* The former name of the first author is Kelly Bemis.
The kindred disorders of anorexia nervosa and bulimia nervosa present a number of common problems to the psychotherapist. Both: (1) are organized around a characteristic set of beliefs about the importance of weight as an index of personal worth; (2) lead to stereotyped behaviors designed to manipulate food intake and energy expenditure; and (3) disrupt normal physiology, with predictable and sometimes profound effects on psychological and social functioning as well as physical health. The central ideas about eating and weight are often highly resistant to modification, especially in individuals with anorexia nervosa; at the same time, the physical consequences that result from the belief-consistent behaviors of undereating, overexercising, and purging require close attention and sometimes prompt intervention on the part of clinicians.
The distribution of these disorders is approximately parallel, and markedly skewed by sex, age, culture, and perhaps era. Females are disproportionately vulnerable to both conditions, with males seldom representing more than 5% of identified cases. (Because the great majority of individuals with anorexia nervosa and bulimia nervosa are female, feminine pronouns are used throughout the chapter to refer to individuals with these disorders.) Anorexia nervosa usually develops between the prepubertal period and the beginning of adulthood; onset for bulimia nervosa is slightly later, with symptoms commonly emerging in late adolescence through young adulthood. Prevalence rates are low for both disorders, with anorexia affecting up to 0.5% of young females and bulimia present in 1–2%. These conditions are rare in underdeveloped countries, often appearing for the first time during periods of rapid social change associated with exposure to Western culture.
Controversy persists regarding the nature and degree of the relationship between these conditions. The two symptom clusters often overlap concurrently or sequentially. Approximately half of low-weight anorexic patients also binge and/or purge, and substantial proportions cross diagnostic boundaries over the course of their disorder, most often from anorexia to bulimia. The picture is further obscured by the fact that many individuals develop persistent eating disturbances that share features with one or both of these disorders, but fail to match the specifications for either and are consigned to the residual category of ‘eating disorder not otherwise specified’ (ED-NOS). Some experts argue that the high percentage of unclassifiable cases, the frequent migration of patients across categories, the similarity of symptoms and distribution patterns, and the evidence of cross-transmission of familial risk suggest the operation of common mechanisms (Holmgren et al., 1983; Beumont et al., 1994; Palmer, 2000; Fairburn et al., 2003; Fairburn and Harrison, 2003). To better reflect this reality, Fairburn et al. (2003) have proposed a ‘transdiagnostic’ approach to conceptualizing and treating the eating disorders.
On the other hand, a number of features suggest meaningful distinctions between anorexia nervosa and bulimia nervosa. The disorders are differentially associated with a variety of background characteristics and personality features. In anorexic patients, low weight status dominates the presenting picture and early phases of intervention. Throughout therapy, the disorders are distinguished by the extent to which symptom resolution is desired, attempted, achieved, and maintained. Anorexic individuals are much less likely to seek treatment, to persevere in efforts to change, and to obtain benefit even if they remain engaged. One follow-up of 246 cases treated an average of 7.5 years earlier found that 74% of patients with bulimia nervosa achieved a full recovery at some point during the follow-up period, compared with 33% of those with anorexia nervosa (Herzog et al., 1999). A prospective naturalistic study of 220 eating-disordered individuals found similarly high rates of symptom remission for those diagnosed 5 years earlier with bulimia or ED-NOS, while a substantially greater proportion of anorexic participants retained eating disorder and/or other psychiatric symptoms (Ben-Tovim et al., 2001).
Another distinction that will be evident throughout this review is that the study of these disorders has followed markedly different developmental sequences. Although anorexia nervosa has been the subject of intensive investigation for more than half a century, only a handful of controlled studies of psychotherapy have been conducted. In contrast, treatment research was initiated soon after the designation of bulimia nervosa as a psychiatric disorder in 1980, and has continued to accumulate at an impressive rate.
In the next sections, we will outline three treatment modalities for bulimia nervosa [cognitive-behavioral therapy (CBT), interpersonal psychotherapy (IPT), and pharmacotherapy] and four for anorexia nervosa (family therapy, psychodynamic therapy, CBT, and pharmacotherapy). These were selected on the basis of their prominence in the field and degree of empirical support. Space limitations prevent a more exhaustive review of the full range of approaches proposed, including behavior therapy (BT; e.g., Rosen and Leitenberg, 1982, 1985), feminist therapy (e.g., Orbach, 1985; Fallon et al., 1994; Kearney-Cooke and Striegel-Moore, 1997), nonverbal expressive approaches such as art and movement therapy (e.g., Hornyak and Baker, 1989; Maclagan, 1998), narrative therapy (e.g., Madigan and Goldner, 1999), and solution-focused therapy (e.g., McFarland, 1995). We omit a number of these with regret; however, on balance it seems preferable to include more detailed information about several approaches than to offer thumbnail sketches of all.
The central feature of bulimia nervosa is the presence of recurrent episodes of binge eating, defined as uncontrolled consumption of objectively large amounts of food, accompanied by compensatory behaviors intended to prevent weight gain (American Psychiatric Association, 2000). Compensatory methods include self-induced vomiting, laxatives, diuretics, enemas, fasting, and excessive exercise. Bulimia nervosa is subdivided into purging and nonpurging types on the basis of the strategies employed. Initially, individuals with this disorder may not view their behavior as problematic, in that the advantage of being able to eat freely without gaining weight overshadows concern about the negative ramifications of binge eating and purging. Over time, this perspective is likely to change, as episodes become more frequent and adverse consequences begin to accumulate.
As the following case examples illustrate, bulimia nervosa varies widely in severity and can occur in patients with vastly different levels of global adjustment. For some individuals, the pattern is experienced as an isolated symptom cluster in the context of relatively successful overall functioning; in other cases, life is dominated by the disorder and additional severe psychiatric problems may be present.
Sharon is a 24-year-old graphics designer with a 5-year history of bulimia nervosa. She started dieting and exercising rigorously after gaining 12 pounds during her first year in college. Although these efforts initially resulted in the desired weight loss, her success began to erode as she developed a pattern of eating larger and larger quantities of food late at night. After reading a personal account of bulimia in connection with a psychology course, Sharon experimented with self-induced vomiting. At first the act was difficult and painful, and she attempted it only when extremely distressed by the amount she had eaten. Over time, she found the reflex easier to elicit, and binge–purge episodes increased in frequency to their present level of three to five times per week. Although Sharon sought counseling for stress and mild depression while in college, she did not disclose her disordered eating behavior to her therapist. Sharon is now motivated to seek professional help for her bulimia because she plans to move in with her fiancé and fears that she will be unable to conceal her pattern once they are living together.
Emily is a 38-year-old woman with severe, unremitting bulimia nervosa dating back to mid-adolescence. It is probable that Emily briefly met criteria for anorexia when she was 15; however, she received no treatment for her eating disorder at that time, and soon shifted into a pattern of bulimic behavior. She has been hospitalized twice for treatment of her bulimia, excessive drinking, self-injury, and suicidal ideation. At present, her life is dominated by nearly continuous cycles of binge eating and purging, with vomiting induced five to 10 times daily. Emily is separated from her abusive husband and estranged from her divorced parents and two sisters. She is currently subsisting on disability payments and occasional temporary work as a data entry clerk. Emily has seen several therapists on an outpatient basis, but frequently fails to attend scheduled sessions and has never remained engaged in treatment for more than several months. Her present weight is at the low end of the normal range, and she is reluctant to gain for fear of becoming overweight, as she was during childhood and early adolescence; however, she believes that the principal determinant of her bulimic behavior is the need to blunt the pain of her empty existence.
Fairburn's cognitive-behavioral model of bulimia nervosa proposes that the disorder arises from excessive reliance on weight and shape as bases for self-evaluation (Fairburn, 1981, 1997a; Fairburn et al., 1986, 1993b). Extreme concerns about the size and shape of the body, in combination with low self-esteem, lead to increasingly determined attempts to limit the quantity and type of foods consumed. These persistent efforts create physiological and psychological vulnerability to episodes of binge eating. Individuals try to undo these lapses in restraint by vomiting, taking laxatives, and imposing still more stringent exercise regimens and dietary rules; however, resort to these behaviors reinforces the bulimic cycle by triggering distress, diminishing self-esteem, renewing concern about weight and shape, and increasing deprivation. CBT is designed to address each of the principal elements in the model.
Support for the cognitive-behavioral analysis of bulimia nervosa comes from a number of sources, including risk factor research, correlational studies, and some experimental investigations (Vitousek, 1996; Cooper, 1997; Fairburn, 1997a; Byrne and McLean, 2002; Fairburn et al., 2003). In addition, patterns of treatment response are consistent with this model of symptom maintenance. Across therapeutic modalities, the reduction of dietary restraint mediates decreases in bingeing and purging (Wilson et al., 2002). The central role assigned to cognitive factors is affirmed by two findings: dismantled versions of CBT that retain its behavioral components but omit direct work on beliefs are less effective than the full treatment package (Fairburn et al., 1991, 1993a; Thackwray et al., 1993; Cooper and Steere, 1995), and the persistence of distorted attitudes at posttreatment predicts relapse (Fairburn et al., 1993a).
The standard intervention is a structured, manual-based approach that includes 19 individual sessions spanning 5 months (Fairburn et al., 1993b; Wilson et al., 1997). Treatment is divided into three stages, which are characterized by distinct therapeutic goals.
The first phase begins by establishing a therapeutic relationship and presenting the CBT model and treatment rationale. The clinician emphasizes that therapy will address all facets of the eating disorder, with particular stress in the beginning on the importance of reducing dietary restraint. Many individuals with bulimia nervosa hope that therapy will help them excise the unwanted behaviors of bingeing and purging so that they can diet more effectively and achieve a lower preferred weight. The message delivered at the inception of CBT contains both good news and bad news from these patients’ perspective. They have not become trapped in their current pattern of behavior because they are greedy or crazy or lack self-control, but because they are attempting to impose unreasonable and counterproductive standards of dietary restraint. Overeating is the normal response to food deprivation in humans and animals alike; indeed, it should not be construed as ‘overeating’ at all, but as a lawful reaction to conditions of deficit or irregular supply. The unwelcome corollary is that the two goals of eliminating bulimic behavior and achieving a higher level of dietary restraint are incompatible. In order to gain freedom from binge-eating, bulimic individuals must adopt a pattern of regular eating.
Accordingly, the intervention begins with a strong emphasis on consuming (and retaining) the regular, spaced meals and snacks that reduce susceptibility to bulimic episodes. A number of behavioral techniques are introduced during the first stage, including self-monitoring and the scheduling of alternative activities to replace binge-eating and purging (see section on Attention to eating and weight). Patients are also provided with psychoeducational material about dietary restraint, nutrition, weight regulation, and the consequences of bulimia. Some of this information is intended to correct erroneous beliefs about specific bulimic behaviors. For example, laxative abuse is usually based on the assumption that cathartics prevent weight gain by shooting food so rapidly through the intestinal tract that calories cannot be absorbed. In fact, even massive doses of laxatives eliminate only a small fraction of the calories consumed during binges (Bo-Linn et al., 1983). Other psychoeducational material is helpful in underscoring the CBT model or decreasing concern about the consequences of giving up bulimic behavior. For example, while most patients fear that the lessening of dietary restraint will cause substantial weight gain, the evidence shows that the great majority of patients gain little or no weight after a successful course of CBT (Fairburn, 1993, 1995; Fairburn et al., 1993a).
In the second stage, the emphasis on regular eating patterns continues; in addition, patients are asked to start reintroducing excluded foods into their diets and to resume eating in settings (such as restaurants) and social situations that they may have been avoiding. Cognitive restructuring techniques are used to analyze thinking patterns that help sustain symptoms, including dichotomous judgments about eating, weight, and personal performance. Patients are encouraged to review the evidence for and against their beliefs in order to reach reasoned conclusions that can be used to guide their behavior.
The final stage focuses on relapse prevention strategies. The patient reviews the tactics that she has found especially helpful during treatment, anticipates high-risk situations, and outlines an individualized ‘maintenance plan.’
Consistent with general CBT principles, therapists combine a directive, problem-solving focus with a collaborative style throughout therapy. Clients must take an active role in achieving symptom control through collecting data, generating solutions, and practicing new behaviors. An important goal is for patients to develop the skills and self-confidence that allow them to ‘become their own therapists’ during and after the time-limited course of CBT (Wilson et al., 1997).
The empirical examination of CBT for bulimia nervosa has followed a thoughtful and systematic sequence of investigation. The approach was developed through clinical experimentation with some of the first bulimic cases reported in the literature, and was guided by a clear, concise model of symptom maintenance. It was translated into a manualized intervention and tested in more than 25 controlled trials in a variety of settings against a number of well-chosen alternative modalities. Within 15 years of the time the approach was proposed (Fairburn, 1981), research had begun to examine therapeutic mechanisms, combined and sequential treatment approaches, generality of effects across different patient populations and providers, and dissemination strategies. On the basis of this impressive body of evidence, CBT has earned the status of treatment of choice for bulimia nervosa (Wilson, 1996; Agras, 1997; Compas et al., 1998; Wilson and Fairburn, 1998; American Psychiatric Association, 2000; Cochrane Depression Anxiety and Neurosis Group, 2000; Fairburn and Harrison, 2003).
In the reduction of both core and associated symptoms, CBT is clearly superior to wait-list control conditions, and matches or exceeds all other examined psychological interventions, including psychodynamic therapy, supportive treatment, IPT, BT, stress management, exposure and response prevention, and nutritional counseling. Reviews indicate that CBT results in mean reductions of 73–93% for binge eating and 77–94% for purging; total remission of symptoms is attained by one-third to one-half of CBT-treated patients when results are analyzed on an intent-to-treat basis (Craighead and Agras, 1991; Wilson et al., 1997; Wilson and Fairburn, 1998; Fairburn and Harrison, 2003; Thompson-Brenner et al., 2003). Consistent with the theoretical model that informs the treatment approach, CBT has also been shown to reduce dietary restraint, decrease depression, enhance self-esteem, and produce positive changes on global measures of adjustment and social functioning (Fairburn et al., 1991; Garner et al., 1993; Wilson et al., 1997; Wilson and Fairburn, 1998).
One clear advantage is that CBT works quickly in comparison with other psychotherapies (Wilson and Fairburn, 1998). For example, Wilson et al. (1999) determined that CBT had already produced most of the improvement evident at posttest by the third week of treatment. The rapid gains associated with CBT are also enduring. Reductions in binge eating and purging are characteristically maintained at 6–12-month follow-up assessments (Wilson et al., 1997). In the longest follow-up reported to date, 71% of the participants who had achieved full symptom remission by the end of the active treatment period remained symptom-free an average of 5.8 years later (Fairburn et al., 1995).
Although the positive effects of CBT are robust and stable, it is also well-established that no more than 50% of patients recover completely, while a substantial minority obtain minimal symptom relief from participation in this mode of therapy. Across studies, the half or more of patients who do not attain full recovery through CBT continue to binge an average of 2.6 times per week and to purge 3.3 times per week at treatment termination (Thompson-Brenner et al., 2003). Little is known about the factors that influence response to CBT, as the few variables that appear to be associated with outcome in individual studies are seldom replicated across them (Wilson and Fairburn, 1998). The most consistent predictors of poor response are comorbid personality disorder and high baseline frequency of bingeing and purging. In addition, the strong relationship between symptom reduction during the first few weeks of CBT and eventual outcome provides some rational basis for continuing the standard approach or considering modified, supplementary, or alternative interventions (Wilson et al., 1999; Agras et al., 2000). Unfortunately, there is scant empirical basis for anticipating that patients who fail to respond to CBT will derive greater benefit from a different treatment approach (Wilson et al., 2000).
