Cognitive-behavioral therapy (CBT) for mood disorders is based on a cognitive theory of mood disorders with solid empirical foundations for its basic tenets, sets out principles that emerge from practice, theory, and research, and has been subjected to numerous outcome studies that have led it to be a ‘treatment of choice.’ CBT uses a combination of behavioral and cognitive techniques to help a person cope with symptoms, find better ways to deal with life problems, and to change the patterns of thinking, beliefs, and responses presumed to underlie the maintenance of depression (see A. T. Beck et al., 1979 for the seminal exposition; Moore and Garland, 2003, for more chronic and recurrent depression; Young et al., 2003, for schema-focused approaches). This chapter focuses primarily on a form of cognitive therapy developed by Professor Aaron T. Beck over 30 years ago and which has spawned a number of derivatives that address particular aspects (e.g., McCullough, 2000; Segal et al., 2002; Moore and Garland, 2003). We cannot do justice to the depth of clinical and research innovation and will therefore signpost key publications throughout the chapter and provide an ‘Indicated Reading List’ at the end of the chapter.
We first describe a case example and refer to this case throughout the chapter to illustrate CBT for mood disorders (see Box). We then describe the cognitive and behavioral theories that underpin CBT approaches for depression using this as the basis for describing the main therapeutic approaches to mood disorders as well as their evidence base. Key practice principles in CBT are applied specifically to mood disorders. Some common themes and issues in working as a CBT practitioner with clients with mood disorders are identified, discussed and illustrated through the case example. Finally, we set out future directions for CBT practitioners and researchers.
Mood disorders comprise affective, cognitive, behavioral, and somatic elements. In the case illustration of Sheryl (see Box) these were persistent low mood, guilt, and anhedonia (affective), negative automatic thoughts and ruminative thinking (cognitive), social withdrawal (behavioral), and sleep disturbance (somatic). Sheryl had suffered from mood disturbance throughout her adult life and had developed a range of negative beliefs about depression: ‘suffering depression is shameful,’ ‘my experience is unique,’ ‘nobody will understand,’ ‘this state will last forever,’ and ‘the future is bleak and hopeless.’
The family of mood disorders is a heterogeneous group of conditions that share in common mood regulation difficulties. The classification of mood disorders are described comprehensively in the Diagnostic and statistical manual of psychiatric disorders (DSM), 4th edn (American Psychiatric Association, 1994). We will refer to three broad groups of mood difficulties. The first, unipolar major depression, refers to an episode where mood is seriously compromised (e.g., at least 2 weeks of depressed mood or loss of interest/anhedonia) and evidence of four additional depressive symptoms (e.g., loss of energy, low self-worth, guilt, suicidal ideation, sleep disturbance, appetite disturbance). The second, bipolar depression is characterized by one or more manic or mixed episodes, usually accompanied by depressive episodes. The third, dysthymia refers to at least 2 years of depressed mood more days than not, accompanied by additional depressive symptoms that do not meet the threshold for major depression.
To date, CBT approaches have focused primarily on unipolar depression. However, the last 10 years has seen the development of CBT expertise for bipolar disorder (Basco and Rush, 1996; Newman et al., 2002) and more recently adaptations for atypical depression (Jarrett et al., 1999) and dysthymia (Arnow and Constantino, 2003).
Practitioners working with people with mood disorders draw several further distinctions that are important in understanding the presenting issues and in making treatment choices. The first distinction refers to the severity of disorder, which is usually mapped on to the continuum from mild to moderate to severe (with or without) psychotic features. The severity of the disorder is judged by the number of symptoms, the severity of particular symptoms, and the degree of functional impairment. A person with mild depression may report only five symptoms, each with mild presentations and producing little or no social or occupational disability. A person with severe depression may report most of the symptoms to a significant degree and may be incapacitated at home or in a psychiatric inpatient setting. This may include mood-congruent psychotic features such as delusions (e.g., of being punished) or hallucinations (e.g., berating voices).
