. At best, the narcissist confidently displays achievements and behaves in an entitled, and occasionally grating manner. Facts are twisted and the line between fantasy and reality becomes blurred as narcissists boast of unsupportable personal successes and talent; at the same time, interpersonal behavior moves toward the inconsiderate, arrogant, and exploitive. Others may express irritation at the nonsubstantiated grandiosity of the narcissist's fantasies and at the inequitable nature of his or her social interactions. However, taking advantage of others to indulge desires and enhance his or her situation, with no consideration of reciprocal responsibilities, is considered justified owing to their sense of self-importance. As long as this self-schema is maintained, the narcissist has little chance of finding motivation to effect changes in other areas. Thus, a likely first therapeutic intervention may be a cognitive refocusing on acceptance of a realistic self-image. This may be done via reframing techniques aimed at acclimating the individual to a balanced view of self. Later techniques may include more direct cognitive disputes of the person's perceived flawlessness. As the cognitive foundation on which exploitive behavior is justified is weakened, interventions that increase empathic understanding and cooperative interactions can become the clinical focus. Synergistically speaking, this process may be enhanced by modeling an empathic and understanding stance (as suggested by Kohut, 1971, 1984) and allowing for a transference identification to take place. The therapist should avoid being ‘infallible;’ rather, as the therapeutic relationship is solidified, it may be beneficial for the individual to see the therapist as a competent and respectable professional, but not as omnipotent or infallible. The benefits of these approaches—warmer receptions from others and a more solid personal sense of efficacy—can then be integrated to encourage further development.
Successful intervention in the primary domains can lead to beneficial advances within secondary domains. Furthermore, resolving secondary domain dysfunctions therapeutically can also bolster progress in the more salient areas. Behavioral interventions, including role-playing, techniques of behavioral inhibition, modeling, and systematic desensitization, which elicit nonadulating therapeutic feedback, can help extinguish haughty expressive behavior as well as exploitive interpersonal conduct. These can in turn result in more genuine interpersonal events that subsequently serve as useful counterexamples to unrealistic or contrived object representations. Such exercises and the results they generate may set the groundwork for a more searching exploration of the patient's internalized schemas and their negative consequences. Illusory ideas and memories and pretentious attitudes can eventually be replaced with reality-based experiences and object representations.
As the patient comes to grasp the nonadaptive nature of the expansive narcissistic cognitive style, preoccupation with immature fantasies may be decreased. As cognitive and behavioral dysfunctions come to be regulated, the narcissist's insouciant mood is also likely to be naturally tempered. Baseline nonchalance and buoyancy can be replaced with more context-appropriate feelings. The rages, shame, and emptiness that resulted from undeniable discrepancies between self-image and reality are often modified along with the patient's self-concept. In some cases, psychopharmacological intervention may be indicated if a resistant depression appears to be interfering with therapeutic progress.
Ultimately, therapeutic interventions in the preceding domains can have a beneficial effect on this personality's spurious morphologic organization. Flimsy defensive strategies can be replaced by stronger coping mechanisms, and the stress-reducing regulatory mechanism of rationalization can be given up for more realistic and growth-fostering inner and outer self-representations.
Characteristic narcissistic confidence, arrogance, and exploitive egocentricity is based on a deeply ingrained, if sometimes fragile, self-image of superior self-worth. Achievements and manifest talents are often not proportional to the narcissist's presumptions of ‘specialness’. The alternative to maintaining unsustainable beliefs of personal infallibility, that is, recognition of imperfections, limitations, and flaws, however, is tantamount to reconciliation with failure and utter worthlessness. For some narcissists such unreal expectations for themselves stem from experiences in which otherwise doting parents became unsupportive or even abusive at the manifestation of ‘imperfection’ in their child; others simply cannot conceive of life among the ‘masses.’ As those around narcissists ‘dare’ not to notice their special uniqueness, and then behave appropriately, narcissists turn away from attempting to secure comfort from ‘simple-minded’ others whose place it is to tend him or her. Instead, they increasingly rely on themselves as a source of rewards. Turning inward provides opportunity to pamper and ponder the self, and to fantasize about the great recognition that will come to shine on the narcissist one day. Thus narcissists, who start out high on the self-polarity, become increasingly less other oriented with the passage of time.