Clinical lore holds that CBT is appropriate only for relatively ‘simple’ cases of bulimia nervosa such as that represented by Sharon, but contraindicated for complex, severe, and/or comorbid symptom pictures, exemplified by the description of Emily. Certainly, Sharon is far more likely than Emily to be symptom-free after 19 sessions of CBT; however, it is a fallacy to conclude that CBT is therefore the wrong treatment for a patient with Emily's symptom profile. Such reasoning holds only if an alternative approach is known to support superior outcomes in comparable patients (Hollon and Kriss, 1984; Wilson, 1995, 1996). No such evidence exists in the treatment of bulimia. A reasonable course for Emily's case might be clinical experimentation with modifying CBT by increasing its intensity and/or duration, and by including additional components to address difficulties with affect regulation (e.g., Segal et al., 2002), self-harm (e.g., Linehan, 1993), and substance abuse (e.g., A. T. Beck et al., 2001; Parks et al., 2001) (see discussions in Wilson, 1996; Wilson et al., 1997 and Fairburn et al., 2003).
More generally, commentators from both within and outside the CBT orientation have suggested that modifications to the basic approach might provide greater benefit to a broader range of patients. Critiques of CBT for bulimia nervosa usually highlight three overlapping limitations. First, the standard intervention is narrowly focused on specific eating disorder symptoms, paying minimal attention to interpersonal issues or generic concerns about self-worth (Hollon and Beck, 1994; Vitousek, 1996; Garner et al., 1997). CBT for other disorders characteristically extends to a wider range of topics as relevant to individual cases, and there is no obvious clinical justification for restricting the scope of CBT for bulimic patients. Second, the manual-based approach relies predominantly on behavioral tactics, with fairly cursory attention paid to the exploration of beliefs and less to the role of affect (Hollon and Beck, 1994; Meyer et al., 1998; Ainsworth et al., 2002). A third and related concern is that CBT appears less effective in reducing patients’ focus on weight and shape than in eliminating the behavioral symptoms of bingeing and purging (Wilson, 1999). Greater change might be obtained through more emphasis on cognitive work; in addition, closer focus on body image issues through therapist-assisted exposure and other targeted CBT techniques could be beneficial (Tuschen and Bent, 1995; Rosen, 1996; Fairburn, 1997a; Wilson et al., 1997; Wilson, 1999; Fairburn et al., 2003).
On the basis of these observations, Fairburn et al. (2003) recently proposed a revised model of the maintenance of bulimia nervosa and outlined a broader approach to its treatment. The new formulation is intended to supplement rather than replace the original model, principally through the inclusion of four additional foci, if indicated for individual patients: perfectionism, low self-esteem, mood intolerance, and interpersonal difficulties.
If the standard course of manual-based CBT is not sufficient for all patients, the full treatment may be unnecessary for some (Wilson, 1995; Wilson et al., 1997). The pressures of cost containment and the scarcity of trained specialists have stimulated efforts to find economical, readily disseminable treatments for bulimic patients. Several streamlined interventions consistent with the CBT approach have been evaluated. One of these involves self-help manuals (Schmidt and Treasure, 1993; Cooper, 1995; Fairburn, 1995) designed for direct use by bulimic individuals with or without guidance by a professional or paraprofessional (Fairburn and Carter, 1997; Birchall and Palmer, 2002; Carter, 2002). Another possibility is an abbreviated CBT intervention that can be applied in primary care settings (Waller et al., 1996). Additional alternatives are group CBT that includes all components of the standard model but can be delivered economically to multiple patients (Agras, 2003; Chen et al., 2003) or a shorter group series that presents the psychoeducational content covered in the full approach (Olmsted and Kaplan, 1995).
Each of these approaches has been examined, and the same general conclusion appears to apply across all: truncated and/or group-administered variants of CBT provide substantial benefit to a subgroup of patients, but typically yield lower rates of improvement and remission than the complete individual approach (e.g., Olmsted et al., 1991; Treasure et al., 1994, 1996; Thiels et al., 1998; Mitchell et al., 2001; Palmer et al., 2002; Chen et al., 2003). The appropriate use of self-help and/or group psychoeducation may be as initial interventions in a stepped-care model, with individuals who fail to respond offered a subsequent course of the full treatment; conclusions about brief CBT and a group version of standard CBT are more tentative pending the accumulation of additional data.
In contrast to CBT, the use of IPT in the treatment of bulimia nervosa is not predicated on an elegant, disorder-specific model of symptom maintenance. The approach was first applied to this population because it suited the purposes of clinical researchers who needed a short-term, well-specified modality that had minimal conceptual or procedural overlap with CBT. IPT fulfilled these specifications admirably, and was initially selected for comparison with CBT and BT in a trial conducted by Fairburn et al. (1991).
Although IPT was in some senses chosen as a foil, it would be unjust to both the researchers and IPT itself to assume that it was meant to be a ‘straw treatment’ that would make the results of CBT appear more impressive by contrast. IPT was already established as an effective therapy for depressed outpatients (Weissman et al., 1979; Elkin et al., 1989), and would have been a poor bet for investigators seeking an attention-placebo condition. Moreover, if there is no elaborated ‘interpersonal theory’ of bulimia nervosa, there is substantial evidence that interpersonal issues are implicated in the disorder. Family problems, sensitivity to criticism, conflict avoidance, and concern about social presentation are all prominent in bulimic patients, and binge episodes are often precipitated by interpersonal stress. Therefore, IPT offered a credible alternative treatment that was manual based and approximately matched to CBT in format, yet focused on different issues, employed different techniques, and presumably worked through different mechanisms.
In its original formulation for depressed patients, IPT was also designed as a ‘research treatment’ that gave structure to the emphasis many clinicians place on their clients’ relationships (Klerman et al., 1984). Drawing on Sullivan's (1953) interpersonal approach, IPT makes few assumptions about the variables that produce specific symptom patterns. The rationale for its use across diagnostic categories and clients is that all psychiatric disorders develop and persist in a social context, and are often ameliorated by resolving interpersonal problems. IPT focuses on patients’ current social relationships rather than attempting to address childhood issues or enduring personality characteristics (Weissman and Markowitz, 1994).
The adaptation of IPT for bulimia is outlined in several descriptive articles (Fairburn, 1993, 1997b, 2002b; Apple, 1999; Wilfley et al., 2003). Therapy is delivered in 19 sessions over 18–20 weeks, scheduled twice weekly in the first month, weekly for the subsequent 2 months, then in alternate weeks. This represents a slight reduction and rearrangement of the sessions specified for work with depressed patients, in order to align the format more precisely with CBT and BT. With a few exceptions, the intervention for bulimia is otherwise identical to the approach detailed in the IPT manual for depression (Klerman et al., 1984; Weissman et al., 2000). Two changes in content are prescribed: the initial sessions involve an analysis of the chronology and context of eating disorder symptoms; thereafter, discussion of disorder-specific material is actively discouraged to maintain the focus on interpersonal issues. The first of these modifications is entirely consistent with the principles of IPT for depression; however, the second represents a departure that was intended to sharpen the distinction between IPT and CBT/BT (Palmer, 2000). In other applications, IPT does not exclude direct work on current symptoms. As reformulated for bulimia, IPT avoids any reference to eating patterns, compensatory behaviors, and weight concern between the first and last few sessions of the treatment course. If these topics are raised by patients, therapists are instructed to try to ‘limit patients’ discussion of their disordered eating behaviors to 10 seconds or less’ (Apple, 1999, p. 717).
The first phase of IPT is completed in three or four sessions, which are devoted to a thorough assessment of the interpersonal context surrounding bulimic symptoms. Therapist and patient trace the historical association between significant events, relationships, mood, self-esteem, and changes in eating patterns and weight. This review is used to create a ‘life chart’ that illustrates the connection between experiences and symptoms. The assessment also includes identification of interpersonal triggers for episodes of binge-eating (Fairburn, 2002b).
On the basis of the information collected and organized during this initial phase, therapist and patient identify one or more problem areas that will become the focus of the next stage of treatment. Paralleling IPT for depression, these are drawn from four categories: grief reactions, interpersonal role disputes, difficulties arising from role transitions (such as moving out of the parental home or starting work), and interpersonal deficits. For bulimic patients, the most common targets are role disputes (relevant for 64% of clients) and role transitions (identified in 36%); issues related to grief (12%) or interpersonal deficits (16%) are less often implicated for this population (Fairburn, 1997b).
With reference to the case examples outlined earlier, a natural focus of IPT for Sharon might be her impending transition from living alone to forming a new household with her fiancé. In view of Emily's profound social isolation, therapy might focus on her interpersonal deficits or unresolved issues in her conflicted relationships with her estranged husband and family. Unfortunately, just as the standard CBT intervention may not be effective in Emily's case, patients presenting with longstanding interpersonal deficits are difficult to help through IPT as well (Fairburn, 1997b).
In the final phase of treatment, the patient and therapist review progress to date, discuss remaining difficulties, and anticipate and plan for possible future problems. At this point, patients are encouraged to identify any changes in eating-disordered symptoms over the course of therapy, and to note their linkage to improvements in relationship patterns (Apple, 1999).
In the study that prompted the adaptation of IPT for bulimia nervosa, the approach appeared moderately effective when status was assessed at the end of the treatment period (Fairburn et al., 1991). IPT and CBT were associated with comparable reductions in binge frequency and depression, as well as equivalent improvements in social functioning; however, CBT was more effective than IPT (or BT) in modifying attitudes about weight and shape, and produced greater reductions in dietary restraint and vomiting frequency. Data collected after a 1-year closed follow-up period revealed some surprising trends (Fairburn et al., 1993a). While participants in the BT condition were doing quite poorly, those who had received IPT had caught up to the CBT-treated patients so that the groups had become statistically indistinguishable across all indices of outcome. A similar pattern of results was obtained in a subsequent multisite study (Agras et al., 2000). CBT again outperformed IPT at posttreatment assessment; once more, no differences were discernible by follow-up as a function of continuing improvement in participants previously treated with IPT.
The unanticipated efficacy of IPT at follow-up seemed to raise important questions for models of bulimia nervosa. Clearly, some individuals were able to accomplish significant (if slightly delayed) changes in their eating-disordered behavior even when therapy paid little or no attention to the specific symptoms that prompted them to seek treatment. The different temporal pattern of change also supported the view that these modalities worked through alternative mechanisms. Fairburn speculated that IPT might facilitate change by increasing patients’ feelings of self-worth, indirectly lessening their tendency to evaluate themselves on the basis of body shape and weight (Fairburn, 1988, 1997b; Fairburn et al., 1991). This hypothesis appeared consistent with the lag between the active treatment phase and the achievement of symptom control—perhaps it simply took more time for individuals to translate improvements in self-esteem into modifications of their eating behavior.
The intriguing intimation of a delayed treatment response or ‘sleeper effect,’ however, was disconfirmed by further analyses of data from the second study (Wilson et al., 2002). In fact, the same proportion of patients who remained symptomatic after IPT or CBT continued to improve during the follow-up period; thus, IPT appeared to ‘catch up’ to CBT simply because there were more symptomatic patients left at the end of IPT who were still eligible for a late shift toward recovery. The conjecture that the two treatments work through different mechanisms was contradicted as well. The mediators believed to account for improvement in IPT—improved self-esteem and interpersonal functioning—showed no relationship to symptom changes in either IPT or CBT. Instead, both treatments decreased bingeing and purging through reductions in dietary restraint, with CBT appearing more effective than IPT at posttest because it accomplished this objective more rapidly.
Although it remains unclear how IPT works, the equivalence of IPT and CBT by follow-up supports the conclusion that these modalities are comparably effective (Fairburn, 1993). On that basis, either treatment is a defensible first-choice alternative for bulimia nervosa, with the selection between them influenced by patient and therapist preference, availability of expertise, and the importance of prompt symptom control. Another possibility is that IPT might be reserved as a second-line treatment for patients who do not achieve satisfactory results through CBT. The sole study that has investigated the merits of such sequential treatment, however, was not supportive (Mitchell et al., 2002).
An eclectic assortment of drugs has been proposed and tested for the treatment of bulimia nervosa, often on the basis of short-lived theories about the nature of the disorder. It was reasoned variously that opiate antagonists might work if patients are ‘addicted’ to bulimic behavior, anticonvulsants if their ‘trance-like’ state during binges reflects seizure activity, and appetite suppressants if they are responding to faulty signals of hunger and satiety. Whatever the merits of these models, the medications they recommended proved unhelpful. Only one group of agents, the antidepressant drugs, outlasted the abandoned model that first suggested its use. Although the view that bulimia nervosa represents a variant form of affective disorder (Pope and Hudson, 1984) is no longer tenable, antidepressants make a moderate contribution to its treatment.
Most classes of antidepressant medication have been examined, including tricyclics, monoamine oxidase inhibitors, SSRIs, and atypical antidepressants (Walsh, 2002a). In virtually all trials, these medications have been superior to placebo, yielding consistent and approximately equivalent reductions in symptom frequency and associated features (for reviews, see Craighead and Agras, 1991; Mitchell and de Zwaan, 1993; Compas et al., 1998; Mayer and Walsh, 1998; Wilson and Fairburn, 1998; Peterson and Mitchell, 1999; Walsh, 2002a). In the short-term, binge–purge episodes are reduced by an average of approximately 60% and suppressed completely in about one-third of patients (Compas et al., 1998; Wilson and Fairburn, 1998); however, relapse rates appear to be substantial if drugs are administered on a long-term basis, and astronomical if they are discontinued (Pope et al., 1985; Pyle et al., 1990; Walsh et al., 1991). Although all tested antidepressants offer comparable benefits, fluoxetine is generally favored for its low side-effect profile (Wilson and Fairburn, 1998; Walsh, 2002a).
Interestingly, it has been established that antidepressants do not decrease bulimic behavior through the alleviation of depressed mood. Neither the presence nor the severity of mood disturbance predicts response to medication, and positive effects on bingeing and purging often precede changes in depressive symptoms (Johnson et al., 1996; Walsh, 2002a). Moreover, higher doses of fluoxetine (60 mg/day) are required for the control of bulimic behavior than the levels typically indicated (20 mg/day) for the management of depression (Fluoxetine Bulimia Nervosa Collaborative Study Group, 1992).
Direct comparisons of antidepressants and CBT consistently favor the latter. A meta-analysis indicated that CBT is significantly more effective in reducing binge–purge frequency, modifying attitudes toward shape and weight, and decreasing depression (Whittal et al., 1999). CBT is also associated with lower rates of attrition, greater reduction of dietary restraint, and better preservation of treatment gains. Only one investigation has suggested modest incremental benefit for simultaneous treatment with CBT and antidepressants (Walsh et al., 1997). Leading researchers in pharmacotherapy for eating disorders conclude that in most cases antidepressants should be used as a second-line treatment for patients who fail to respond to an adequate trial of CBT (Mitchell et al., 2001; Walsh, 2002a). The only two studies that have examined the use of medication as a follow-up treatment reached differing conclusions about its incremental advantage (Walsh et al., 2000; Mitchell et al., 2002).
Anorexia nervosa is defined by the assiduous pursuit of thinness through dietary restriction and other weight-control measures, resulting in a body mass index (BMI) substantially below the normal range. As patients’ weights decline, their fear of gaining weight paradoxically increases, so that the prospect of going from 89 to 90 pounds may seem almost as intolerable as reaching 150 pounds. Their attitudes toward their current dimensions are complex. On the one hand, many describe feeling overweight even while emaciated; simultaneously, most take pride in their exemplary thinness and may be offended if it is not recognized by others (Bruch, 1978; Vitousek, 2005). The cardinal features of the disorder are ego-syntonic—indeed, they are often fiercely and assertively so. Low weight and restrictive eating are not merely accepted as consistent with the ‘real self,’ but valued as accomplishments of the ‘best self.’ Many patients keep this dynamic to themselves; those who discuss it use striking imagery to describe the appeal of semistarvation:
When I eventually weighed under 80 pounds and looked at myself in the mirror… I saw someone beautiful: I saw myself…. The clearer the outline of my skeleton became, the more I felt my true self to be emerging…. I was, literally and metaphorically, in perfect shape… I was so superior that I considered myself to be virtually beyond criticism.