A further distinction is whether the depression is the first episode or part of a recurrent pattern of depressive episodes. The diathesis-stress formulation and treatment of depression is probably different for these two presentations. Similarly, the age of first onset is important, as earlier onset is associated with more problems in adulthood, poorer prognosis, and greater likelihood of eventual suicide (Rao et al., 1999; Fombonne et al., 2001). In recurrent depression, the person's experience over time is important. Do episodes of depression arise through a gradual onset or more rapidly? Do the episodes last weeks, months, or even years? Is recovery gradual, sporadic or rapid? Between episodes does the person feel well and function fully or does s/he experience ongoing residual symptoms of depression?
The final categorizations that are sometimes used are of ‘chronic’ and ‘treatment-resistant/refractory’ depression. While nosologically contentious, some consensus exists that practitioners and researchers tend to use these to refer to the group of people who have unremitting depression that begins in adolescence/early adulthood and lasts over years (chronic depression) (McCullough, 2000; McCullough et al., 2003) or who do not respond to established evidence-based approaches.
These finer-grained categorizations are important because CBT theory and practice are adapted for different forms of depression. Therefore, through a thorough assessment process, a cognitive therapist would formulate diagnostic opinions that shape intervention choices (see Box for the diagnostic opinions for Sheryl).
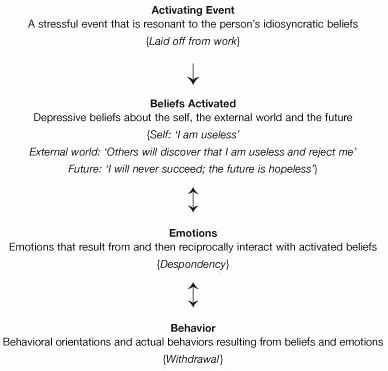
CBT theories of mood disorders move beyond description to explain and predict depressive phenomena. We cannot do full justice to CBT theories of depression here and interested readers are referred to recent reviews (see: A. T. Beck, 1996; Ingram et al., 1998; Clark et al., 1999). In brief, CBT theories of mood disorders are based on several assumptions. First, a diathesis-stress biopsychosocial model is implicated in the development and maintenance of emotional disorders. That is to say, biological, psychological, and social factors can all be involved in both diathesis, predisposing someone to mood disorders, as well as acting as stressors that precipitate the onset/relapse of mood disorders. Second, maladaptive beliefs about the self, the external world and the future are shaped through formative developmental experiences. Third, these maladaptive beliefs lie dormant and are activated only when precipitated by resonant situations. Fourth, when precipitating situations occur, the beliefs interact with the situation through processes of selective attention and inference, and generate negative mood reactions. These negative beliefs and emotions lead to behavioral consequences that serve to maintain negative mood (A. T. Beck, 1976b; A. T. Beck et al., 1979). Figure 11.1 shows this original model, and provides an illustration by describing a typical situation–belief–emotion–behavioral cycle for Sheryl.
Sheryl is a 44-year-old married woman, who presented with major, chronic, recurrent depression. A detailed assessment revealed an early onset of dysthymia at age 12 and a first episode of major depression at age 17. Her primary care physician has prescribed a selective serotonin reuptake inhibitor, which was augmented with lithium when Sheryl did not respond. She is currently unemployed, having been laid off 5 months ago from her job. Sheryl reports a difficult childhood, during which she felt little support or love from her parents. Her father suffered from depression and substance dependence, and died when she was aged 16 through suicide (although this information only became available some way through therapy). Sheryl has four children. Two of the children (male aged 23, female aged 23) were the children of her first husband who was alcohol dependent. He physically and sexually abused Sheryl, escalating to a point where Sheryl took refuge in a women's center. The younger two children (female aged 17 and male aged 12) are children by her second husband, with whom she currently lives. Her husband works as an engineer and she describes him as supportive.
Sheryl presented with the following issues: (1) increasing social withdrawal; (2) suicidal thoughts; (3) loss of her job and lack of success in finding a new job; (4) conflict with her 17-year old daughter; and (5) lack of self-worth. Sheryl's goals for therapy were: (1) to return to work; (2) increase her sense of self-worth; and (3) manage her daughter's problematic behavior more effectively.