In the mind of the narcissist, others are the source of all of his or her troubles and difficulties, and are responsible for any failures to achieve fantasized goals. Not only do others have to make this up to the narcissist, but their natural inferiority dictates that they should attend to all the narcissist's whims and needs. The narcissist's exploitive egocentricity is not the two-faced, contract-breaking, means-to-an-end exploitiveness of the antisocial. Rather than actively planning, the narcissists’ arrogance and snobbish sense of superiority lead them to believe that others ‘owe’ them something, and their self-centered convictions of genuine entitlement results in the ‘passive’ exploitation of others. The sense of superiority often results in a lack of goal-oriented behavior in general; narcissists simply believe that good things are their due, a natural byproduct of their intrinsic ‘specialness’. This nonadaptive bias toward the passive end of the active-passive dimension often results in personal, social, and professional stagnation.
A main therapeutic goal in trying to increase a narcissist's other-orientedness and active goal-directed behaviors is to help him or her accept that while human imperfections are inevitable, they are not necessarily a sign of failure or worthlessness. If narcissists can appreciate the benefits (lack of pressure, decreased fear of criticism) of not needing to be infallible, they may be able to consider their part of the responsibility for any difficulties they may be having. Active problem solving and improved interpersonal interaction is a worthy goal.
Narcissists’ characteristic difficulties almost all stem from their lack of solid contact with reality. The same disdain for objectivity prevents effective coping with subsequent troubles. The problem-perpetuating cycle begins with early experiences that provide noncontingent praise that teach narcissists to value themselves regardless of accomplishments. Their inflated sense of self-worth causes them to conclude that there is little reason to apply any systematic effort toward acquiring skills and competencies when ‘it is so clear that’ they already possess such obvious and valuable talents and aptitudes. Their natural gifts, they believe, are reason enough for them to achieve their goals and earn others’ respect.
In time, narcissists come to realize that others, who are expending considerable effort to achieve goals, are moving ahead and receiving more recognition. Envious and resentful that the acknowledgment that is ‘rightfully theirs’ is being bestowed upon others, narcissists intensify their boasting and air of superiority. Eventually, the prospect of actually going out in the world and risking humiliating failure for all to witness becomes untenable in the face of the grand illusions of personal competence narcissists feed to themselves and others.
The problems posed by narcissistic illusions of competence feed into and are exacerbated by social alienation and lack of self-controls. The conviction that they are ‘entitled’ leads narcissists to harbor disdain for social customs and cooperative living. A lack of respect for others’ opinions and feelings lead to a failure to integrate normative feedback about their behaviors and illusions. In fact, the conviction that others are simple minded and naive cause narcissists to retreat further into their illusory and isolated world of fantasy at every hint of disapproval. Self-serving rationalizations of others’ lack of adulation can escalate until complementary paranoid delusions of persecution and grandiose illusions become firmly entrenched. Were narcissists to possess some self-controls, their social isolation may not have such dire consequences. Internal reality testing, however, is as neglected as are external inputs. Rathezr than working to realize ambitions, threat of failure and conceit push narcissists to retain their admirable self-image through fantasy. The regard for reality that would prevent narcissists from perpetuating their psychological and coping difficulties are notably absent.
Therapeutic intervention offers an inroad into the pathological cycle through the modification of the overblown self-image. As the self is appraised more realistically, perfection is seen as unattainable, and the need to employ self-discipline to achieve goals is understood, the narcissistic patient may come to recognize and accept his or her similarity to others. As the patient begins to make genuine efforts to improve the genuine quality of life, an appreciation for others’ hard work and achievements may develop and replace chronic envy and resentment. Intervention aimed directly at increasing empathic understanding can lead to a sensitivity to other's feelings that fosters motivation to adopt cooperative interpersonal behaviors. Toward this end, the narcissist can choose to learn to tolerate and make use of constructive social feedback. Day to day successes can eventually provide the gratification that can bolster the patient's resolve not to perpetuate nonadaptive cognitive and behavioral strategies, and help control the impulse to escape into unproductive flights of fantasy. If social isolation is thus decreased, therapeutic work has led to difficult-to-realize modifications in the patient's deeply entrenched lifestyle.