For me—this is really sick—it's like winning the Nobel Prize or something. It's like you get a kingdom or become a goddess… I felt it was to be someone, like I was becoming a unique person, creating my own identity. You feel that you are nobody before, and when you starve, you're getting yourself down to the bones: ‘This is really me. This is what I am.’
The ego-syntonic quality of symptoms seems to account for much of the variance in explaining why anorexia nervosa is so distinctively difficult to treat. In most disorders, lack of motivation is considered a ‘special problem’ in psychotherapy. In anorexia nervosa, however, attachment to symptoms and reluctance to change are not special problems but expected features that affect almost every aspect of treatment with virtually all patients. Without some understanding of this central issue, it is difficult to appreciate why controlled trials of psychotherapy are so rare, attrition rates so high, and results so unsatisfactory. Awareness of the phenomenon also provides essential context for the treatment modalities outlined below, illuminating why family therapy favors external control by parents, why dynamic therapy is usually supplemented with symptom-focused treatment, why CBT expects little attitude change from cognitive restructuring techniques, and why pharmacotherapy has failed to identify any medications (at least to date) that influence the core psychopathology of this disorder.
The achievement of restraint and thinness, however, comes at substantial cost. Patients are haunted by anxiety about the risk of losing control and increasingly constrained by self-imposed rules about what, when, where, and how to eat. These distressing concerns are accompanied by other characteristic symptoms, including depression, irritability, social withdrawal, and sexual disinterest, as well as a host of major and minor physiological disturbances. Most of these symptoms are secondary to semistarvation; all are exacerbated by undereating and weight loss. The pattern that most consistently precedes anorexia nervosa and survives its resolution is a cluster of obsessional and perfectionistic traits (Vitousek and Manke, 1994; Fairburn et al., 1999a; Serpell et al., 2002; Shafran et al., 2002; Anderluh et al., 2003). There is evidence that these features have a genetic basis (Lilenfeld et al., 1998), and some experts believe that they help to account for both the appeal of a narrowed focus on weight control and the capacity to persevere in the demanding routines required.
Data on the course of anorexia nervosa indicate that it can be a persistent, disabling, and sometimes lethal condition. Rapid weight gain can be accomplished in the hospital through operant programs or skilled nursing care, without resort to nasogastric feeding; however, patients often begin losing weight immediately after discharge. When outcomes are averaged across follow-up studies of varying lengths, it is typically reported that somewhat fewer than half of anorexic patients have recovered, while a third are improved but still manifest significant eating disorder symptoms and a fourth remain severely ill or have died of the disorder (Pike, 1998; Steinhausen, 2002; Sullivan, 2002).
These aggregate statistics, however, obscure considerable heterogeneity in the odds for recovery in the individual case (Fairburn and Harrison, 2003). One variable that contributes to the prediction of outcome in anorexia (but less consistently in bulimia) is the duration of illness at intake (Steinhausen, 2002; Keel et al., 2003). In some young patients with a short symptom history, the disorder appears to be either self-limiting or responsive to brief, low-intensity interventions; after the disorder is well-established, it is often highly resistant to change efforts (Wilson and Fairburn, 1998; Fairburn and Harrison, 2003). Comparisons of outcome figures across treatment trials are uninformative without reference to the age and duration of illness of the samples treated—even if the current severity of symptoms appears approximately equivalent, as in the two cases outlined below.
Chloe is a 16-year-old high school sophomore who began dieting after her track coach suggested that her performance might be enhanced if she lost 5 or 10 pounds. She immediately reduced her food intake during the day to a single carton of yogurt and an apple, and did her best to avoid eating ‘fattening’ foods during family dinners. In addition to her track practice, she also began running for an hour each morning before school and doing calisthenics in her room at night. Within several months, she had lost 20 pounds. Chloe was elated by her weight loss (as well as her improved race times), and felt confused and angry when her coach suspended her from the team and contacted her parents after she fainted during practice. On the advice of the family physician, Chloe was initially seen by a counselor who worked with adolescent (but rarely eating-disordered) clients. When Chloe's weight continued to decline, her physician prescribed an antidepressant and referred her to a dietitian for nutritional counseling, to no apparent effect. At that point, she was briefly hospitalized on a pediatric unit for medical stabilization and an attempt at weight restoration. By the time her increasingly desperate parents brought Chloe (figuratively kicking and screaming) to a specialty eating disorder program, she had reached a BMI of 14.5, just over 1 year after the onset of her anorexia nervosa.
Amanda is a 29-year-old English instructor in a community college who has a long history of restricting anorexia nervosa. She was hospitalized for 6 months when she was 20, but lost weight soon after discharge. Amanda maintained a BMI between 15 and 17 for the remainder of her years in college and graduate school. She was in therapy on and off during this period, but studiously avoided any form of treatment in which she would be expected to gain weight. At present, Amanda follows a highly restrictive vegetarian diet, and exercises 2 hours per day. Her life centers around her disorder and her teaching. She lives alone but remains close to her parents, who are resigned to their inability to affect her eating behavior. She has few social contacts outside of work, and rarely dates. After Amanda's weight recently drifted down an additional 7 pounds, her co-workers and physician began urging her to seek help.
Dominant schools of family therapy have taken a keen interest in anorexia nervosa and had considerable impact on the field (e.g., Minuchin et al., 1978; Selvini-Palazzoli, 1978; Dare, 1985; Dare and Eisler, 1992). Minuchin's structural model identified anorexia as the prototype ‘psychosomatic’ disorder, in which family dysfunction (including enmeshment, overprotectiveness, rigidity, and conflict avoidance) is expressed by the symptom-bearing child. The treatment approach featured ‘family lunch sessions,’ during which the therapist observed family dynamics and carried out on-the-spot interventions. Parents were urged to unite and force their anorexic child to eat—in some instances by holding her down and pushing food into her mouth with the therapist's encouragement and support. The method was widely publicized through the distribution of filmed sessions, which for a time were shown routinely in abnormal psychology classes throughout the United States. Many undergraduates found these disturbing to view—as did most eating disorder specialists. The results Minuchin claimed to have achieved, however, were every bit as dramatic as the sample sessions: nearly 90% of patients were said to be doing well at follow-up (Rosman et al., 1978). Critics have questioned the rigor, representativeness, and even the veracity of these data; many experts also dispute the assumption that family dynamics are uniform or causal in anorexia nervosa (e.g., Yager, 1982; Rakoff, 1983; Vandereycken, 1987).
The most influential contemporary form of family therapy for anorexia nervosa is the ‘Maudsley model,’ which combines elements from both structural and strategic approaches (Dare and Eisler, 1995, 1997; Lock et al., 2001). Following Minuchin, therapists direct parents to assume control over the anorexic child's eating behavior and orchestrate crises during meal sessions to empower them in this role. The Maudsley approach is more closely aligned with strategic family therapy, however, in favoring an ‘agnostic’ view of etiology. Family members are charged with responsibility for the anorexic individual's recovery, but explicitly exonerated from blame for her disorder.
As applied to adolescent patients, the Maudsley approach involves 10–20 family sessions spaced over 6–12 months. The ‘conjoint’ format specifies that all family members—siblings as well as parents and the anorexic child—should be seen together. A recently published manual (Lock et al., 2001) describes the implementation of conjoint family therapy (CFT) in detail. As discussed below, a form of ‘separated’ family therapy has also been devised and tested.
CFT is divided into three phases, with transition from one to the next dependent on the achievement of specific objectives. The approach is highly structured—indeed, almost scripted, particularly in the early sessions. The key therapeutic maneuver in Phase I is to reestablish parental authority in the family system, with particular reference to asserting control over the anorexic child's eating and weight. Several tactics are adopted to further this goal. Using a sympathetic but authoritative style, the therapist works to heighten the parents’ level of anxiety by underscoring the severity of their daughter's condition. In an ‘almost ritualistic’ fashion (Lask, 1992), clinicians are advised to assume a ‘portentous, brooding, and grave manner’ (Lock et al., 2001, p. 208) when they greet parents; in the first session, they should ‘concentrate on the horror of this life-threatening illness,’ (p. 52) warning parents that ‘something very drastic has to happen for you to save [your child's] life’ (p. 47).
Another recommended technique is the externalization of anorexic symptoms. The disorder is construed as an alien force that has overtaken the patient so completely that she is incapable of controlling her own behavior—and therefore critically in need of her parents’ forceful intervention. This ‘benevolent dissociation’ is intended to assuage parents’ guilt about using strong measures to combat the illness, as well as to convey support for the patient as an individual distinct from her disorder (Lock et al., 2001; Russell, 2001).
Parents are asked to bring food to the second treatment session, and coached by the therapist to find ways of compelling their daughter to eat. Outside of therapy, they are advised to keep her under parental supervision 24 hours a day during the first few weeks, temporarily arranging leaves of absence from school and work to accomplish the task of refeeding. External control tactics are also applied to other eating-disordered behaviors; for example, parents are told to lock the refrigerator and cupboard doors if necessary to prevent binge-eating, and to inform neighborhood pharmacies that their daughter must not be allowed to purchase laxatives.
Phase II begins when the patient is surrendering relatively consistently to the demand to increase her intake and weight, typically after 3–5 months of weekly family sessions (Lock et al., 2001). During this stage, the therapist encourages a gradual fading of close supervision and reinforces the patient's return to age-appropriate activities and levels of autonomy. The message is that anorexia nervosa deprived her of the right to make her own choices, as she had functionally regressed to a child-like incompetence and dependency; now that she is beginning to improve, she is entitled to reclaim more control over her life in this and other domains. Parents are asked to focus their attention on strengthening the marital relationship; all members of the family are enlisted in reestablishing ‘intergenerational boundaries’ between the parental dyad and the children.
Phase III is initiated after the patient demonstrates her capacity to maintain a stable weight without high levels of external control. This stage involves several sessions spaced 4–6 weeks apart. Parents are provided with information about normal adolescent development, and the emphasis on fostering independence continues; however, the therapist also works to instill fear about the possibility that symptoms could resurface, in order to ensure continued parental vigilance to the risk of relapse.
A modified form of family therapy is recommended for adult patients. It is inappropriate (as well as impossible) for the family or partner of an adult patient to seize control of her eating behavior—clearly, the 29-year-old Amanda's parents cannot be advised to hold her down and push food into her mouth. Instead, CFT for older patients focuses on restructuring family relationships so that the eating disorder no longer dominates the picture. This application has not been described in the same detail as family therapy for adolescents and, as discussed below, appears to be much less effective. It should also be noted that in the case of adult patients, a decision to implement CFT does imply certain assumptions about the significance of family dynamics in the maintenance of symptoms. It may well be possible to take an ‘agnostic’ view of etiology when using the approach with adolescents, as the tactic of enlisting parents as treatment agents can be justified on purely pragmatic grounds. Because adults necessarily retain principal responsibility for the management of their own symptoms, however, a preference for working with such individuals through a family unit that may no longer reside together requires a theory-based explanation. Many individual therapists might schedule a few sessions with the spouse, parents, or friends of an older anorexic patient (generally because she requests it); however, a therapist who elects to see her primarily or exclusively with her family members present is making a much stronger statement about why she became or remains ill.
Family therapy is the most extensively researched treatment for anorexia nervosa, contributing at least one cell to half of all controlled trials of psychotherapy. Only one of these studies found family therapy clearly superior to a comparison treatment, and the effect was restricted to patients who carried particularly favorable prognoses by virtue of their young age and brief duration of illness. At least for this subgroup, however, no alternative treatments have been demonstrated to work better than some version of family therapy. On the basis of the accumulated evidence, family therapy is the sole intervention that currently meets the standard of an ‘empirically supported treatment’ for adolescent anorexia nervosa.
The strong association between recency of onset and the likelihood of positive response to family therapy was evident in the first trial conducted by the originators of the Maudsley approach (Russell et al., 1987). In that study, CFT was much more effective than a supportive, dynamically oriented individual therapy with a subset of patients who had become anorexic before the age of 19 and been symptomatic for less than 3 years. The effects of initial treatment were still discernible at 5-year follow-up: 90% of those who had received CFT were classified as ‘recovered,’ while 45% of the patients originally allocated to individual therapy remained anorexic or bulimic (Eisler et al., 1997). In contrast, family therapy was neither effective nor differentially effective for other subsets of patients who had a longer history or a later onset; in fact, there was a tendency for the latter group to do better in individual therapy, although few patients responded well to either treatment.
Subsequent research has confirmed the importance of short duration as a predictor of response to CFT. Indeed, the data suggest that the window for successful intervention is even narrower than the 3-year period used to form subgroups in the Russell et al. (1987) study. In a project carried out by the same investigators, all participants had been anorexic for just 2–36 months, with an average duration of 12.9 months and a mean age of 15.5 years (Eisler et al., 2000). Even within this extremely restricted range, there was a significant correlation between how very recent onset had been and treatment outcome in either of two forms of family therapy. Patients who were doing well at 1 year had been anorexic for a mean of 8 months at the inception of treatment, compared with 16 months for those with intermediate or poor outcomes. Another historical variable was also linked to treatment response. When patients who had received repeated prior treatment on an inpatient or outpatient basis were compared with those obtaining therapy for the first time, the contrast was again sharp: 73% of the treatment veterans did poorly in family therapy, while only 19% of the novices failed to improve.
The significance of these data is underscored when we consider their implications for the sample cases of Chloe and Amanda. There is no reason to anticipate that 29-year-old Amanda would respond to family therapy; indeed, she falls into the category of adult patients for whom individual therapy appeared slightly—if rarely—more effective in the initial study. Chloe, however, seems to match all specifications for the empirically supported treatment of CFT: the onset of her disorder was squarely in the middle of adolescence, she has been anorexic for just over a year, and she is still living at home in an intact (and concerned) family. If we try to extrapolate her prognosis from the figures provided by Eisler et al. (2000), however, Chloe's outlook appears less sanguine. At a duration of 13 months, she falls right in between the group of patients for whom family therapy was found to be effective and those for whom it was not. The fact that she has already been a treatment failure elsewhere is ominous as well. Even though the nonspecific therapy, nutritional counseling, drug treatment, and brief hospitalization to which she has been exposed may not represent particularly promising interventions for her disorder, their presence on her treatment record consigns her to the category from which only one-fourth of patients will emerge as successful responders to family therapy.
This pattern could have a number of plausible explanations, and the alternative possibilities hold different implications for how we should view the results of family therapy. In the early stages of anorexia nervosa, patients may not yet have crystallized their identities around the disorder, and it is conceivable that it is easier and more efficacious to exercise external control over the expression of symptoms in such cases. It is also possible that early intervention appears to work better in part because we end up counting among our ‘treatment successes’ the subset of patients whose disorders would be self-limiting with or without professional (or parental) intervention.
Although it is clear that family therapy is effective principally for briefly ill anorexic patients, it has not been established that it differs from other forms of treatment in this regard. It may well be that alternative approaches are comparably constrained. Certainly, the general pattern of correlation between duration and outcome obtains across most of the treatment trials and uncontrolled follow-up studies reported in this field; however, few have analyzed data with sufficient precision to confirm or disconfirm the stark association between months of symptom persistence and treatment response evident in Eisler et al. (2000).
The view that family therapy is preferentially indicated for the treatment of recent-onset anorexia nervosa depends on the demonstration that it resolves such cases faster or more completely or in a higher proportion of patients than alternative therapies. The answers to those questions are less clear than the wide disparity found by Russell et al. (1987) suggested. The pronounced superiority of family over individual treatment in that initial study—evident even with samples of 10 and 11 patients per cell—certainly offered a compelling basis for further investigation. Commendably, proponents of family therapy did continue to examine the method they advocate; inexplicably, however, they stopped comparing it with anything else. The Maudsley group never tried to replicate their remarkable finding with larger samples or alternative forms of individual therapy. Instead, they embarked on a series of intramural studies comparing different formats and intensities of family therapy (le Grange et al., 1992; Lock, 1999; Eisler et al., 2000), as if the case for its superiority over other modalities were already amply documented.