The DSM-IV diagnostic impressions were as follows:
Axis I: major depressive episode, recurrent, severe; dysthymia (early onset)
Axis II: avoidant personality traits
Axis III: migraine
Axis IV: occupational problems (unemployed); economic problems (low income); other psychosocial problems (conflict with 17-year-old daughter)
Axis V: GAF (current): 55
GAF (highest in last year): 55
Use of standardized measures of depression severity, hopelessness and anxiety, Beck Depression Inventory-II, Beck Hopelessness Scale and Beck Anxiety Inventory suggested depression and hopelessness in the severe range and anxiety in the moderate range. Item analysis, with follow-up questioning suggested suicidal ideation but no suicidal intent. The assessment further indicated that that the onset of depression would be quite sudden, with Sheryl moving rapidly from normal functioning to feeling overwhelmed, often triggering a suicide attempt. On several occasions this had required hospitalization. Episodes tended to be of several months duration with a gradual recovery. Between episodes Sheryl was able to function normally, but careful assessment indicated that this was more apparent than real, with significant residual depressive symptoms that she did not disclose to others or indeed acknowledge fully to herself: fatigue, irritability, negative intrusive thoughts, and feelings of guilt.
Sheryl's nonresponsiveness to initial pharmacotherapy suggests combination CBT and pharmacotherapy as the next treatment approach.
This basic cognitive model has been significantly elaborated and refined on the basis of over 30 years of empirical work (see: Clark et al., 1999). One significant refinement is the suggestion that maladaptive cognitive processing, including negative beliefs, becomes activated only after the onset of depressive mood problems when dysphoric states are present (Miranda and Persons, 1988; Teasdale and Cox, 2001). In the onset and maintenance of mood disorders, depression is fuelled by a stream of negative ruminative automatic thoughts (e.g., ‘My high functioning façade is breaking down,’ ‘My family think I am weak,’ ‘I will be unable to cope with a family Christmas’) that are congruent with underlying higher-order modes (e.g., ‘self-as-weak’) and dysfunctional assumptions (e.g., ‘If my high functioning façade breaks down people will think I am weak’).
A second significant refinement is the concept of core modes that become activated in depression. Core modes are interlocking information processing systems that draw on the parallel processing from cognitive, affective, and sensory processing modules (Teasdale and Barnard, 1993; A. T. Beck, 1996). Once instated in depression, these core modes have a self-maintaining property as mode-consistent biases of attention, overgeneralized memories, higher-order self-schemas, ruminative thinking, and sensory feedback loops from unpleasant bodily states ‘interlock’ in self-perpetuating cycles of processing. The more often a person has suffered depression, the more easily these core modes become automatic and easily activated (Segal et al., 1996). The content of depressive core modes tends to be organized around themes of loss, defeat, failure, worthlessness, and unloveability.
Several theoretical reformulations argue that core modes are directly linked to depressive affective and motivational symptoms (Teasdale et al., 1993; Power and Dalgleish, 1997), while lower order maladaptive beliefs are linked to depression only indirectly through the core modes. Maladaptive beliefs are secondary dysfunctional assumptions (e.g., ‘I have to put on a strong façade, or people will reject me’), rules for living (e.g., ‘don't show weakness’), and attitudes (e.g., ‘weak people are pathetic’) that are closely linked to core modes (e.g., ‘self-as-weak’). Various commentators have noted this distinction between higher-order self-schemas and lower-order maladaptive beliefs as reflecting the difference between emotional and intellectual belief, ‘hot’ and ‘cold’ cognition (Teasdale, 1993; J. S. Beck, 1995; Young et al., 2003), or as clients have described it to us ‘I know it in my gut rather than in my head.’