As a general note, working with narcissists is difficult for therapists who seek change in a patient's personality. Benjamin (1993) notes that the patient's presumptions of entitlement and admiration may encourage the therapist to join the patient in mutual applause, while criticizing the rest of the world. Alternatively, the patient may maintain a stance of superiority. Neither kind of therapeutic alliance helps the patient achieve more adaptive functioning. Any confrontation of the narcissist's patterns will be experienced as criticism, however, and chances are high that the patient will choose to terminate therapy. Benjamin suggests that narcissists may consider changing their interpersonal habits if they are convinced that it will lead to a more favorable response from others. Overall, best therapeutic outcomes may come from honest interpretations presented in a tone of approval and acceptance. Good therapeutic gain will result when the patient internalizes the therapist's empathic acceptance of the patient's faults and deficits. As children, most narcissists were noncontingently praised for their ‘perfection,’ and may have been led to feel like utter failures when their inevitable lack of perfection was too apparent to be ignored. The therapist's attitude that faults are inevitable and perfectly human provides an opportunity for realistic self-evaluation of self-worth that were rarely provided in the typical narcissist's early learning history. Carefully timed self-disclosures of the therapist's reactions toward the patient can also potentially lead to substantial therapeutic gain. Such information can encourage the patient's insight into the negative impact of his/her habitual behaviors on others, and, if revealed with supportive skill, can foster motivation to modify these habits.
As noted previously, effective therapy must match the personality's system of interweaving domains, for unilateral approaches will lack the tenacity to effect broad-based changes. From the functional and structural domains listed in an earlier section, techniques may be suggested that interface well with the personality constellation (see Table 23.1 for an overview).
Narcissists are not inclined to seek therapy. Their pride disposes them to reject the imperfection-confirming ‘weak’ role of patient. Most are convinced they can get along quite well on their own. Often if a narcissist does accept voluntary treatment, he or she will try to enlist the therapist to support the opinion that the patient's problems are largely the result of the imperfections and weaknesses of others. Alternatively, the narcissist may adopt a stance of superiority and discredit the therapist, or terminate treatment prematurely. In sum, narcissists will not accede to therapy willingly. Moreover, once involved, they will maintain a well-measured distance from the therapist, resist the searching probes of personal exploration, become indignant over implications of deficiencies on their part, and seek to shift responsibility for these lacks to others. The treatment setting may give witness to struggles in which narcissists seek to outwit the therapist and assert their dominance. Stone (1993) notes that much of the narcissistic patient's sarcasm, devaluation, and domination toward the therapist can been seen as a ‘test’ of whether the therapist will respond in kind and therefore, like the patient's parents (who may have modeled the offensive behavior), is not to be trusted. Setting limits without resorting to an accusatory or attacking stance can prove to be invaluable aids in working with these patients. Great patience and equanimity are required to establish the spirit of genuine confidence and respect without which the chances of achieving reconstructive personality change becomes even slimmer.
|
Table 23.1 Domain-oriented tactical modalities
|
||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
As mentioned previously, personality disorders rarely present in what may be termed ‘prototypal’ cases. We will not usually be confronted with a ‘pure’ narcissist; rather, admixtures of narcissism with other personality variants are usually seen. Experience with the Millon Clinical Multiaxial Inventory scores III (Millon et al., 1997) suggest several personality blends that incorporate distinct narcissistic features. A review of the developmental background of other narcissistic personalities contributed further to the variants described in the following two cases.