Three different teams of investigators did take up some of the basic questions bypassed by the Maudsley group, with mixed results. Two studies revisited the question of family versus individual treatment. When individual therapy was operationalized in the form of an ‘ego-oriented’ approach in one trial, family therapy (combined with some CBT elements) appeared slightly but not durably more effective with a sample of adolescent patients who had been ill for less than a year (Robin et al., 1994, 1995). When the individual treatment condition was CBT, both modalities yielded equivalent and fairly positive results with adolescent and young adult patients, with no trends favoring either approach for any subgroup (Ball, 1999). A third study found no differences between eight sessions of family therapy and eight sessions of group family psychoeducation when these were provided adjunctively in connection with inpatient treatment for adolescents (Geist et al., 2000).
Interestingly, the intramural research to which the Maudsley investigators turned did identify one mode of treatment that appears superior to CFT: an alternative format for delivering the same Maudsley message. In two studies, the standard ‘conjoint’ approach was compared with ‘separated’ family therapy (SFT), in which parents and the anorexic child were counseled in different sessions (le Grange et al., 1992; Eisler et al., 2000). In parent meetings, the therapist provided advice consistent with the parental control strategies of CFT, while anorexic patients received supportive individual therapy that could include discussion of both family and eating/ weight issues. On theoretical and clinical grounds, SFT was clearly expected to prove weaker than CFT, as it offered no direct opportunities to observe and intervene in family dynamics, did not include meal sessions, and did not involve siblings.
Across both trials, however, there was a trend favoring SFT over CFT. In the second and larger project (Eisler et al., 2000), nearly twice as many patients achieved a ‘good’ outcome through SFT (48% versus 26%), while fewer than half as many patients did poorly (24% versus 53%). This effect was accounted for by the subset of families in which parents frequently directed critical remarks toward the anorexic child. When subgroups of cases high and low in expressed emotion (EE) were compared, SFT was significantly and strikingly more effective than CFT with high EE families, benefiting 80% versus 29% of the patients treated; for low EE families, no trend favored either format.
It is commendable that the Maudsley investigators put themselves in a position to learn that their assumptions about what works best for anorexia nervosa were mistaken. To date, however, their response to these unusually decisive results has been disappointing—both for this specialty area and the evidence-based treatment movement as a whole. Their own findings indicate that SFT is a slightly better treatment option overall and a dramatically better one for patients with the misfortune to come from contentious families. Yet the Maudsley group recently published a manual that strongly advocates the less effective conjoint format (Lock et al., 2001), and is using that approach rather than SFT in ongoing research (Lock, 1999). At present, then, a curious anomaly attaches to the empirical standing of family therapy for anorexia nervosa. CFT is at once the best-supported treatment for recent-onset adolescent patients—and one of the very few ‘active’ modalities in the field that has been found inferior to an alternative approach. A therapist who was committed to practicing validated treatments should indeed adopt the Maudsley model for cases matching the profile of Chloe; ironically, however, he or she should not adhere to the manual written to disseminate the approach, as it describes a version of family therapy that has been shown to disadvantage a sizeable subgroup of the patients to whom it is applied.
More broadly, it should be noted that no study has yet examined the merits of the specific type of family intervention espoused in the Maudsley model. Across orientations, most specialists advocate working with parents when treating individuals in the young-to-mid-adolescent age group, sometimes using principles and techniques quite different from those associated with the Maudsley model. Only direct comparisons can illuminate which of these should be preferred. At present, all that can be stated with some confidence is that seeing family members together does not contribute to positive outcomes, and is contraindicated for a subgroup of particularly vulnerable patients.
Psychodynamic approaches do not fit comfortably into the format used to profile other modalities in this chapter. The difficulty is that there are too many alternatives to cover, none of which is dominant in the eating disorder field. They differ so markedly that there would be multiple ‘theories’ and ‘treatment descriptions’ to summarize under the section subheadings, while the ‘empirical evidence’ that has been collected bears only on the specific variants tested.
In this specialty area, the designation of a treatment approach as ‘psychodynamic’ conveys little information about the conceptual model that guides it or the techniques it subsumes. Drive-conflict, object relations, and self-psychological models disagree about why people become anorexic and how they should be helped to recover (Goodsitt, 1997). According to different accounts, self-starvation is a defense against oral impregnation or aggressive fantasies (Waller et al., 1940/1964; Masserman, 1941; Freud, 1958; Szyrynski, 1973), a reaction to maternal impingement and/or hostility (Masterson, 1977; Selvini-Palazzoli, 1978), or a desperate attempt to organize and empower the self (Bruch, 1973; Casper, 1982; Goodsitt, 1985, 1997; Geist, 1989; Strober, 1991). Therapists may be advised to interpret the meaning of the patient's symptoms (Thoma, 1967; Sours, 1974, 1980; Crisp, 1980, 1997) or to offer her a healing relationship with a caring adult (Goodsitt, 1997); alternatively, both of these prescriptions may be misguided and perhaps downright dangerous (Bruch, 1988). Depending on the source consulted, eating and weight issues should be addressed, ignored, or delegated to someone other than the therapist. Some treatment proposals specify a 25-session course of outpatient psychotherapy (Treasure and Ward, 1997a), while others advocate 6–24 months of residential care (Story, 1982; Strober and Yager, 1985). Clearly, any attempt to generalize across such diverse models, methods, and formats would be uninformative.
Only a few characteristics help to distinguish psychodynamic approaches from alternative methods (although none is universal across or exclusive to this group of therapies). Psychodynamic therapists are more likely to endorse the view that ‘it's not about eating and weight,’ to explore the origin of symptoms, to focus on longstanding conflicts or deficits, to encourage the expression of emotion, and to highlight the therapeutic relationship. They are, in general, less likely to emphasize the provision of facts about the disorder, to give advice about the management of eating and weight, to examine disorder-specific beliefs, to suggest extra-therapy activities, or to use an active, directive style during sessions.
Another factor complicating the review of psychodynamic models is that they are routinely combined with other approaches in the treatment of anorexia nervosa. Virtually all therapists find their accustomed modes of practice challenged by the distinctive features of this disorder, and many venture outside familiar frameworks in search of better alternatives (Garner and Bemis, 1982; Casper, 1987; Tobin and Johnson, 1991; Palmer, 2000). The identity crisis seems especially acute, however, for those who practice nondirective forms of therapy. To a greater extent than family therapists or CBT therapists, clinicians whose primary affiliation is psychodynamic tend to favor a ‘hyphenated’ approach when working with anorexic patients, borrowing elements from family systems, CBT, interpersonal, experiential, and medical models. Most are (commendably) reluctant to overlook patients’ current health, weight, eating behavior, and patently false beliefs, while tracing the origins of their difficulties to early developmental deficits. In response, some adopt a pragmatic eclectic approach, importing symptom management strategies from other orientations to put alongside the techniques they prefer. Others modify psychodynamic therapy itself to suit the distinctive features of patients with this disorder.
For example, the influential theorist and therapist Hilde Bruch (1973, 1978, 1988) outlined a causal model of anorexia nervosa consonant with her psychoanalytic training, yet cautioned that traditional psychodynamic therapy was ‘singularly ineffective’ and ‘potentially harmful, even fatal’ when applied to these patients. She recommended using a more direct ‘fact-finding treatment’ that enlisted the patient as a ‘true collaborator’ in the effort to identify and challenge specific ‘false assumptions or illogical deductions’ (Bruch, 1962, 1978, 1985). The therapeutic style that Bruch described as more effective with this population bears a striking resemblance to Aaron Beck's cognitive therapy (A. T. Beck, 1976; A. T. Beck et al., 1979; J. S. Beck, 1995; Greenberger and Padesky, 1995) and adapted versions designed for use with anorexic patients (Garner and Bemis, 1982, 1985; see subsequent section on CBT).
Only a few psychodynamic interventions for anorexia nervosa have been outlined in detail, including the hybrid approaches labeled ‘feminist psychoanalytic therapy’ (which also incorporates elements of CBT; Bloom et al., 1994) and cognitive analytical therapy (CAT; Treasure and Ward, 1997a). Still fewer have been both specified and examined in controlled trials, including CAT and focal psychoanalytic psychotherapy (FPP; Dare and Crowther, 1995).
CAT is a time-limited dynamic therapy (Ryle, 1990) that is described as ‘uniquely positioned between [the] extremes’ of symptom focus and insight orientation (Bell, 1999, p. 36). As applied to anorexic patients, the format involves 20 weekly sessions followed by 3–5 monthly follow-up visits (Treasure and Ward, 1997a; Dare et al., 2001; Tanner and Connan, 2003). Working collaboratively, the therapist and patient identify target problems and analyze the ‘traps,’ ‘snags,’ and ‘dilemmas’ through which these are maintained. Therapy also examines interpersonal patterns, termed ‘reciprocal roles,’ which are traceable to early relationships and form the background for the patient's present experience. This information is mapped on to a visual schematic called the ‘sequential diagrammatic reformulation’ that depicts connections between the individual's symptoms and her relationships and self-concept, and becomes the basis for ongoing monitoring and discussion in therapy.
FPP is a more traditional approach based on Malan's work (1976, 1979) and adapted for anorexia nervosa by Dare and Crowther (1995). In the context of research, treatment is delivered weekly for 1 year. Therapy is organized around a ‘focal hypothesis’ that links the patient's internalized representation of significant people in her past to her evolving feelings for the therapist and the function of her symptom in current personal relations. Anorexia nervosa is viewed as a means of gaining a spurious sense of control, in an effort to manage patients’ central fear of the vulnerability experienced through closeness, and as a powerful method of soliciting care from others. Analysis of transference and countertransference phenomena is prominent in this mode of treatment. Weight is monitored by a nurse and reported to the therapist, who charts and discusses weight changes with the patient in connection with other developments as they unfold in psychotherapy.
Six controlled trials have included at least one cell of psychodynamic therapy. Unfortunately, three of these describe the modalities in minimalist terms, saying little more than that one treatment condition was ‘psychodynamically oriented.’ In view of the diversity of models, such brevity means that we have no way to determine which treatment principles are being supported or invalidated by the results. One of these investigations found a psychodynamic condition inferior to dietary counseling (Hall and Crisp, 1987), one inferior to family therapy for adolescent but not late-onset cases (Russell et al., 1987), and one equivalent to inpatient care and superior to treatment as usual (Crisp et al., 1991).
The remaining three trials, two of which included CAT, provide more interpretable information. As noted in the section on family therapy, Robin et al. (1994) reported that ego-oriented individual therapy was slightly less effective than family therapy with young, recent-onset anorexic patients. A pilot study comparing CAT to an ‘educational behavioral’ treatment found no differences between conditions at 1-year follow-up (Treasure et al., 1995). Most patients in both groups gained weight but only about a third of each achieved a good outcome.
A subsequent study compared CAT, FPP, family therapy, and low-contact routine treatment (Dare et al., 2001). All interventions were provided on an outpatient basis to a sample of adult patients who would be expected to carry a poor prognosis as a function of their average age (26 years), extended duration of illness (6 years), low weight (BMI of 15.4), and history of prior treatment (79% overall, 43% inpatient). When reassessed a year after treatment initiation, most patients in all conditions remained underweight, with an average BMI of 16.5. A few group differences attained significance: patients assigned to routine treatment were more likely to require hospitalization than those in any of the three specialized therapies, and gained less weight than patients in focal psychoanalytic or family therapy (but not CAT). On an intent-to-treat basis, 28–37% of those allocated to the specialized treatments had recovered or significantly improved, versus 5% of those getting routine care; however, half to two-thirds of the former and three-fourths of the latter were still doing quite poorly. Moreover, because of design inequities, even the obtained differences between the specialized therapies and routine treatment are not clearly interpretable as support for any one (or all three) of these specific modalities. Widely varying lengths and densities of therapy were used across conditions; routine treatment was delivered by psychiatric trainees with less overall and disorder-specific experience, who transferred their anorexic patients/subjects to another therapist when rotated to a new service every 6 months. As a result of these discrepancies, differences in outcome cannot be attributed to particular models versus the general advantages of treatment amount, continuity, and expertise.
While the available evidence is not strongly supportive of any form of psychodynamic treatment, it should be stressed again that no intervention of any kind has so far yielded satisfactory results with the patient group most often included in these trials: older adolescents or adults with established anorexia nervosa. Psychodynamic models have been highly influential, however, in shaping the ways therapists conceptualize and treat eating disorders. Although few clinicians practice therapy precisely as specified by CAT or FPP, psychodynamic principles inform the work of most. Bruch's characterization of symptoms as a desperate struggle for a self-respecting identity, Crisp's depiction of flight from psychobiological maturity, and Goodsitt's emphasis on the importance of a healing relationship have all been incorporated into dominant clinical views of the disorder. Above all, psychodynamic approaches underscore that the eating and weight symptoms that command our attention do not define the scope of problems faced in the treatment of anorexia nervosa.
A cognitive-behavioral framework for understanding and treating anorexia nervosa was initially described by Garner and Vitousek (Garner and Bemis, 1982, 1985; Garner et al., 1997). The model overlaps substantially with Fairburn's (1981, 1985) analysis of bulimia nervosa, reflecting the CBT perspective that these disorders share many core features and maintaining variables. At the center of both is the premise that personal worth is dependent on the size and shape of the body. This dominant idea spins off a host of specific irrational beliefs, conditions a characteristic set of fears, and prompts stereotyped avoidance behaviors. Over time, anorexic and bulimic individuals begin to process information in accordance with predictable cognitive biases and respond to increasingly eccentric reinforcement contingencies. In addition, anorexic individuals incur the hard-wired consequences of semistarvation, which also contribute to the entrenchment of the pattern (Garner and Bemis, 1982).
To a greater extent than other models, cognitive accounts stress the positively reinforced and ‘organizing’ functions of anorexia nervosa, postulating that these explain its most unusual features better than the avoidance-based functions that are also present and influential (Garner and Bemis, 1982; Slade, 1982; Bemis, 1983; Vitousek and Hollon, 1990; Vitousek and Ewald, 1993; Wolff and Serpell, 1998; Fairburn et al., 1999b; Vitousek, 2005). These distinctive features include a sense of ‘specialness,’ moral certitude, competitiveness, and positive identification with the disorder (Vitousek, 2003). Because the sum of these distinctive elements seems to explain the distinctive resistance to change in this disorder, CBT for anorexia nervosa is organized around efforts to address them.
The CBT approach has been outlined in a series of papers that describe different components of the treatment package (Garner and Bemis, 1982, 1985; Garner, 1986, 1997; Orimoto and Vitousek, 1992; Pike et al., 1996; Garner et al., 1997; Vitousek et al., 1998; Wilson and Vitousek, 1999); however, no treatment manual combining this material is available. The format specifies an extended course (1–2 years) of individual therapy, supplemented with family sessions if indicated. One-to-one therapy is considered essential to the delicate work of addressing motivational issues and idiosyncratic beliefs. The long duration reflects the time required to engage reluctant patients as active participants in the change process, as well as to help them reach normal weight and recover from the persistent after-effects of semistarvation.
The CBT model has a strong bias toward accomplishing weight restoration on an outpatient basis whenever possible, to maximize patients’ sense of responsibility for decision making and minimize the risk of reactance to external control. In some cases, inpatient or partial hospital treatment may be essential; guidelines are available for using CBT principles in such settings (Bowers et al., 1997).
Treatment phases parallel the three-stage sequence common to CBT and IPT for bulimia (and to some extent, family therapy for anorexia): an initial phase for engagement, provision of rationale, and beginning steps toward change; a middle phase for focused work on identified maintaining variables; and a concluding phase for consolidation and relapse prevention (Garner et al., 1997). In practice, however, the progression of CBT for anorexia nervosa is less fixed than these divisions imply. The general movement is from developing motivation to modifying eating and weight to examining disorder-specific beliefs to focusing on broader aspects of self-concept; however, all of these issues are necessarily addressed throughout therapy, and many CBT techniques target multiple areas simultaneously.