|
|
Fig. 11.1 Illustration of basic cognitive model of depression, with case example. |
Related to core modes are cognitive and behavioral compensatory strategies that enable a person to cope with the negative consequences of core modes. The strategies are usually part of a spectrum of normal coping strategies but have become problematic because they have become inflexible and therefore inadvertently maintain core modes and maladaptive beliefs. In their most primitive form perceived threat triggers compensatory strategies to mobilize for action or inhibit into inaction. Examples of dimensions of compensatory strategies include:
avoid intimacy—appropriate intimacy—overly intimate
passive-aggressive—appropriate assertiveness—aggressiveness
abdicate control to others—appropriate use of control—authoritarianism
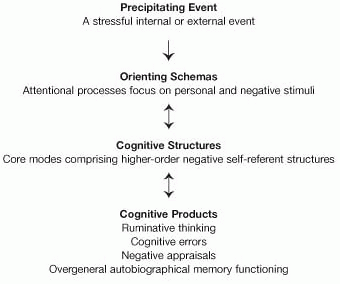
A table and schematic diagram summarize the reformulation of depression (Table 11.1 and Figure 11.2).
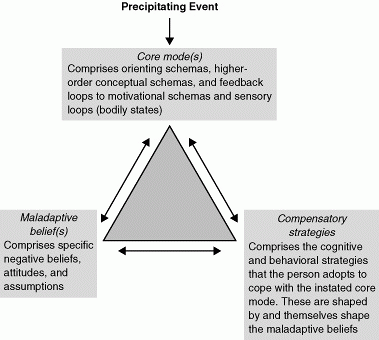
Activating events (internal or external) activate orienting schemas, which in turn activate the patterns of cognitive processing (dynamic cognitive structures) that are core modes or interlocked ‘minds-in-place.’ The cognitive features that make up depression (e.g., ruminative thinking, negative appraisals, memory biases) are produced once a negative core mode is instated. The characteristics and relationship between core modes, maladaptive beliefs, and compensatory strategies are shown in Table 11.1 and Figure 11.3.
In parallel with the emphasis on compensatory strategies in cognitive accounts, recent behavioral conceptualizations of depression have highlighted the importance of avoidant behaviors in depression, particularly within the behavioral activation (BA) approach. BA was initially developed as part of a component analysis of the active components of CBT, and only reflected the behavioral components of CBT (Jacobson et al., 2001; Hopko et al., 2003). After BA was found to be as effective as BA plus thought challenging and as effective as full CBT in treating major depression (Jacobson et al., 1996), the treatment was further elaborated (see: Martell et al., 2001), drawing on behavioral approaches to depression (e.g., Ferster, 1973). Central to the BA conceptualization of depression is the concept of secondary avoidant behaviors in response to the symptoms of depression produced by negative events: BA proposes that unhelpful secondary coping responses lead to the maintenance of depression. Typically, unhelpful secondary coping responses involve attempts to escape from an aversive environment (e.g., arguments, confrontations, reminders of loss) or to avoid aversive situations or emotional states (risk of failure or embarrassment), that is, secondary coping responses are compensatory strategies. Avoidance behaviors include being passive, withdrawal, rumination, complaining, or avoiding new activities. Because these behaviors reduce exposure to aversive situations they are negatively reinforced and become more prevalent, reducing the frequency and narrowing the range of other behaviors, which in turn reduces contact with positive reinforcers and increases the risk for depression.
|
|
Fig. 11.2 Cognitive model of depression. |
|
|
Fig. 11.3 Schematic diagram of cognitive reformulation of depression. |
|
Table 11.1 Core modes, dysfunctional assumptions, and compensatory strategies in depression
|
|||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
As in the original cognitive model for depression, cognitive approaches to bipolar disorder emphasize a diathesis-stress biopsychosocial model and focus on the importance of maladaptive beliefs and automatic thoughts. Although a comprehensive cognitive model of bipolar disorder is yet to be delineated, recent attempts to develop cognitive behavioral approaches for bipolar disorder have all focused on evidence suggesting that psychosocial stressors and adverse cognitive styles interact with an inherent biological vulnerability to produce manic and depressed episodes (Newman et al., 2002). The biological vulnerability appears in part to be hereditary, with bipolar disorder running in families, and genetic factors demonstrated in twin and adoption studies. Recent theories have suggested that biological vulnerability to bipolar disorder may result from dysregulation in the BA system, which is a putative neurobiological motivational system that regulates goal-directed approach to potential reward and is proposed to influence positive affect, energy, and attention.