Jules, 34, was a young hydraulics salesman who had ‘risen from the plebs’ to find unmitigated success in the sales field until a blatant disregard for the terms of a contract brought his actions into question, and he was asked to see a counselor through his company's employee assistance plan. Initially, he seemed to be simply a self-confident, gregarious man, but this quickly gave way to a more realistic picture of an intimidating, manipulative individual. He proudly shared the secret to his success: use unethical techniques others won't. He saw himself as separate and apart from the crowd of salesmen, as he was one who would not get ‘pushed’ by a customer. He also explained with a knowing grin that it was possible to butter up any deal with a little fraudulent use of the expense account. Jules viewed himself as a ‘free agent,’ one who didn't feel the customary rules of employment, society, and life applied to him. Consequently, this freedom allowed him to successfully pursue virtually anything he wanted. Perhaps one of the most striking moments of the interview came when Jules was describing his parents. His mother, a quiet, dutiful woman was seen by Jules as ‘nothing really special;’ his father, on the other hand, by virtue of his beer consumption and the ability to make his point clear (with a ‘whipping’) over a minor infraction, was seen as an impressive, revered figure.
Unprincipled narcissists such as Jules are seen most often these last two or three decades in drug rehabilitation programs, centers for youth offenders, and in jails and prisons. Although these individuals often are successful in society, keeping their activities just within the boundaries of the law, they enter into clinical treatment rather infrequently. Jules's behavior was characterized by an arrogant sense of self-worth, an indifference to the welfare of others, and a fraudulent and intimidating social manner. There was a desire to exploit others, to expect special recognitions and considerations without assuming reciprocal responsibilities. A deficient social conscience was evident in his tendency to flout conventions, to engage in actions that raise questions of personal integrity, and to disregard the rights of others. Achievement deficits and social irresponsibilities were justified by expansive fantasies and frank prevarications. Descriptively, we may characterize Jules as devoid of a superego, that is, evidencing an unscrupulous, amoral, and deceptive approach to his relationships with others. More than merely disloyal and exploitive, he was likely to blend in with society's con-men and charlatans, many of whom are vindictive and contemptuous of their victims. The features clearly seen in Jules support the conclusion that he was an admixture of both narcissistic and antisocial personality characteristics.
Jules evidenced a rash willingness to risk harm and was notably fearless in the face of threats and punitive action. Malicious tendencies were projected outward, precipitating frequent personal and family difficulties, as well as occasional legal entanglements. Vengeful gratification was often obtained by humiliating and dominating others. He operated as if he had no principles other than exploiting others for his personal gain. Lacking a genuine sense of guilt and possessing little social conscience, he was an opportunist who enjoyed the process of swindling others, outwitting them in a game he enjoyed playing in which others were held in contempt owing to the ease with which they can be seduced. Relationships survived only as long as he had something to gain. People were dropped with no thought to the anguish they may have experienced as a consequence of his careless and irresponsible behaviors.
Jules displayed an indifference to truth that, if brought to his attention, was likely to elicit an attitude of nonchalant indifference. He was skillful in the ways of social influence, was capable of feigning an air of justified innocence, and was adept in deceiving others with charm and glibness. Lacking any deep feelings of loyalty, he successfully schemed beneath a veneer of politeness and civility. His principal orientation was that of outwitting others, getting power, and exploiting them ‘before they do it to you.’ He often carried a chip-on-the shoulder attitude, a readiness to attack those who were distrusted or who could be used as scapegoats. Jules attempted to present an image of cool strength, acting tough, arrogant, and fearless. To prove his courage, he may have invited danger and punishment. But punishment only verifies his unconscious recognition that he deserves to be punished. Rather than having a deterrent effect, it only reinforces his exploitive and unprincipled behaviors.
While it would be important to garner understanding of Jules's point of view and express accurate empathy, it would be equally crucial for the therapist to maintain a steadfast posture that would remain focused on tangible interventions. It would be ill-advised to indulge in self-image techniques that may guide the process into digressions about his perceived grandeur. Of primary importance would be a cognitive reorientation that would enhance Jules's alertness to the needs of others, while diminishing his self-important illusion. On an interpersonal level, it would be necessary to adjust Jules's social outlook, which would include clarifying his active-passive conflict. One of his primary perpetuations is his tendency to actively exploit others, yet to maintain a laid-back, uncaring attitude regarding anyone or anything that doesn't immediately affect him. A major focus of behavioral therapy for Jules would be to introduce steps to overcome his deficient controls, while instilling a greater sense of empathy for others.