In descriptions of CBT for anorexia nervosa, considerable space is devoted to suggested strategies for engaging patients’ interest in the prospect of change and then translating that interest into action. Four emphases are identified as crucial to the promotion of change (Vitousek et al., 1998). The first involves the nonconfrontational use of psychoeducational information to help the patient reassess the perceived risks and benefits of her symptoms and reconstrue their meaning. The second is an affirmation of the experimental method of CBT, which casts each proposed step in therapy as an opportunity to gather information rather than an irrevocable commitment to change. A third key theme is an emphasis on exploring the functional effects of patients’ choices, rather than challenging their rationality or validity. A substantial portion of the first few sessions of therapy is typically devoted to helping the patient develop a list of the advantages and disadvantages of her eating disorder, phrased in her own terms (Vitousek and Orimoto, 1993). Samples of the kinds of material provided by patients such as Chloe and Amanda are included in Table 15.1 (see discussion in the subsequent section on Attention to motivational issues). The serious attention given to the perceived advantages of symptoms can be disarming to patients who are accustomed to being warned about the dangers of their behavior. The therapist is advised to acknowledge these benefits without minimizing or disputing them. At the same time, she or he introduces a theme that will recur throughout treatment: the disadvantages the patient is experiencing are inextricably linked to subnormal weight; however, it may be possible to secure the positive effects at lower cost through alternative means.
|
Table 15.1 Advantages and disadvantages of anorexia nervosa
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
The fourth theme is an exploration of philosophical issues that bear on patients’ attachment to symptoms and fear of change (Vitousek et al., 1998; Vitousek, 2005). CBT advocates working through each patient's personal values to convince her that her anorexic way of life violates key principles that are even more fundamental to her sense of identity. For example, Amanda echoed the common anorexic view that denying herself desired foods and working out several hours a day were testimony to her strength and self-discipline—characteristics she valued highly in herself and others. In fact, after years of anorexia nervosa, adherence to these rigid, fear-driven patterns of behavior represented the path of least resistance. For Amanda, the truly brave and difficult choice would be to violate her anorexic system of rules by eating forbidden foods or defying the impulse to exercise.
Because many anorexic individuals are passionately committed to their beliefs, work with these patients can seem more analogous to the conversion of a member of the National Rifle Association to a gun control advocate, or a religious fundamentalist to Unitarianism, than it does to psychotherapy with a depressed or anxious patient. It follows that attempts to dispute anorexic beliefs logically are seldom successful—and are not advised by CBT experts in this area. The treatment approach does make use of the conventional CBT techniques of cognitive restructuring and prospective hypothesis testing; for example, the therapist and patient might collaborate in designing an experiment to check out the patient's belief that other people respond to her more favorably when she loses weight. Contrary to stereotype, however, CBT does not assume that anorexic patients will give up their symptoms once the therapist points out their ‘errors in thinking’ and challenges their irrational beliefs. Instead, therapists are encouraged to draw on a blend of factual, functional, and value-related material to enlist patients in reexamining the relationship between anorexic symptoms and their own goals and ideals.
The processes of dietary rehabilitation and weight restoration are not carried out in isolation from the rest of CBT but integrated with the ongoing examination of patients’ beliefs. Initially, patients are encouraged to follow individualized, structured meal plans, gradually introducing larger amounts and avoided food types. Meal planning is usually incorporated into regular sessions and conducted by the primary therapist. In vivo therapy sessions may be used to assist patients with particularly challenging situations, such as grocery shopping, eating in restaurants, or trying on new clothes (see section on Attention to eating and weight).
During the course of therapy, attention gradually shifts from the focal symptoms of anorexia nervosa to more general aspects of self-concept and interpersonal relationships. It is not necessary to switch paradigms in order to address these issues, as CBT offers mode-consistent principles for work on this level. In the later stages, patients are encouraged to experiment with new strategies for achieving their goals, new sources of positive reinforcement, and new standards for gauging personal worth.
Paralleling the general state of treatment research across the eating disorders, there is a vast gap between the empirical standing of CBT for anorexia nervosa and for bulimia nervosa. During the first 7 years after the approach was proposed, several case studies (Cooper and Fairburn, 1984; Garner, 1988; Peveler and Fairburn, 1989) and one small controlled trial (Channon et al., 1989) were reported. Very recently, four comparative studies have been completed and others are in progress. Only a few tentative observations are warranted pending publication of these data.
Two recent controlled trials compared CBT with nutritional counseling. The first of these broke down after 100% of the 10 patients assigned to nutritional counseling dropped out of treatment and refused further contact; in contrast, 92% of the 25 patients allocated to CBT persisted to completion of the 20-session series (Serfaty et al., 1999). Although statistical analyses of outcome were precluded by the mass defection of patients from nutritional counseling, it was reported that those who had received CBT showed significant changes in BMI and on measures of eating disorder and general symptoms.
Findings from a second study confirmed the pattern of differential attrition from these treatment conditions (Pike et al., 2003). This investigation was designed as a ‘relapse prevention’ trial, with patients randomly assigned to 50 sessions of individual CBT or nutritional counseling and medical management after completing inpatient weight restoration. The study included a severe sample of 33 adult patients (average age 25 years) with longstanding anorexia nervosa (7.5 years). Fewer patients in the CBT condition terminated prematurely (27% for CBT versus 53% for nutritional counseling) and more met criteria for ‘good’ outcome at the end of treatment (44% versus 7%).
Another trial compared CBT, fluoxetine, and combined treatment conditions with a sample of 108 partially weight-restored anorexic patients (Halmi, 2000). Final results have not been reported, but the interim data suggested that CBT, alone or in combination with medication, also conferred some protection against premature termination compared with medication alone. The extremely high dropout rates already evident for all conditions at mid-treatment are troubling, however, and inconsistent with the patterns seen in other investigations.
Collectively, these findings support the tentative conclusion that CBT does further at least two of the goals it was expressly designed to fulfill: higher rates of initial engagement and treatment persistence in these notoriously ‘resistant’ patients. While it is tempting to attribute these desired effects to the collaborative style and motivational emphasis of CBT, such inferences are premature. Because each of these studies compared CBT with a nonpsychological intervention, they suggest only that psychotherapy—perhaps, but not necessarily, in the specific form of CBT—produces better outcomes than nutritional counseling and/or drug treatment alone (Vitousek, 2002). Ironically, the choice of weak comparison treatments has made it difficult to gauge the efficacy of CBT. In order to determine whether CBT confers any benefits beyond its apparently greater capacity to retain patients, researchers must identify comparison treatments that serve the same objective at least equally well, so that sufficient numbers of patients are willing to remain in the alternative condition.
To date, only two investigations have examined the effects of CBT relative to other forms of psychotherapy. Both used abbreviated versions of CBT (20–25 sessions) with patients who were underweight or partially weight restored. One of these found CBT equal to BT and treatment-as-usual with adult patients (Channon et al., 1989); a second obtained positive and equivalent results using CBT or family therapy with adolescents and young adults (Ball, 1999).
In view of the fact that no form of psychotherapy has been shown to work better than any other form of psychotherapy for adult anorexic patients, how should clinicians evaluate the merits of CBT relative to other treatment options, pending the availability of more instructive data? Several considerations recommend the approach as a defensible interim choice (Vitousek, 2002; Fairburn and Harrison, 2003). One argument is the documented success of a related approach for bulimia nervosa. Because anorexic and bulimic patients share many beliefs and behaviors, it seems likely that at least some of the same strategies will prove effective in treating them. Another putative benefit of CBT is its integration of direct work on eating and weight with attention to motivational issues—a characteristic that may become increasingly appealing as outpatient services are forced to take on more responsibility for the weight restoration phase of treatment.
A disadvantage of CBT is the fact that this complex intervention requires considerable training to deliver. In addition, all CBT experts concur that the treatment must be lengthy—not the 18–25 sessions used in most trials to date, but something on the order of 40–60 sessions in the usual case of established anorexia nervosa (Garner et al., 1997; Fairburn et al., 2003; Pike et al., 2003). Such extended outpatient treatment clearly requires justification through data showing that it reduces the need for expensive inpatient care and subsequent services to a greater extent than brief interventions.
Recently, this area has been invigorated by new proposals for shifts in emphasis in the basic CBT model, offered both by its originators and other CBT experts in the eating disorder field. Like the initial approach, however, these suggested revisions are based on clinical experience rather than accumulated evidence about the strengths or weaknesses of existing models. As we know very little about how well the ‘traditional’ CBT approach to anorexia nervosa works, it remains a matter of conjecture how it might be improved (Vitousek, 2002). Some specialists have suggested that the ‘traditional’ model is too narrow, paying insufficient attention to interpersonal issues and ‘deep’ aspects of the self (Leung et al., 1999); others have speculated that the model is too broad, allocating unnecessary attention to interpersonal issues and ‘deep’ aspects of the self (Fairburn et al., 1999b). Specific aspects of the approach have also been recommended for closer focus, notably work on the extreme need for self-control (Fairburn et al., 1999) and the connection between symptoms and values (Vitousek, 2005). Because the few data available already indicate that many anorexic patients will fail to achieve full recovery with CBT (or any other tested modalities), thoughtful modifications to the existing approach should be examined through systematic case study or small group designs.
If the length of this section were proportionate to the number of medications tested, it would dominate a review of alternative treatments for anorexia nervosa. According to a leading specialist (Walsh, 2002b), however, the list of agents that have proven beneficial can be summarized succinctly: none. Paradoxically, the most important contribution of pharmacotherapy research may be the repeated demonstration that drugs are ineffective in the resolution of this disorder.
In other specialty areas, pharmacotherapists are sometimes suspected of overstating the merits of drug treatment relative to psychotherapy. In contrast, their counterparts in this field consistently emphasize the limits on what they have to offer (e.g., Garfinkel and Walsh, 1997; Mayer and Walsh, 1998; Garfinkel, 2002b; Walsh, 2002a,b; Bruna and Fogteloo, 2003). Reviews summarize the evidence in bleak (if honorable) terms: ‘no psychopharmacological treatment for anorexia nervosa has ever proved satisfactory’ (Andersen, 1995, p. 373); ‘to date, no medication has been shown to change eating behavior reliably, assist weight gain… or alter body image disturbance’ (Johnson et al., 1996); ‘to date, medications have added little to overall management’ (Garfinkel, 2002b, p. 225). The recurrence of the phrase ‘to date’ holds out some hope for the future; after all, as one specialist notes, ‘there are always new medications appearing’ (Garfinkel, 2002b, p. 225), and it is conceivable that one will break the string of failures being reviewed. Yet the same phrase reappears in summaries written many years apart, as each promising debut is followed inexorably—at least, ‘to date’—by the accumulation of more discouraging data.
In some instances, drugs are prescribed for anorexia nervosa simply because they carry side-effects that promote weight gain (Walsh, 2002b). As in the case of pharmacotherapy for bulimia nervosa, however, most candidate drugs are linked to specific models about what has gone awry and why the proposed medication should help put it right. Most of these conjectures are plausible, because anorexia nervosa subsumes a variety of psychiatric and medical symptoms for which useful drug treatments have been identified (Walsh, 2002a). For example, the ubiquity of depression and prominence of obsessive-compulsive patterns in anorexic patients support the use of antidepressants, while the near-delusional quality of their distorted thinking warrants trials of antipsychotic medication.
Antidepressants seem to provide little benefit in promoting weight gain, but one study has reported that fluoxetine may help forestall relapse after weight restoration (Kaye et al., 1997; Ferguson et al., 1999), and additional investigations are currently in progress. In one of these, however, the dropout rate from the medication condition had already reached two-thirds by treatment midpoint (Halmi, 2000). Case reports suggest some benefit from the atypical neuroleptic olanzapine (La Via et al., 2000; Boachie et al., 2003; Malina et al., 2003). In view of the long record of dashed hopes in this area, however, even cautious optimism should be deferred until results are replicated. (Curiously, the lack of evidence supporting the efficacy of medication has done little to discourage its use; if Chloe had not been placed on antidepressants by her family physician, there is a good chance that they would have been prescribed at the time of her referral to a specialty clinic.)
From one perspective, it may be unreasonable to expect medication to be particularly effective for the purpose of dismantling organized, coherent, highly valued systems of belief. Few pharmacotherapists would be chagrined by their failure to identify a drug that could change the attitudes of political extremists, religious fanatics, or extreme high altitude mountain climbers. Biological factors might well be involved in the development of such patterns; once established, however, they may become inaccessible to modification even if the underlying vulnerability is correctly identified and treated. The same may hold for anorexia nervosa.
Clinicians with minimal background in the eating disorder field are often wary of treating anorexic or bulimic patients. Their reluctance is warranted: in most circumstances, competent care involves referral to specialized services. The treatment of these conditions puts a premium on specific expertise for a number of reasons.
First, semistarvation and the binge–purge cycle have profound effects on physiology and psychology. These consequences are predictable to experts, but can be obscure, alarming, and/or misleading to inexperienced practitioners. For example, chronic caloric deprivation produces an array of symptoms, including depression, anxiety, irritability, impulsivity, social withdrawal, and sexual disinterest, as well as characteristic peculiarities in food-related attitudes and behaviors. Therapists who are not aware that these patterns emerge in well-adjusted individuals undergoing semi-starvation (Keys et al., 1950) are prone to make up case-specific explanations and complicated treatment plans for general phenomena with a parsimonious cause.
Second, as noted earlier, the provision of psychoeducational material is a prominent component of treatment for anorexia and bulimia across most modalities (Olmsted and Kaplan, 1995; Garner, 1997). Clinicians cannot impart such information credibly and persuasively unless they have acquired a solid background in a wide range of relevant topics. It is unrealistic to expect that nonspecialists will have the time to acquire and update the necessary knowledge base; even clinicians who devote their practice to this population have difficulty keeping current across these rapidly developing fields.
Mastery of such material is especially crucial because many patients are themselves amateur experts on dieting, weight, and exercise. They tend to be keen consumers of the jumble of accurate and inaccurate information that is disseminated in popular culture, and often cite specific sources in support of their symptoms. For example, Amanda had audited several nutrition classes at the college where she taught, and justified her abstemious eating in part by referring to solid evidence on the retardation of aging through caloric restriction (Weindruch, 1996; Vitousek et al., 2004). At the same time, she quoted freely from pamphlets picked up at health food stores, attributing her avoidance of specific foods (which happened to be high in calories or fat) to concerns about allergens or toxic build-up in her gastrointestinal tract. In order to help her disentangle the true and false bits of input that she has muddled together, her therapist should know more than Amanda—and more than the average physician or dietitian—about factual matters that affect her willingness to change.
Finally, familiarity with the phenomenology of anorexia and bulimia helps the clinician ask crucial questions, evaluate the plausibility of answers, and establish credibility as someone who understands the private and often protected experience of individuals with eating disorders (Vitousek et al., 1998).
In circumstances where specialized expertise is not available, therapists may find it valuable to act as ‘guides’ for the use of self-help manuals by their clients—a process that can facilitate the acquisition of knowledge and skill by both parties (Birchall and Palmer, 2002). Supervision through teleconferencing may also be beneficial for clinicians who work in sparsely populated areas (Mitchell et al., 2003).
Most experts consider direct work on eating disorder symptoms essential for patients with anorexia nervosa and desirable for those with bulimia nervosa. There is some disagreement, however, about the degree of emphasis such work should be given and whether it should occur within or outside the context of psychotherapy.
As discussed in the section on bulimia, at least one modality that does not address specific symptoms (IPT) can yield benefits approximately equal to the ‘treatment of choice’ that does (CBT), while therapy focusing exclusively on behavior (BT) may be contraindicated (Fairburn et al., 1993a). Even if bulimic symptoms can be eliminated without specific assistance, however, it is not clear why therapists would choose to withhold it. We know that dietary restraint is a risk factor for bingeing and that its reduction mediates improvement during treatment (Wilson et al., 2002)—and we know that bulimic patients get better faster when clinicians give them direct help in changing these patterns.