Other evidence suggests that bipolar episodes occur in response to stressful life events, whether disruptions in daily routines (Malkoff-Schwartz et al., 1998), negative life events, or even goal attainment. Typically, it appears that negative life events predict bipolar depression, while goal attainment predicts mania; however, the relationship is not always straightforward, with negative events producing mania in the context of increased BA.
Cognitive-behavioral approaches to bipolar disorder emphasize that an individual's cognitive style and behavioral coping strategies in response to stressful life events mediates the extent to which the biological vulnerability is expressed in a full-blown bipolar episode. Consistent with this, Reilly-Harrington et al. (1999) report that negative attributional styles increase vulnerability to both manic and depressive symptoms following stressful life events.
Similarly, the response to prodromes of mania and depression is considered an important factor in the cognitive-behavioral model. Prodromes are the early signs and symptoms that can precede a full-blown episode, which the cognitive model assumes to be activated by the interaction between stressful life events and biological vulnerability. For example, disruptions in daily routine coupled with biological vulnerability may lead to reduced sleep. The cognitive-behavioral approach to bipolar disorder predicts that the particular thinking patterns and coping strategies instated in response to prodromal symptoms will determine whether a full bipolar episode will occur. As in models of unipolar depression, particular patterns of affect, cognition, and sensory input (e.g., depressed mood or hypomania) are hypothesized to activate associated schemas or core modes, which, in turn, will bias information processing towards information consistent with the schema, further fuelling the mood states. Thus, a patient in a hypomanic state will have positively valenced schemas activated, which will be characterized by processing that emphasizes goal attainment and potential rewards, while downplaying potential risks and problems. The particular schemas and modes that are activated in response to stress are hypothesized to determine which life events an individual will be more vulnerable to and to determine what form their response to stress will take. The activation of more adaptive, less extreme schemas and modes will lead to more stable mood, while less adaptive, more extreme schemas will produce further emotional dysregulation. For example, extreme beliefs about need for achievement and autonomy would be hypothesized to increase risk for depression and/or mania in patients with a biological vulnerability when exposed to potentially triggering events. In the case of perceived failure, such beliefs may lead to low self-worth and depressed mood, while in the context of perceived success such beliefs may lead to more grandiose thoughts about the self, feeding into hypomania.
Schemas and modes will also determine the strategies chosen to respond to stressful events and prodromes, e.g., achievement-related schemas would lead to overdriven behavior to compensate for lost time. Helpful coping strategies act against the prevailing prodrome, e.g., reduced arousal in hypomania, whereas unhelpful coping strategies further reinforce the initial stages of the bipolar episode, fuelling more extreme mood swings, e.g., rushing around doing many things at once (Lam et al., 2001). The specific schemas and modes available to be activated in any individual by stressful events or prodromes will depend upon his or her early learning history, as well as upon experiences in adolescence and adulthood, often linked to the onset and consequences of the bipolar disorder (e.g., beliefs such as ‘I am a difficult person’ and ‘I am defective’ following from the emotional fallout of mood swings).
Cognitive models of bipolar disorder also highlight the self-fulfilling nature of the disorder, with the consequences of a bipolar episode further contributing to the maintenance of the episode. For example, impulsive spending may lead to financial problems, irritability coupled with poor concentration may lead to problems at work or the loss of employment and promiscuous behavior may lead to problems in intimate relationships. All of these episode-related difficulties could then act as further stressors to interact with the underlying biological vulnerability to further generate bipolar symptoms. Furthermore, bipolar disorder is associated with a great deal of loss (e.g., lost potential, lost employment prospects, lost relationships), self-blame for impulsive acts committed during mania, and stigma, which can act as further stressors and/or further reinforce dysfunctional beliefs.