Short-term methods were suitable for Jules, although environmental management, psychopharmacologic treatment, and behavior modification could be safely disqualified. The most effective course to begin changing some of his troubling attitudes and behavior was cognitive reorientation. As the therapeutic relationship began to develop and a modicum of comfort was established, the therapist was able to begin confronting Jules's dysfunctional beliefs and expectations. Short-term interpersonal methods were also used to explore and adjust his social skills and demeanor. More expressive and time-extended techniques were not justified here, as it is more prudent in a case such as this to work at controlling Jules's illusions, rather than to foster possible grander illusions. Group therapy was most beneficial here, as the members provided a means for Jules to express himself without his usual arrogant front in a benevolent and noncritical environment.
While it was very important to avoid emphasizing Jules's negative attributes, the therapeutic relationship also depended upon not allowing him to assert dominance in treatment in his usual way. He fully believed himself to be perfect, and this made him notably disinclined to change any of his attitudes. He refused, initially, to commit to any amount of time investment in therapy, and early cession would have virtually guaranteed quick relapse. Throughout the early stages, he maintained a careful distance from the therapist, and would attempt to thwart any exploration of personal issues that may have implied any deficiency on his part. Cognitive confrontations arranged in graduated depths (beginning with presentation of alternatives, evolving to more direct statements challenging Jules’ current mind set) were able to counter these efforts, and difficulties rooted in his evasiveness and unwillingness, though sometimes disruptive, were dealt with directly and firmly, but without emitting disapproval. With this consistently honest and confrontive stance, the treatment setting went from an environment that frequently gave witness to attempts at dominance, to one of relative cooperation and efficacious collaboration.
Jules routinely thought of others, regardless of their status, position, or intellect, as callow and stupid. Rather than ever question his viewpoint, his response to any challenge (including those he instigated) was, without question, that the other person was not only wrong, but an idiot. A direct cognitive approach confronted this habit of assuming everyone else to be wrong, and claiming superiority based on frequent arguments he could win by acumen and intimidation. Gone unchecked, this habit would have continued to encourage Jules's arrogant and presumptuous demeanor.
Jules had not sought therapy voluntarily, and was convinced that there really was no problem. After all, there were no current failures or dissatisfactions on his current ‘scorecard,’ so what could be wrong? Even if he had brought himself to seek help due, perhaps, to an unaccustomed loss in sales, or a declining social context, it would have been unlikely that he would conceive of any trouble as linked to his actions or demeanor. It was quite transparent that entering this office put his pride on the line, and that was not a position he was inclined to take lightly. This particularly defensive stance also called for direct, firm confrontation, while maintaining a safe but honest therapeutic environment through an empathic attitude expressed by the therapist. Jules's acceptance of this environment was questionable, and his attitude towards the process ambivalent, until he came to respect the therapist as being forthright and not easily intimidated.
Although Jules's self-esteem needed to be augmented as a result of his being placed in the role of patient, the therapist needed to maintain his authoritative therapeutic posture. Jules easily restored his self-confidence by brief visitations to his accomplishments, a process that took no more than a session or two. It was more important, however, to work with Jules to instill a sense of empathy for others through focused exploration of how he imagined their experience, and to understand and accept the ‘unspoken contract’ of restraint and responsibility in society. This measure, aimed at preventing recurrences, required that no deceptions were made by Jules, and that his compliance was sincere.
Barbara was a 27-year-old bartender who enjoyed her line of work, as it was quite agreeable with her lifestyle. There was a component of tending bar in a nightclub that allowed her to ‘perform,’ she explained, thereby garnering much attention and attracting multiple sexual partners. She seemed quite proud of this social life and conquests, as she spoke of her previous night's ‘hook-up.’ Although the majority of her experience had been with very short-term partners, she was actually once married. She described this relationship in very nonchalant terms, seeming to bestow no more importance to the arc of this 6-month relationship than to a particular afternoon's activities. When questioned regarding the ending of the marriage, she faulted her spouse's jealousy, as she still drew the attention of many men at work. Although Barbara seemed relatively content in her presentation, and was vague in her reasoning for seeking therapy, she seemed to detect some personal inadequacy that could not be fulfilled by her exploits, or a vague tinge of guilt over some of her more dishonest manipulations.