In the case of anorexia nervosa, we lack the evidence for data-based conclusions about the relative merits of treatments that pay considerable attention, some attention, and no attention to eating and weight; once again, purely symptom-focused treatment in the form of dietary counseling seems to be associated with particularly abysmal results. In practice, however, few specialists are willing to let anorexic symptoms take care of themselves while psychological issues are addressed. There are obvious medical and ethical reasons for a more active approach, and some compelling clinical grounds as well. The heart of the matter is that professionals must attempt to modify undereating and low weight because anorexic patients probably won't, left to their own devices. Unlike bulimic patients who want to stop bingeing and purging, they are not disposed to translate any improvements in overall functioning into symptom control. Moreover, there are much sharper constraints on the extent to which general improvements can occur while semistarvation persists.
The field includes instructive examples of what can happen when therapists focus on ‘deeper’ issues in preference to eating and weight. One disturbing case report describes narrative therapy with a 29-year-old anorexic patient whose BMI was approximately 10 (Lemberg, 1999). The therapist—who apparently persisted in the same approach for 7 years, while the patient's weight remained critically low—wrote that this brilliant young woman ‘deserved much more’ out of life than enslavement by anorexia nervosa. Most experts would agree: At a minimum, she deserved a form of therapy that would not continue discussing her dilemma from alternative perspectives while her life remained on hold and potentially in jeopardy. Another account details the consequences of a day-hospital program that focused on the ‘difficulties underlying [patients'] eating problems’—but elected not to attend to the eating problems themselves (Thornton and Russell, 1995, cited in Zipfel et al., 2002, p. 114). Of the 23 anorexic patients treated with this approach, 95% lost weight while in the program, and 64% required readmission to the hospital.
Some therapists who agree that direct intervention is necessary would prefer that the battles be waged in someone else's office. In many programs, eating and weight issues are managed by dietitians, physicians, and/or nursing staff. The rationale for separating symptom-focused work from psychotherapy is sometimes that sessions should be reserved for matters more significant than what brand of breakfast cereal the patient selects and whether or not a 2-ounce change really constitutes weight gain; it is also argued that the therapeutic relationship should be shielded from the unpleasantness that often surrounds such discussions (e.g., Rampling, 1978; Powers and Powers, 1984). Others simply see dietitians as better prepared for this work (Beumont et al., 1997); certainly, they are less likely to let it slide.
The alternative position has been stated most forcefully by CBT experts, who maintain that dietary counseling and weight management should be incorporated into regular therapy sessions (Garner et al., 1982, 1997; Garner and Bemis, 1985; Wilson and Agras, 2001). Meal planning is not simply a matter of imparting information and issuing instructions, but a persuasive and essentially ‘therapeutic’ undertaking best handled by a clinician who is familiar with all aspects of the patient's situation (Wilson and Agras, 2001). Work on eating and weight invariably provides access to important beliefs and intense emotions, and offers numerous opportunities to take on motivational issues and explore ‘deeper’ concerns. The obvious interdependence of these variables in patients’ own experience should be reflected in the structure of treatment.
Guidelines for conducting this work are available in basic CBT articles (e.g., Garner and Bemis, 1985; Fairburn et al., 1993b; Garner et al., 1997; Wilson et al., 1997; Wilson and Vitousek, 1999) and materials on nutritional counseling (e.g., Beumont et al., 1987, 1997; Rock and Yager, 1987; Reiff and Reiff, 1997). Specific controversies persist about matters such as how rapidly weight gain should proceed and whether or not calories should be monitored, patients informed of their exact weights, and vegetarian diets accepted. The invariant principle is that highly restrictive eating and extremely low weight are incompatible with progress in therapy. A continued trend toward improvement in these areas is a marker of effective outpatient treatment. In general, a different pace of change would be expected for subgroups of patients matching the profiles in the section on anorexia nervosa. For individuals such as Chloe, whose weight loss was recent and precipitate, a fairly assertive program of weight restoration might be appropriate. For patients such as Amanda, whose low weight has been relatively stable for years, more gradual increments are usually indicated—in part because they are often all that these patients can be persuaded to consider.
One basic strategy used in CBT, BT, and adjunctive nutritional counseling is self-monitoring of food intake. For both bulimic and anorexic patients, self-monitoring provides a means of assessing the temporal pattern, quantity, and quality of dietary intake, and can yield information about the precipitants and consequences of targeted events such as binge-eating. A sample record from the bulimic patient Sharon is shown in Figure 15.1. The form is similar to that recommended by Fairburn (1995), and can be adapted to suit the specific needs of individual patients. Typically, such forms include columns for recording the timing and context of eating episodes, the type and amount of foods consumed, the patient's subjective judgment about whether the event constituted a binge, the occurrence of purging, and the type and duration of exercise. CBT therapists usually encourage patients to record food quantities in approximate and colloquial terms (such as ‘a large bowl of cereal’ or ‘half a piece’), avoiding the precise measuring or weighing of food and the counting of calories or fat grams (Fairburn, 1995; Wilson and Vitousek, 1999). In addition, patients may be asked to summarize their thoughts and emotions during different phases of the binge–purge cycle, or to write down a brief analysis of the factors contributing to its occurrence. It can also be useful for patients to identify the point at which they made a decision to initiate an episode or to designate eating that was already underway as a ‘binge.’ In Figure 15.1, Sharon has used an asterisk to mark when this occurred.
Review of Sharon's daily record suggests several themes that may contribute to maintaining her disorder and triggering specific incidents of binge eating, including erratic meals, long periods of deprivation, fatigue, isolation, and interpersonal disappointment. These linkages can help Sharon and her therapist identify and change patterns that increase her vulnerability to overeating and purging. For example, one obvious goal for Sharon would be to include breakfast in her regular routine, in part to lessen the likelihood that she will eat unplanned foods on a haphazard basis (such as the chocolate doughnut she encountered at work), and then interpret her ‘lapse’ as proof that she cannot exercise self-control. If the association between feelings of loneliness and/or abandonment and symptomatic behavior recurs in a number of situations, it would also become an important focus for work in psychotherapy.
Some behavioral changes are so challenging that they may not be attempted without more direct assistance from the therapist. In these instances, in vivo sessions can be an invaluable addition to discussions in psychotherapy. Although therapist-assisted exposure is a common component of BT and CBT for other anxiety-related disorders, this strategy has been surprisingly neglected in the eating disorder field—except in the form of office-based sessions for exposure and response prevention (ERP) to bingeing and/or purging cues (e.g., Rosen and Leitenberg, 1985; Wilson et al., 1986; Agras et al., 1989; Jansen et al., 1992; Carter et al., 2003) and, more recently, body size in the mirror (e.g., Tuschen and Bent, 1995; Rosen, 1996; Wilson, 1999). In addition to these applications, exposure principles can be applied flexibly to a wide range of issues that hamper progress in recovery.
In the very early stages of therapy, in vivo sessions can take the form of supervised meals with patients who are eating infrequently or extremely poorly, or who are unable to interrupt the binge–purge cycle without external structure and support. For example, for a patient such as Emily, who induces vomiting almost every time she eats, the therapist might arrange several extended sessions that involve eating a regular meal, then assisting with anxiety management until the high-risk period for self-induced vomiting has elapsed. Clearly, sessions of this kind cannot be scheduled with sufficient frequency to replicate the meal supervision available in day hospital or inpatient settings, and should not be used for more than brief periods of intensive support. In our experience, however, such interventions sometimes help patients surmount barriers to change that they cannot negotiate on their own between therapy sessions, allowing them to accomplish the initial steps toward symptom control without the cost or disruption of inpatient treatment.
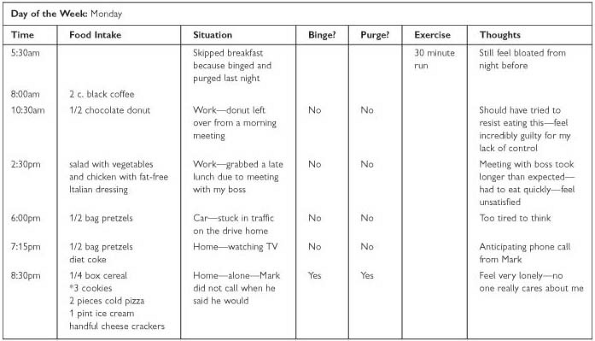
|
|
Fig. 15.1 Food record. |
In vivo eating sessions can also be focused on the reintroduction of especially distressing ‘forbidden foods,’ exposure to avoided situations (such as fast-food restaurants), and modification of specific eating rituals (such as eating slowly or ‘dissecting’ food). Other kinds of sessions can be devised to target a variety of problems related to food, weight, and exercise. For example, the long-term anorexic patient Amanda adhered to a highly restrictive vegetarian diet, limiting her selection to just eight specific food items (e.g., defatted tofu, a single brand of plain yogurt, one type of bran cereal) that she was willing to consume, in addition to fruits and vegetables she deemed ‘safe.’ During meal planning sessions, Amanda was unable to come up with any alternatives she might consider sampling, and rejected each suggestion offered by her therapist as unappealing, inconvenient, or ‘unhealthy.’ Rather than debating the merits of each candidate in the office, the therapist suggested spending a session in a health food store (and subsequently in a regular supermarket) reviewing and selecting additional choices. To some clinicians, this kind of intervention may seem superficial and ‘nonpsychological,’ in that it takes expressed concerns at face value and addresses them as practical problems to be solved. As emphasized above, however, direct work on these issues usually elicits valuable material that may be less accessible through verbal reconstructions. When patients are assisted in taking active steps to live differently, rather than simply encouraged to talk about their inability to do so, both parties get a much clearer view of the attitudes and fears that support eating disorder symptoms.
More ‘advanced’ in vivo sessions can be organized around creative scenarios that often include elements of role-play. For example, after making substantial progress in therapy, the adolescent patient Chloe came to a session distraught over a comment a friend had made about Chloe's increased weight and more normal eating behavior. Chloe recognized that the remark had been intended as a compliment, but felt humiliated that her weight gain was obvious to others and ambivalent about losing her identity as ‘the anorexic’ in her school. Chloe also said that she found it distressing to be around other girls who made disparaging comments about their own body size and talked about their diet regimens, at a time when she was trying to reduce the salience of these concerns in her own self-evaluation.
After affirming the difficulty of change in the context of conflicting messages, the therapist helped Chloe consider the relative merits of coping through attempted avoidance of such events versus building her confidence that she could handle their inevitable occurrence. Chloe and her therapist decided to set up an in vivo lunch session in which the therapist would play the role of a friend who repeatedly talked about feeling fat, asked for advice about dieting, and expressed surprise about the nonrestrictive food choices Chloe was making. During that session, Chloe tried out a variety of different responses to the scenarios presented, and gained on-the-spot assistance in working through her own reactions. She subsequently reported that similar events were much less upsetting, noting that ‘instead of walking around wondering when the next hurtful thing is going to happen, I get kind of curious about which way I'll decide to handle it when it does.’
Across all in vivo experiences—particularly those designed to elicit anxiety in a sensitive domain—it is crucial that the patient view the exercise as chosen rather than imposed. Each session should be worked out collaboratively on an individual basis, with the parameters negotiated and fixed in advance. If a patient becomes distressed and reluctant to continue during an exercise, the therapist should be in a position to refer her back to her own decision to take on the problem through this experiment, rather than pressuring her to comply with an external demand for change.
Until quite recently, specialists have agreed that anorexic symptoms are ego-syntonic without making much effort to find out why—at least from the perspective of the patients themselves. Belatedly, the field has become more curious, setting out to explore patients’ opinions through questionnaires (e.g., Vitousek et al., 1995; Ward et al., 1996; Blake et al., 1997; Rieger et al., 2000), structured interviews (e.g., Geller and Drab, 1999; Geller, 2002b), and a bit of qualitative research (e.g., Serpell et al., 1999; Surgenor et al., 2003). The results of the assessment research confirm the view that anorexic patients are more invested in retaining their symptoms than bulimic individuals—or patients with most other psychiatric disorders. Strategies for enhancing motivation have been proposed (e.g., Goldner et al., 1997; Treasure and Ward, 1997b; Vitousek et al., 1998; Kaplan and Garfinkel, 1999; Treasure and Bauer, 2003) and a few related interventions examined (e.g., Treasure et al., 1999; Feld et al., 2001). Most importantly, many clinicians are beginning to reconceptualize their task in therapy, accepting patients’ views as the necessary starting point for any efforts at change, rather than a particularly vexing byproduct of their psychopathology.
Of necessity, all existing treatment approaches for anorexia nervosa have adopted methods for handling resistance to change. The modalities outlined in preceding sections propose different—and sometimes opposite—tactics for accomplishing the shared goal of helping anorexics recover in spite of their reservations. There are basically three ways to go: (1) clinicians can try to override the desire to retain symptoms by making it difficult or impossible for symptoms to continue; (2) they can attempt to decrease the attachment indirectly by addressing the underlying problems it is presumed to reflect; and (3) they can make direct efforts to change patients’ attitudes about symptoms and recovery (Vitousek, 2005). Most modalities include some components fitting each of these descriptions; however, it may be useful to divide methods according to where they invest most of their therapeutic capital.
The ‘overriding’ approach is characteristic of inpatient weight restoration, parental control models of family therapy, and pharmacotherapy (when prescribing drugs for their weight gain side-effects). Indirect efforts to reduce the investment in symptoms are favored by psychodynamic therapy, IPT, narrative therapy, feminist therapy, and pharmacotherapy (when using medication to treat depression, anxiety, and/or obsessionality). Direct work on motivation is featured in CBT and to some extent in the psychodynamic variants that resemble it most closely, such as CAT and Bruch's ego-oriented approach. Again, it should be stressed that these divisions are not absolute; indeed, they cannot be. ‘Overriding’ methods must still enlist a degree of cooperation from the patient, unless she is very young or in imminent danger. Drugs can't work if the pharmacotherapist fails to convince the patient to take them. CBT and most (but not all) of the ‘indirect’ modalities agree that some forms of external control are indicated with some patients at some times, although they may work assiduously to keep the number of patients limited, the touch light, and the duration brief.
As noted in the review of modalities, there is still insufficient information to conclude which of these treatment packages works best with what subgroups of patients. At present, clinical decisions about how to address motivational issues must be based on some combination of each therapist's preferences and each patient's characteristics and circumstances. In the past, most clinicians opted for a blend of ‘overriding’ and ‘indirect’ methods when treating anorexia nervosa. In recent years, for a variety of philosophical and pragmatic reasons, there has been a clear trend toward the ‘direct’ approach. Increasingly, therapists are seeking ways to affect patients’ own views of their symptoms and the prospect of change—and discovering an unusual convergence of opinion about the strategies that further these goals. For ‘direct’ work on motivation, the same basic principles are recommended with reassuring reliability across different orientations and populations (Vitousek et al., 1998).
Notably, the eating disorder field has been influenced by exposure to motivational interviewing (MI; Miller and Rollnick, 1991, 2002). This approach was initially developed as an alternative to confrontational tactics for inducing alcoholic individuals to enter treatment. Miller and Rollnick argue that traditional methods of breaking down denial (such as highlighting the irrationality and danger of the symptomatic behavior, urging acceptance of the label ‘alcoholic,’ and insisting on the need for treatment) tend to backfire, paradoxically increasing the individual's investment in defending the status quo. MI uses a variety of strategies to heighten the salience of the patient's own concerns about the problem behavior, including reflection, affirmation of the patient's experience, emphasis on individual choice and control, exploration of personal values, amplification of discrepancies, and sharing of psychoeducational information. Most of all, the approach describes a stance toward treatment that is based on respect for the patient's perspective (Geller, 2002a)—along with the pragmatic recognition that in the end, the patient's opinions about the merits of change are the only ones that will determine the success or failure of attempted interventions.