Thus, in summary, cognitive models of bipolar disorder emphasize: (1) underlying biological vulnerability (emotional dysregulation) and underlying cognitive vulnerability (dysfunctional schemas); (2) that these vulnerabilities interact with stressful life events to determine prodromes and patient's responses to prodromes; (3) less adaptive schemas will lead to less adaptive coping strategies and the exacerbation of prodromes into full-blown episodes; and (4) The consequences of episodes further exacerbate stressful life events and underlying cognitive vulnerabilities.
The advantages of these theoretical formulations to the CBT practitioner are that they introduce a more integrative model of mood disorders that provides clear rationales for why and how a broad range of CBT interventions might impact on cognition, behavior, and affect.
CBT has been demonstrated to be a generally effective treatment for depression in the large number of studies that have accumulated since the original study by Rush et al. (1977). CBT produces a greater improvement in symptoms than no treatment or waiting-list controls (Dobson, 1989) and demonstrates equivalent efficacy to pharmacotherapy for depression, although many studies did not employ a drug–placebo control condition or monitor plasma medication to check on the adequacy of pharmacotherapy (e.g., Blackburn et al., 1981; Hollon et al., 1992; Blackburn and Moore, 1997).
What about CBT compared with other psychotherapies? The large multisite National Institute of Mental Health (NIMH) Treatment of Depression Collaborative Research Program (TDCRP) trial (Elkin et al., 1989), which compared CBT, interpersonal psychotherapy, imipramine, and a placebo control, found that although there were few significant differences between treatments, for more people with more severe depression, pharmacotherapy and interpersonal therapy did better than CBT, with CBT only doing as well as placebo control on several outcome measures. This result has been much debated, with questions about differences in the skill in application of CBT across sites. Other studies comparing CBT with interpersonal or psychodynamic therapies for depression found CBT as effective as psychodynamic/interpersonal (PI) therapies (see: Leichsenring, 2001). However, the people in the NIMH-TDCRP study tended to have more severe depression than the other studies. More recent evidence attests to the efficacy of CBT for people diagnosed with depression, across a wide range of depression severity (DeRubeis et al., 1999).
One randomized controlled trial (RCT) compared CBT with BA (Jacobson et al., 1996; Gortner et al., 1998). The BA component of CBT focused on monitoring daily activities, assessment of pleasure and mastery, graded task assignment, cognitive rehearsal, problem solving, and social skills training. There were no significant differences between BA, BA plus modification of automatic thoughts (AT) and a full CBT treatment, at completion of treatment, 6-month follow-up (Jacobson et al., 1996), or 2-year follow-up (Gortner et al., 1998).
How well does CBT work for more chronic and severe depression? A recent trial examined CBT with and without nefazodone for chronic depression, operationalized as major depression lasting at least 2 years or a current major depression superimposed on preexisting dysthymia (Keller et al., 2000). This version of CBT, Cognitive-Behavioral Analysis System of Psychotherapy (CBASP) differs from classical CBT in its explicit focus on the consequences of client's interpersonal behavior through the use of a situational analysis protocol, which helps clients to identify whether their expectations and behaviors help or hinder movement towards their goals (see: McCullough, 2000). This trial found that CBASP and nefazodone in combination produced more remission in chronic depression (48%) than either nefazodone (29%) or CBASP alone (33%) (Keller et al., 2000). One limitation of this study was that treatment-resistant participants, that is, people who had not responded to previous antidepressants or psychotherapy, were excluded, i.e., the study lacked an important subgroup of chronic depression. Nonetheless, if replicated, this study would suggest that a combination of CBT and pharmacotherapy may be most appropriate for chronic depression.