The distinctive feature of Barbara, an amorous narcissist, was an erotic and seductive orientation, a building up of her self-worth by engaging members of the opposite gender in the game of sexual temptation. There was an indifferent conscience, an aloofness to truth and social responsibility that, if brought to her attention, elicited an attitude of nonchalant innocence. Though highly self-oriented, she was facile in the ways of social seduction, often feigned an air of dignity and confidence, and was rather skilled in deceiving others with her clever glibness. She was skillful in enticing, bewitching, and tantalizing the needy and the naive. Although indulging her hedonistic desires, as well as pursuing numerous beguiling objects at the same time, she was strongly disinclined to become involved in genuine intimacy. Rather than investing her efforts in one appealing person, she sought to acquire a coterie of amorous objects, invariably lying and swindling as she wove from one pathological relationship to another. The qualities just outlined are strongly suggestive of the observation that narcissistic personality types such as Barbara possess numerous characteristics that are primary among histrionic personalities, a fact clearly seen in her Millon Clinical Multiaxial Inventory scores.
Although a reasonably good capacity for sexual athletics sustains the vanity of many individuals, narcissists or not, the need to repeatedly demonstrate one's sexual prowess is a preeminent obsession among amorous subtypes. Among these personalities are those whose endless pursuit of sexual conquests is fulfilled as effectively and frequently as their bewitching style ‘promises.’ Others, however, talk well, place their lures and baits extremely well, that is, until they reach the bedroom door; maneuvering and seduction is done with great aplomb, but performance falls short. For the most part, the sexual exploits of the amorous narcissist are brief, lasting from one afternoon to only a few weeks.
Perhaps Barbara was actually fearful of the opposite sex, afraid that her pretensions and ambitions would be exposed and found wanting. Her sexual banter and seductive pursuits were merely empty maneuvers to overcome deeper feelings of inadequacy. Although she seemed to desire the affections of a warm and intimate relationship, when she found it (assuming her marriage appeared, at first, to provide these qualities), she undoubtedly felt restless and unsatisfied. Having won someone over, she probably needed to continue his pursuit. It is the act of exhibitionistically being seductive, and hence gaining in narcissistic stature, that compels. The achievement of ego gratification terminates for a moment, but it must be pursued again and again.
It was possible that Barbara left behind her a trail of outrageous acts such as swindling, sexual excesses, pathological lying, and fraud. Her disregard for truth and the talent for exploitation and deception was neither hostile nor malicious in intent. These characteristics appeared to derive from an attitude of narcissistic omnipotence and self-assurance, a feeling that the implicit rules of human relationships did not apply to her and that she was above the responsibilities of shared living. As with the basic narcissistic pattern, Barbara went out of her way to entice and inveigle the unwary among the opposite sex, remain coolly indifferent to the welfare of those whom she bewitched, whom she had used to enhance and indulge her hedonistic whims and erotic desires.
Caring little to shoulder genuine social responsibilities and unwilling to change her seductive ways, Barbara wouldn't ‘buckle down’ in a serious relationship and expend effort to prove her worth. Never having learned to control her fantasies or be concerned with matters of social integrity, Barbara maintained her bewitching ways, by deception, fraud, lying, and by charming others through craft and wit as necessary. Rather than applying her talents toward the goal of tangible achievements or genuine relationships, she devoted her energies to constructing intricate lies, to cleverly exploit others, and to slyly contrive ways to extract from others what she believed was her due. Untroubled by conscience and needing nourishment for her overinflated self-image, she fabricated stories that enhanced her worth and thereby succeeded in seducing others into supporting her excesses. Criticism and punishment were likely to prove of no avail as Barbara was likely to quickly dismiss these aspersions as products of jealous inferiors.