The discovery of MI struck many in the eating disorder field with the force of revelation. Applications of the approach for anorexic and bulimic patients were outlined (e.g., Killick and Allen, 1997; Treasure and Ward, 1997b; Tantillo et al., 2001; Treasure and Schmidt, 2001), scores of training workshops delivered, and pretherapy motivational sessions added to treatment protocols in many specialty clinics. Therapists with a CBT background have welcomed the approach not because it represents a paradigm shift, but because its popularity has contributed to the wider dissemination of shared principles. MI is essentially a focused application of the Socratic style advocated in both general and disorder-specific models of CBT, usefully elaborated for the achievement of a particular objective during the initial phase of treatment. Many of the same strategies are featured in both approaches; for example, MI and CBT would be equally disposed to focus on exploring the ‘pros and cons’ of change (see Table 15.1), and outline precisely the same principles for using this technique (Miller and Rollnick, 1991, 2002; Vitousek and Orimoto, 1993; Vitousek et al., 1998).
In both approaches, review of the material shown in Table 15.1 is often the principal focus of initial sessions with a new patient. On one level, the exercise is transparent and straightforward: the therapist encourages the patient to share her views about the advantages and disadvantages of her disorder. Yet the simple exercise of reviewing perceived benefits and costs embodies many of the most central assumptions that these approaches share—and, when implemented correctly, offers a highly economical means of conveying them in the first hour of contact. By paying serious, sustained attention to what the patient thinks about being anorexic, the therapist communicates a number of important messages: her opinions are respected and her goals are important; she won't be forced to defend or to denounce her disorder; she will be treated as an individual rather than a predictable case of anorexia nervosa; she has the capacity to make active choices about her behavior; therapy is a collaborative process intended to help her find more rewarding ways to live in future.
Therapists should begin by asking patients what they like or value about their symptoms. By the time they enter treatment, individuals with anorexia nervosa are accustomed to being told what is wrong with what they are doing. Clinicians who depart from the script by asking them what feels right about anorexia are likely to learn considerably more about both sets of consequences, as experienced by the patients themselves. For example, Chloe started the first session by declaring that she was happy, healthy, and symptom-free, insisting that ‘everything would be totally fine if people would just stay out of my business.’ Rather than confronting Chloe with evidence that she was manifestly not ‘fine’ or enumerating the dangers she faced, her therapist encouraged her to describe what felt so good about anorexia that it counterbalanced the problems caused by outside interference. Chloe expounded eagerly on the rewards of thinness—and then, with little prompting from the therapist, began to divulge some of its drawbacks. By maintaining a curious, nonjudgmental tone about both sides of Chloe's experience, the therapist disinhibited much more self-disclosure of Chloe's own ambivalence than she had shared with other professionals.
The diversity of concerns expressed by anorexic patients is evident in the two examples charted in Table 15.1. Chloe's lists feature interpersonal considerations on both sides of the question: She values her thinness in part because it makes her attractive, enhances her status, elicits caretaking, and provides a distinctive identity—but it also troubles her that her disorder causes dissension, distresses her mother, decreases her privacy, and isolates her from friends. Amanda's concerns are more abstract and evaluative: Her ascetic life-style is virtuous, self-disciplined, productive, and safe—yet it seems to her simultaneously trivial, enervating, and, she fears, ultimately futile. These themes may (or may not) presage important issues to address in ongoing therapy; for the moment, they suggest ways to engage the patient's interest in getting it underway.
Throughout the process of reviewing pros and cons, it is crucial to remember the premise for the inquiry. The patient has been asked to share her own perspective on the rewards and costs of her symptoms. If the therapist asserts that a declared advantage is invalid, superficial, short-sighted, or ‘typically anorexic,’ the terms under which the patient chose to reveal her experience are violated. Any intimation that stated motives are not the ‘real’ reason for the disorder is also contrary to the spirit of the inquiry. At this stage of therapy, the patient's beliefs about her disorder are more important than its actual origins and effects (Miller and Rollnick, 1991). Her personal causal model may be inaccurate, and is always incomplete; however, its influence on her decision to stick with the status quo or experiment with change is not constrained by its validity (Vitousek et al., 1998).
While taking care not to dictate or dismiss patients’ views, the skilled MI or CBT therapist does much more than simply reflect and record them. Review of pros and cons often provides opportunities to insert psychoeducational material naturally and gracefully, so that didactic elements are less intrusive in the early phase of therapy. For example, when Chloe admitted that she felt cold all the time, her therapist took a minute to explain the phenomenon of starvation hypothermia—noting that one implication of this effect is that fewer calories are required to maintain weight. Common complications not mentioned by the patient can be introduced through the ‘hippocket patient’ technique: ‘I don't know whether you've experienced this at all, but another thing sometimes reported by people who have lost a lot of weight is that their hair begins to fall out—have you noticed that happening?’ This angle of approach is especially valuable for content that might be seen as unsympathetic, blameworthy, or bizarre. For example, if the therapist suspects a reluctance to admit to competitive motives, he or she might raise the topic as follows: ‘Some people say that they get a private sense of satisfaction out of knowing they can do something really tough that other folks don't have the will power to accomplish. Does that sound similar to how you've felt at times, or has your experience been different?’ It should be noted that in all instances the patient is offered the opportunity to endorse, reject, or modify the possibility proposed. Even if the content is acknowledged, its meaning and importance for the individual should be assessed rather than assumed.
Taking the patient's slate of perceived costs and benefits as a whole, one obvious question is whether the disorder seems like a good package deal. The calculations that determine the balance are not always logical—and certainly not additive, as a single powerful incentive may trump numerous liabilities (Miller and Rollnick, 1991). Clearly, it would be an error to conclude that as Chloe has listed more costs than benefits while Amanda identified an equal number of each, the former has become disaffected from her disorder and the latter is poised between two evenly weighted options.
If the patient attests that the status quo is preferable to the possibility of change, several lines of inquiry may be useful. While the balance of costs and benefits may be acceptable in the present, does she anticipate that it will remain so 5 or 10 years in the future? In her experience, has the ratio of advantages and disadvantages stayed constant over the course of her disorder, or has she noticed a trend toward diminishing returns? What plans has she considered for mitigating the costs she finds difficult to bear? If her eating disorder is working well, would she be pleased if her own daughter adopted the same strategy some day?
One of the most consistently helpful techniques is to frame the patient's dilemma by juxtaposing specific pros and cons she has identified. Almost without exception, lists such as those charted in Table 15.1 are full of internal inconsistencies. Chloe likes the attention she receives for her thinness, but hates it when people make a fuss about her weight and feels increasingly estranged from her friends. Amanda maintains that her disorder keeps her disciplined and diligent, but believes she would have accomplished more in her professional life in its absence; she prides herself on ‘eating right and being healthy,’ but has developed osteoporosis as a direct consequence of her diet; she believes that restriction makes her a ‘better person’ in moral terms, but recognizes that it has constricted and trivialized her concerns. Without going outside the patient's own system of goals and values, the therapist can highlight discrepancies between the objectives she hopes to fulfill through anorexia and her own assessment of its net effects: ‘So one reason that you value being thin is that it attracts a lot of attention from other people—yet on the other hand, you've noticed that you are lonelier and more isolated than you were before this started. That sounds like a real bind… What are your thoughts about why that might be happening?’ The patient is encouraged to begin exploring the possibility that different coping mechanisms might yield the desired outcomes at a substantially lower price. Most of the goals she seeks—such as self-control, emotional stability, and respect from others—are separable from the means she has relied on to achieve them; it is the means of food restriction and low weight that cannot be detached from their unwelcome consequences.
While the current enthusiasm for MI reflects an encouraging trend in the eating disorder field, two caveats are in order. The first is that clinicians who expect too little from the approach are unlikely to receive much more. Motivational work is often misconstrued as a nondirective form of counseling designed to help the patient sort through her options in a warm, accepting environment, so that she can pick the one that best suits her current stage of ‘readiness.’ Miller and Rollnick (1991, 2002) emphasize that MI is not simply empathic listening and reflection. It is, rather, a biased, systematic effort to accomplish a specific objective: a decision on the part of the patient to change the problematic behavior, followed by action consistent with that resolve. Both MI and CBT are trying to influence; the fact that they proceed more subtly than many other persuasive efforts simply increases the odds that they will succeed.
The other concern is that some therapists may expect more from brief, first-phase work on motivation than it can reasonably deliver. MI is usually conceptualized as a discrete intervention, delivered in one to five sessions preceding treatment proper. In contrast, CBT regards the emphasis on motivation as an integral, ongoing part of all treatment efforts. Particularly in the case of anorexia nervosa, resistance to change is not an initial barrier that is cleared as soon as patients are persuaded to enter treatment and begin the ‘real work’ of psychotherapy. In many ways, dealing with motivational issues is the real work of psychotherapy for this population, and should be considered in designing all of its elements (Vitousek, 2002).
Although attention to motivational issues is especially crucial in the treatment of anorexia nervosa, the same strategies can be extended to work with any clients in whom ambivalence is marked, including bulimic patients who are desperate to stop bingeing but reluctant to stop dieting and those who fear giving up a pattern that has provided some relief from negative self-awareness. In fact, these principles represent good therapeutic practice for all individuals with eating and weight concerns, with the need to implement them systematically increasing in proportion to patients’ investment in the status quo.
The ideal system would be one in which patients could be referred to the type and intensity of treatment that maximized their probability of success while minimizing the financial and personal costs of exposure to too much, too little, or the wrong sort of care. Unfortunately, even in the well-studied case of bulimia nervosa, the use of such a ‘matching’ strategy has been thwarted by the failure to find consistent predictors of treatment response (Wilson et al., 2000). A less elegant alternative is the stepped-care model, in which interventions of increasing cost, complexity, and/or intensity are delivered sequentially. In a pure stepped-care protocol, all patients are started off with the least expensive and intrusive treatment that is known to provide some benefit, even if it does not offer the best statistical chance for improvement (Garner and Needleman, 1997; Wilson et al., 2000). If patients do not respond, they are provided with progressively more intensive and specialized interventions until a successful result is achieved (or until the optimism or resources of the individual and/or treatment agency are depleted).
For several reasons, a stepped-care approach of some kind seems indicated for bulimia nervosa (Fairburn and Peveler, 1990; Fairburn et al., 1992; Carter and Fairburn, 1997; Garner and Needleman, 1997; Wilson et al., 2000; Birchall and Palmer, 2002; Fairburn, 2002a; Fairburn and Harrison, 2003). The two forms of psychotherapy (CBT and IPT) that have demonstrated effectiveness for this disorder are both complex treatments that specify 19 hours of individual contact time and require specialized training to deliver. The necessary expertise is unavailable in many locations; in other settings, cost containment measures discourage routine use of the full course of treatment. Moreover, in the case of bulimia nervosa, there is no clear empirical basis for advocating rapid, maximally intensive treatment at the moment of case detection, as duration may not influence the odds of recovery.
As noted in the section on CBT, several economical and readily disseminable alternatives have demonstrated effectiveness with some bulimic patients, including CBT-based self-help and brief psychoeducational group treatment. The low cost and widespread availability of these approaches make them appealing first steps on the treatment hierarchy, with patients who do not achieve a satisfactory response moving on to the ‘gold standard’ treatment of full CBT (or perhaps IPT). It should be noted, however, that the moderately encouraging data on abbreviated treatments do not provide direct support for a stepped-care strategy. Most of the studies have delivered a single brief treatment, such as self-help or group therapy, without following nonresponders through subsequent rounds of higher-level intervention to gauge the cumulative effect of successive treatments. Although symptom duration alone does not predict treatment response, it is certainly conceivable that repeated failures in less potent treatments might discourage some patients from persisting to forms of therapy that could have been helpful if provided from the outset (Garner and Needleman, 1997; Palmer, 2000).
In practice, few specialists would advocate the use of a stepped-care model that automatically initiated treatment at the lowest level for every patient. Guided self-help might be an excellent opening move in the case of Sharon, the 24-year-old woman with bulimia nervosa who is bingeing and purging at fairly low frequency, shows no significant psychopathology, has a strong support system, and is highly motivated to recover. Indeed, Sharon might well appreciate an intervention that imposed few demands on her work schedule and maximized her sense of autonomy and self-efficacy. In contrast, even in the absence of data to support a matching strategy, most clinicians would reject the option of low-level modalities for patients such as Emily. The severity of her bulimic symptoms suggests that such treatments would be futile—and interventions that are unlikely to work are not cost-effective if they are simply unnecessary preludes to further treatment. In addition, a number of clinical considerations discourage the use of self-help or minimal group treatment in Emily's case, including her social isolation, fluctuating motivation, and suicidal risk.
The field is many more years away from accumulating data of the kind and quality that would permit evidence-based stepped-care protocols for anorexia nervosa. At present, there is no ‘gold standard’ treatment to recommend, much less an empirically supported ‘first step’ or ‘follow-up’ intervention. Some features of anorexia do provide a rational basis for eliminating the lower levels of stepped-care models from consideration (Wilson et al., 2000). Self-help manuals are inappropriate for this population; indeed, programs written for other eating disorders typically caution underweight individuals not to ‘try this at home’ without professional assistance (Cooper, 1993; Fairburn, 1995). Group and psychoeducational strategies are seldom recommended as stand-alone treatments, and medication offers little or no benefit (Walsh, 2002a). In contrast to bulimia nervosa, there is a strong relationship between treatment delay and poor response (Eisler et al., 2000; Steinhausen, 2002); moreover, the medical complications associated with low weight status are clear contraindications for postponing effective treatment. In addition, these patients’ lack of motivation for change creates a different context for stepped-care decision making (Wilson et al., 2000).
There is no clinical or ethical basis for deferring research on the higher levels of the stepped-care hierarchy, however, and some compelling reasons to proceed. The most crucial priority is study of the indications for inpatient care. Some experts consider hospitalization the standard approach for the management of anorexia nervosa, exempting only mild cases of recent onset. Although inpatient refeeding is clearly indicated for patients who are medically compromised, there is little evidence that it confers long-term advantages that justify its routine or extended use. Moreover, some correlational evidence suggests that hospitalization may actually contribute to negative outcomes (Gowers et al., 2000; Ben-Tovim et al., 2001; Meads et al., 2001). Studies that randomly assign eligible patients to different levels and lengths of treatment are long overdue.
In spite of repeated attempts at treatment, eating disorders prove refractory in a substantial minority of patients. Few data are available on long-term outcome in bulimia nervosa. In anorexia nervosa, 20–25% of surviving patients still meet criteria for an eating disorder when reassessed one to two decades after the index treatment episode, while another sizeable subgroup is improved but symptomatic (Steinhausen et al., 1991; Strober et al., 1997; Zipfel et al., 2000; Steinhausen et al., 2002). Several studies have suggested that chronic patients reach a point of no return—or at least extremely rare return—approximately 10–15 years after the initial treatment contact (Theander, 1985; Strober et al., 1997; Lowe et al., 2001), with virtually none of those still unrecovered by that point crossing over to complete remission when reexamined years later.
No treatment studies have been designed exclusively for individuals with long histories of anorexia nervosa, although some projects include a high proportion of chronic patients (e.g., Dare et al., 2001; Pike et al., 2003). Thoughtful (and generally convergent) clinical recommendations are available for work with this population (e.g., Hall, 1982; Kalucy et al., 1985; Yager, 1995, 2002; Goldner et al., 1997; Geller et al., 2001a; Noordenbos et al., 2002). Most experts stress the importance of ‘steering a balance between expecting too much and too little’ (Yager, 2002, p. 346) from these individuals, who are often disheartened by previous treatment failures yet unwilling to take the behavioral steps essential to recovery. Many writers caution against coercive or overzealous interventions (Goldner et al., 1997; Rathner, 1998; Yager, 2002), warning that aggressive treatment may precipitate severe depression and suicide attempts (Kalucy et al., 1985; Garfinkel, 2002b) or drive patients away from the longer-term, slower-paced therapy from which they might be more likely to benefit. Moreover, even when treatment is successful in producing weight gain, the loss of anorexia nervosa can leave these isolated, constricted individuals feeling bereft, unable to find another organizing principle or sense of purpose to replace their disorder (Hall, 1982).