One potential benefit of CBT for depression is that it reduces relapse/recurrence to a greater extent than antidepressant medication. Given that recurrence is a significant problem for people with major depression (Judd, 1997a,b), treatments that reduce relapse/recurrence are urgently needed. A number of studies report that after 1 or 2 years follow-up, relapse rates following treatment for depression with CBT were lower than for people treated with pharmacotherapy, when both treatments are stopped at termination (Kovacs et al., 1981; Simons et al., 1986; Evans et al., 1992; Shea et al., 1992; Gortner et al., 1998) (see also meta-analysis: Gloaguen et al., 1998). However, interpretation of these findings needs to be cautious because different studies used different criteria for relapse; Beck Depression Inventory scores greater than 16 or ‘treatment reentry for depression’ (Kovacs et al., 1981; Simons et al., 1986), compared with fulfilling criteria for major depression (Shea et al., 1992). Clearly, diagnosis of major depression is the most stringent criterion, while reentry into treatment is problematic as people in the CBT condition may still be symptomatic but attempting to deal with their symptoms themselves. Furthermore, an important comparison group is antidepressant continuation; people maintained on antidepressant appear to do as well as people who received a brief course of CBT (Evans et al., 1992). Blackburn and Moore (1997) in a randomized acute trial for recurrent major depression compared acute antidepressant treatment followed by maintenance antidepressants, acute CBT treatment followed by maintenance CBT and acute antidepressant treatment followed by maintenance CBT. All three groups showed clinical improvements during the acute and maintenance phases of treatment, with no significant differences between the three groups. CBT is therefore as effective in preventing the recurrence of depression as continued antidepressant medication.
More recently, several trials have specifically investigated the role of CBT treatments as relapse prevention for people whose depression was in remission rather than as an intervention for current depression. Fava et al. (1994, 1996, 1998) have developed a version of CBT to be used after successful treatment of an acute episode by pharmacotherapy. This therapy protocol involves a combination of CBT focused on residual symptoms of depression, life-style modification, and well-being therapy. Residual symptoms of depression are known to predict increased risk of relapse and therefore targeting such symptoms may well help reduce future episodes of depression. RCTs suggest that CBT for residual depression results in significantly less relapse/recurrence over 2 years (25%) than standard clinical management in the absence of antidepressant medication (Fava et al., 1998). Paykel et al. (1999) further demonstrated that compared with clinical management alone, clinical management plus CBT reduced relapse in 158 people with recent major depression that had partially remitted with antidepressant treatment.
An alternative approach to preventing relapse/recurrence has specifically targeted people with a history of recurrent depression who are currently in remission. Based on the hypothesis that these people tend to be caught up in ruminative depressive processing at times of potential relapse/recurrence, Teasdale et al. (1995) proposed that using mindfulness meditation, which fosters a relationship to thoughts and feelings antithetical to such rumination, might prevent future episodes of depression. Therefore, elements of a mindfulness-based stress reduction program (Kabat-Zinn, 1990) were incorporated into CBT to create mindfulness-based cognitive therapy (MBCT). MBCT is delivered in weekly group training sessions, in which participants practice and develop a moment-by-moment nonjudgmental awareness of sensations, thoughts, and feelings, through the use of formal and informal meditation exercises. These awareness exercises are further practiced during homework (see: Segal et al., 2002). For people with a history of three or more episodes of major depression, MBCT significantly reduced risk of relapse/recurrence over 1 year compared with treatment as usual (Teasdale et al., 2000). Without a further component trial, it is not possible to determine whether it was the mindfulness element or the CBT element or the combination thereof that was effective in this treatment.
In recent years, several RCTs have shown that compared with standard clinical management (including the prescription of mood stabilizers), standard clinical management plus CBT can reduce the recurrence of future bipolar episodes in people with bipolar disorder (e.g., Perry et al., 1999; Lam et al., 2000, 2003; Scott et al., 2001). These trials have focused on CBT as an adjunct to mood stabilizers.
Understanding the process and mechanisms of successful CBT for mood disorders is essential to developing more efficacious, more effective, and more appropriately targeted treatments for depression. The cognitive model (A. T. Beck, 1976a) predicts that CBT should produce specific changes on measures of cognitions, that these changes in cognitions are unique to CBT and that these changes in cognitions should predict symptomatic improvement.