It was expected that Barbara would attempt to manipulate and monopolize the process of therapy, and would need to be engaged and controlled through a firm and focused attitude on the part of the therapist. Cognitive and interpersonal strategies would focus on altering her perpetuating belief of her own importance and the devaluation of (but reliance on) others, and would thereby serve to establish improved social skills and more genuine relationships. Concurrently, it would also be prudent to help Barbara assume a less passive affective stance (less nonchalant and superficial in her attitude). In addition to cognitively and interpersonally undermining Barbara's irresponsible attitudes and actions, behavioral interventions should be fruitful in reinforcing new habits and skills, as well as establishing responsible social actions. A group milieu might be a most beneficial adjunct, as well, in guiding Barbara towards reassessing her interpersonal style and self-important attitude, establishing empathy towards others, and taking on a more responsible disposition.
Cognitive reorientation seemed to be the most effective catalyst for Barbara to modify some of these attitudes about herself and her socially lamentable actions in a short-term milieu. As her more affable but trite veneer gave way to increasingly more meaningful exchanges with the therapist, Barbara was able to begin working on her erroneous assumptions regarding herself and her social context. Interpersonal methods also were employed to examine these assumptions and reevaluate some of her less acceptable actions. These focused interpersonal methods, most notably group therapy, helped her reassess herself more realistically and effectively, and provided a forum for her to experiment with more cooperative and sociable behaviors. For Barbara, the more expressive and longer-term techniques would not have been useful, as she was prone towards self-illusions too easily reinforced by the imaginative freedom these methods foster. Likewise, several other popular short-term techniques, including environmental management, psychopharmacologic treatment, and behavior modification would not be of value in effecting change.
In the early sessions, Barbara frequently attempted to dominate the therapeutic relationship, relying on her well-practiced and suave seductive tactics. This habit needed to be confronted, though delicately and honestly, as overemphasizing any shortcoming might have led to regression in establishing rapport. During this early stage, she navigated her way around any investigations into personal issues by using her ‘charm’ and jumping from one superficiality to the next, as well as casting responsibility for herself on to others. Unless dealt with directly, yet without disapproval on the part of the therapist, her evasiveness and unwillingness would have seriously interfered with short-term gains. Cognitive confrontations, which were firm but consistently honest, were effective in prompting her to examine critically her own beliefs and behaviors, avoid further attempts to win dominance, and to invest in the change process.
Cognitively based methods were effective at undermining faulty beliefs that prompted Barbara's tendency to devalue others. It was, at first, unfathomable to her that her assumptions were askew, as she had consistently assured herself that everyone else's views were inane. That is, she simply couldn't be wrong, as her modus operandi seemed to work well for her, yet so many others seemed to be discontent. She needed to understand the basic tenet that disparity between herself and those more sensitive (or perhaps, more accurately expressive) did not necessarily mean that her views were superior.
Generally, an illusion that calls for brief confrontive therapy with amorous narcissists is based on the fact that these patients are unlikely to seek therapy on their own. They typically believe that they will solve everything for themselves by simply being left alone. In Barbara's case where treatment was self-motivated, it may have followed an unadmitted humiliation or failure. Regardless of what her promptings were, seeking professional help harmed her pride. Though she gave lip service to accepting therapy, this attitude was rather tentative and delicate throughout the therapeutic relationship.
Although it was appropriate to help Barbara rebuild this guarded, deflated self-image, the therapist could not appear submissive lest Barbara revert rapidly to many of her older, problematic tactics. Rebuilding her self-confidence was a simple process, which merely involved indulging her in reminiscing about a few past conquests. An objective geared more at preventing recurrences was that of helping Barbara become more empathic with others, and to understand the effects of her behavior in social interactions.
We have attempted in this chapter to promote the view that there is not a ‘singular’ modality of therapy that is most indicated for a particular personality (in this case, the narcissistic personality). Rather, the therapeutic techniques that have evolved over the history of modern treatment modalities may all be useful, not in a ‘grab-bag’ way, but in a coherent, synergistic fashion that facilitates understanding and intervention for the multidimensional nature of the individual personality. We may learn considerably from the individual schools of thought and their evolution, and as astute clinicians, a thorough understanding of these modalities is requisite for effective therapy. We also make note that there is not one singular narcissistic personality that will easily match our preconceived notions from the DSM or psychopathology textbook. Rather, each is a unique individual, likely expressing one of several possible admixtures of personality characteristics, and a thorough understanding of the personality matrix may prove fruitful in gaining a fuller understanding of the precise presentation of that individual.