With some patients, the most helpful approach is the harm reduction model advised for resistant or intractable cases of substance abuse (Marlatt and Tapert, 1993). Using the empathic, collaborative style favored by MI and CBT, the therapist can encourage the patient to set and achieve more modest goals, such as stabilization at a low but safer weight, selection of a restrictive but balanced diet, and elimination of the most dangerous practices of laxative abuse, fluid restriction, frequent vomiting, and extreme exercise. Principles may also be drawn from the rehabilitative model used to support patients with other severe mental illnesses, which focuses on minimizing inpatient care and fostering participation in social and occupational activities (Goldner et al., 1997).
A harm abatement approach may be indicated as well for severe cases of bulimia nervosa that are unresponsive to sustained trials of high-quality, individually tailored treatment. Again, duration is less likely to be a relevant consideration, but extraordinarily high frequency and atypical reluctance to give up the bulimic pattern may contribute. In such instances, it might be reasonable to target eating small retained meals during the day and postponing binge episodes, working simultaneously on other treatment goals such as coping with negative affect and strengthening interpersonal connections.
The decision to use a management model should be reached slowly, reluctantly, and above all tentatively (Vitousek et al., 1998). Certainly, just as with the constructs of ‘readiness’ and ‘stages of change,’ there is a risk that clinicians may use ‘chronicity’ to give both themselves and their patients a pass, abandoning active treatment efforts in cases that are not intractable but merely difficult. In view of the early age of onset in anorexia nervosa, most persistently ill patients will qualify for ‘chronic’ status while still in their 20s—which leaves a lot of years ahead consigned to a very limited, very hungry, and very tired life. That is a steep price to pay for unwarranted therapeutic pessimism. Even in truly refractory cases, the hope of transformational change should never be extinguished (Palmer, 2000; Yager, 2002). Anecdotal accounts describe instances of recovery in patients who have been anorexic for more than 25 years—in one case, accomplishing symptom remission at the age of 67, after half a century of life as an anorexic (Noordenbos et al., 1998).
On one level, the treatment of eating disorder patients with a comorbid Axis I or II condition should not be considered a ‘special problem.’ Like the issue of resistance to change in anorexia nervosa, it is an expected rather than exceptional complication of work in this area. Anorexia and bulimia often co-occur with affective disorders, anxiety disorders, substance use disorders, and personality disorders (for reviews, see Wonderlich and Mitchell, 1997; Pearlstein, 2002 and O'Brien and Vincent, 2003). Specific rates vary widely across studies as a function of referral and recruitment patterns, assessment procedures, and changes in diagnostic criteria over time (Grilo et al., 2003; O'Brien and Vincent, 2003). It is clear, however, that in the majority of cases clinicians treating anorexic and bulimic patients will confront psychiatric profiles that include more than one symptom cluster. It is far less clear how treatments should be adapted to address those diverse clinical pictures.
An obvious point to underscore is that not all comorbidities are equally meaningful or problematic. In a sense, comorbidity with depression is built into severe eating disorders. Any individual who ate less than 1000 calories per day at a BMI of 14, like the chronically anorexic Amanda, would be depressed; no one who matched the behavioral pattern of the severely bulimic Emily could maintain a normal mood state. From that perspective, it is nonsensical to speak of treating depression before taking on the eating disorder—or even alongside management of the eating disorder. We treat depression by alleviating the eating disorder, and wait to discover what vestiges remain after it is resolved.
Other kinds of problems are less inevitably linked to eating and weight pathology, even though they frequently co-occur with such symptoms and are usually exacerbated by them. These may (or may not) need to be addressed directly. In some instances, such interventions should precede close focus on the eating disorder, as in the case of serious substance abuse or active psychosis. In general, however, it is preferable to defer the treatment of extraneous psychopathology unless it poses a significant barrier to work on the eating disorder, as anxiety, depression, and even maladaptive ‘personality’ patterns all tend to improve with amelioration of anorexia or bulimia (Wilson et al., 1997).
Comorbidity figures prominently in the current debate about the value of empirically supported treatments (e.g., Seligman, 1995). Clinicians often hold that research findings are of limited relevance to their own practice (Haas and Clopton, 2003), which includes complex, treatment-resistant cases not represented in the tidy samples selected for study in controlled trials. Wilson (1995, 1996, 1998a,b) makes a persuasive case that the opposite is true in the eating disorder field. Anorexic and bulimic patients referred to specialty services and treated in the context of research tend to be especially challenging cases, with severe eating disorder pathology, high levels of comorbidity, and a record of repeated failures in previous treatment attempts. For example, in one trial comparing CBT and IPT for bulimia nervosa, 37% of participants had at least one Axis II disorder and 22% currently met criteria for major depressive disorder (Agras et al., 2000). In addition, the record of lifetime psychiatric illness included rates of 53% for major depression, 23% for substance abuse or dependence, and 24% for anorexia nervosa.
Therapists are correct, however, that the research literature offers little guidance about how to assist patients with so much compound psychopathology that their eating disorder symptoms may rank second, third, or fourth on a list of priority treatment targets. The sample case of Emily matches this profile. Whether or not she would be accepted into a controlled trial would probably depend on the level of her fluctuating substance use and suicide risk at the time she is evaluated. If she does make it into a study, she is fairly likely to drop out before completion (just as she has dropped out of nonresearch treatments in the past); if she did persist, she is fairly unlikely to obtain full symptom control (just as she has failed to respond to a variety of previous interventions). As discussed in the section on CBT for bulimia, the fallacy arises when we assume that because patients like Emily do poorly in research treatments, they can only profit from different (and usually ‘deeper’) treatments guided by clinical judgment rather than empirical data (Wilson, 1995, 1996, 1998a,b). In fact, patients who fare poorly tend to do so across modalities, and there is no evidence that they do better when treated outside the context of research or with untested approaches.
Clearly, the field needs to experiment with more effective ways to help these severely impaired patients. One clinical approach is based on the assumption that individuals similar to Emily have a subtype of eating disorder termed ‘multi-impulsive bulimia,’ in which binge–purge behavior is associated with other patterns such as substance abuse, self-harm, sexual disinhibition, and shoplifting (Lacey and Evans, 1986; Lacey, 1993). An eclectic treatment program has been proposed for such cases, but has not yet been examined in controlled trials. Most experts construe this profile as a not-uncommon overlap between Axis I and Axis II pathology, and recommend combining treatments that have been validated for each. Recently, several specialists have described adaptations of dialectical BT (DBT; Linehan, 1993) for bulimia (Wiser and Telch, 1999; Safer et al., 2001a,b; Palmer and Birchall, 2003; Palmer et al., 2003). A clinical case series reported encouraging results using the full DBT program for treatment-resistant bulimic patients with comorbid borderline personality disorder (Palmer et al., 2003).
We have been reviewing features of the eating disorders and individual patients that make change difficult to accomplish; for balance, it is important to note that the attitudes and behaviors of clinicians can prove equally resistant to modification. Some persistent problems in this area include: (1) rejecting, patronizing, and punitive responses to eating disordered individuals; (2) denial of key dynamics that are theoretically inconvenient or clinically unsympathetic; (3) resort to the extremes of aggression or passivity; (4) stereotyping of anorexia and bulimia; (5) insensitivity to sociocultural context; (6) personal issues with eating and weight that interfere with optimal treatment; and (7) reluctance to change accustomed therapeutic practices.
Traditionally, the therapist–patient relationship is abysmal in anorexia nervosa (Garner and Bemis, 1982, 1985; Garner, 1985; Goldner et al., 1997; Beumont and Vandereycken, 1998; Kaplan and Garfinkel, 1999). A former anorexic patient wrote: ‘It is difficult not to gain the impression from the literature [on anorexia nervosa] that individual therapy has been devalued because (among other reasons) psychotherapists do not like anorexics, and anorexics do not like psychotherapists’ (MacLeod, 1982, p. 122).
MacLeod's impression of the antipathy aroused by people who share her diagnosis has been confirmed in surveys of therapists, physicians, and nurses (e.g., Brotman et al., 1984; Fleming and Szmukler, 1992; Burket and Schramm, 1995). Few symptom patterns evoke stronger negative reactions from professionals or create more dissension among treatment teams (Tinker and Ramer, 1983; Hamburg and Herzog, 1990).
A number of factors appear to contribute to the unsavory clinical reputation of anorexic patients, including the views that they are deceptive, manipulative, defiant, rigid, suspicious, and ungrateful for the efforts clinicians make on their behalf. Perhaps the most provocative element is the perception that these patients’ suffering is self-inflicted. Like individuals who abuse drugs or commit acts of self-harm, they become ineligible for compassion by taking part in the manufacture of pathology. The eating disorders are often regarded as ‘diseases of the will’ (Halleck, 1988), in which symptoms arise ‘because of stubbornness (anorexia) or lack of willpower (bulimia)’ (Beumont and Vandereycken, 1998). Across mental and physical illnesses, people who are considered able but unwilling to recover are viewed as having less ‘respectable’ and more blameworthy disorders (Halleck, 1988). These attitudes undoubtedly contribute to the occasional use of punitive interventions in this specialty area (Garner, 1985), and the much higher rate of contentious and controlling ones.
Ironically, some of the most impassioned pleas for more sensitive treatment are based on the same judgmental premise. Apparently sharing the view that patients would be culpable if they did contribute to their own pathology, many clinicians insist that they do not, casting anorexic patients as unwilling victims of an unwelcome disease. Although this construction is perhaps the most economical way for professionals to sustain ‘therapeutic’ attitudes toward difficult patients, it should not be confused with genuine empathy. Our goal must be to understand the complex experience of anorexia nervosa, not to distort it for the purpose of getting around the constraints on our own compassion.
Problems also arise from the fact that many eating-disordered beliefs are exaggerated versions of culturally-syntonic ideas (Garner and Bemis, 1985). Some clinicians (often, but not exclusively, male clinicians) are insensitive to the social context in which their patients are immersed; other therapists (often, but not exclusively, female therapists) run into trouble because they are susceptible to the same pressures—or have rejected those influences on political grounds and are frustrated that their clients succumb (Gutwill, 1994; Garner et al., 1997). There are numerous discussions in this area of the relative assets and handicaps of female and male therapists (e.g., Frankenburg, 1984; Wooley, 1991; Kopp, 1994; Stockwell and Dolan, 1994; Katzman and Waller, 1998; McVoy, 1998) and of clinicians with or without eating disorder histories (e.g., Kalucy et al., 1985; Jasper, 1993; Johnson, 2000). Whatever the therapist's sex, politics, personal background, or current weight, it is crucial that she or he is both attuned to the sociocultural environment that surrounds the eating disorders and sufficiently distanced from it to avoid transmitting mixed messages (Garner et al., 1997).
Like virtually every eating-disordered individual, all four patients profiled in this chapter could enumerate troubling encounters with professionals who seemed to endorse elements of their pathology. For example, a physician told the weight-suppressed bulimic patient Emily that her low BMI would be ideal if she could only manage to sustain it without vomiting five to 10 times per day; the dietitian to whom the young anorexic patient Chloe was sent applauded her avoidance of ‘junk food’ while suggesting that she increment her caloric intake with additional ‘healthy’ choices. In our view, whether or not therapists have had a clinical eating disorder in the past, it is also unacceptable for highly restrained or weight-conscious clinicians to work with bulimic or anorexic patients—not least because it is hypocritical.
After 20 years of treatment research, efforts to help individuals with bulimia nervosa can now be guided by information about what works best, fastest, and most reliably. Two very different forms of psychotherapy (CBT and IPT), as well as antidepressant medication, have been shown to benefit these patients. CBT is by far the most examined, supported, and endorsed approach. This treatment produces greater symptom reduction more rapidly in a higher percentage of patients than any other modality, and its effects have proven stable over time and robust across settings. Although CBT is by no means universally accepted (or even widely practiced, at least in its specified form), its influence can be gauged by the fact that CBT is a party to almost all of the active debates in this specialty area. Critics generally contend that we would do better in the treatment of bulimia if we shifted the focus of standard CBT or included additional elements; rarely, however, do they propose jettisoning the model in favor of a radically different approach. Similarly, the key questions in pharmacotherapy concern whether drugs can add to CBT or benefit the subset of CBT nonresponders.
There is still substantial room for improvement in the results obtained through CBT, and the next logical stages of research are proceeding with efforts to streamline the approach for patients who respond well and to broaden or supplement it for those who do not. At present, however, CBT stands not only as the best validated treatment for bulimia nervosa, but as one of the most thoughtfully investigated and strongly supported interventions across the psychological disorders. In many ways, progress in this relatively new specialty area is a model for how systematic research can enhance our understanding and treatment of psychopathology.
At the same time, the status of CBT for bulimia also illustrates a persistent problem in our discipline. Relatively few patients receive this effective treatment because most practitioners are neither inclined nor trained to use it (Wilson, 1998b; Crow et al., 1999; Fairburn, 2002a). One of the highest immediate priorities must be the development of more successful strategies for disseminating both information about the approach and the skills required to deliver it.
The situation is quite different in the case of anorexia nervosa, where no single treatment model is preeminent in either the empirical literature or clinical practice. The most discouraging commentary on the state of psychotherapy research is that there is remarkably little evidence to summarize. Few controlled trials have been attempted; some have broken down after a majority of patients dropped out or failed in treatment. Sample sizes are uniformly small, and results seldom replicated. As a result, the field sometimes draws unwarranted conclusions about what treatments work best for which patients on the basis of single studies that included eight to 10 participants per cell.
Unfortunately, the meager data we possess confirm the clinical impression that no known treatments work especially well, rapidly, or consistently for established cases of anorexia nervosa. Although it is clear that many anorexic individuals do recover and most improve, we have yet to identify psychological or pharmacological interventions that clearly contribute to the likelihood of a favorable outcome. Only a few conclusions are justified at present—and offer more guidance about treatments to avoid (dietary counseling alone, medication alone, methods that concentrate solely on underlying issues) than what approaches to adopt. In the persistent absence of data, ‘best practice’ standards for the treatment of anorexia nervosa continue to be defined by the ‘best guess’ opinions of experts rather than the ‘best evidence’ criteria of research.
While there are grounds for pessimism, it is much too soon for hopelessness. Because many individuals do overcome anorexia nervosa—and seem responsive to environmental factors rather than solely influenced by intrinsic disease processes—it is reasonable to surmise that we might be able to speed up recovery and perhaps change ultimate outcomes by varying what we do in treatment. A few dimensions that seem to make a difference have been identified. For example, it is desirable to intervene as soon as possible after onset; if patients are still adolescent, it is probably important to work with family members as well as the anorexic individual, although the optimal methods for doing so have yet to be identified; it appears preferable to see parents and patients separately, at least if a parental control model of therapy is used.
With older patients or those with a longer history of illness, the parameters of effective treatment are unclear, and the results likely to remain less satisfactory. In a backwards sort of way, however, the accumulation of data about the difficulty of modifying established anorexia nervosa should contribute to the design and delivery of more promising treatments. For example, in view of what we know about the nature of this disorder, it was not reasonable to anticipate that the minimalist 20-session treatments provided in some controlled trials would transform the attitudes and behavior of ambivalent patients with longstanding anorexia nervosa. Future studies should offer interventions that are better matched to the well-studied features of the disorder than the short-term and/or crisis-driven models of care often used. There is also increasing recognition that it is crucial to attend to the patient's own views about her symptoms and the prospect of change, and foolish to neglect either specific eating/weight-related behaviors or the broader context that makes them meaningful for the anorexic individual. Just as most psychodynamic therapists perceive a need for direct attention to symptoms, most CBT experts stress the importance of exploring their meaning and function. At least to some extent, anorexia nervosa seems to impose a degree of convergence on the factional field of psychotherapy. The high levels of agreement on a number of practice principles increase the confidence with which these can be recommended until more conclusive evidence is available.