One approach to testing this model is to examine changes on questionnaires designed to assess cognitive-specific changes, such as the Dysfunctional Attitude Scale (DAS: Weissman and Beck, 1978) and the Attributional Style Questionnaire (ASQ: Peterson et al., 1982). Several studies have found that people receiving pharmacotherapy for depression achieved similar changes in mood and cognitive processes as people receiving CBT, suggesting that cognitive changes were secondary to mood change (e.g., Imber et al., 1990). However, Seligman et al. (1988) found that CBT significantly improved explanatory style on the ASQ and that change in explanatory style correlated with change in depressive symptoms. However, without comparing CBT with other therapies, it was not possible to determine whether this change was unique to CBT or just secondary to symptomatic improvement. DeRubeis et al. (1990) found that change from pretreatment to mid-treatment on the ASQ and DAS predicted change in depression from mid-treatment to posttreatment for depressed patients in a CBT group but not in a pharmacotherapy group, suggesting that cognitive change is associated with improvement in CBT but is not alone sufficient to produce symptom relief.
There are general problems with the use of questionnaire measures to investigate cognitive change. Self-report responses are vulnerable to demand effects, response biases and the mood of the reporter may influence which items are endorsed, as many items differ in hedonic tone. Furthermore, it is not clear how well self-report questionnaires measure underlying cognitive structures and processes, such as schema, which are hypothesized to be important in the development of depression. There is also evidence to suggest that the specific cognitive biases associated with depression can only be observed when people are tested in a negative mood (Teasdale and Dent, 1987; Dent and Teasdale, 1988; Miranda et al., 1988).
More supportive of the cognitive change hypothesis, recent research found that a significant minority of people diagnosed with depression undergoing CBT showed ‘sudden gains’, where there was substantial symptom improvement in one between-session interval (Tang and DeRubeis, 1999). Such sudden gains are associated with better long-term outcomes, with people who experienced sudden gains significantly less depressed than those not experiencing sudden gains at 18-month follow-up. In CBT, sudden gains seemed to be preceded by critical sessions in which substantial cognitive changes occurred. However, as the sudden gains effect has recently been found in supportive-expressive psychotherapy for depression (Tang et al., 2002), the exact mechanism underpinning sudden gains (i.e., different mechanisms for different therapies versus nonspecific treatment effects) remains unresolved.
Recent studies have suggested that changes in the style of processing depression-related information, rather than just changes in thought content, might be important in the mechanism of CBT. Teasdale et al. (2001) found that in people with residual depression, CBT reduces an absolutist all-or-nothing thinking style, which, in turn, was found to mediate the effects of CBT on preventing relapse. Similarly, CBT successfully reduces relapse in people who report increased ‘metacognitive awareness’ at the end of treatment (defined as the ability to view thoughts as mental events in a wider context of awareness) (Teasdale et al., 2001). Thus, these studies suggest that CBT may prevent relapse by shifting the mode or style of processing. However, these studies have exclusively focused on residual depression with relapse as the outcome measure, leaving the generalizability of these findings to acute depression unresolved.
Interestingly, successful CBT for acute depression produces significantly greater reductions in ‘cognitive reactivity’ (operationalized as increases in dysfunctional attitudes following a negative mood induction) than successful pharmacotherapy for depression (Segal et al., 1999). Together with Teasdale et al.'s findings, this result is consistent with the notion that CBT helps people to acquire compensatory or metacognitive skills (Barber and DeRubeis, 1989) that regulate their cognitive responses to sad mood and stressful events.
An alternative approach to examining the process of change in CBT is to study the effects of specific techniques on outcome. Several therapy process-outcome studies suggest that homework is perceived as helpful and contributes significantly to change in cognitive therapy (Burns and Nolen-Hoeksema, 1991; Detweiler and Whisman, 1999; Burns and Spangler, 2000). Concrete symptom-focused methods of CT predict subsequent symptom reduction when assessed early in treatment (DeRubeis and Feeley, 1990). These concrete methods involved setting an agenda, asking for specific examples, labeling cognitive errors, examining evidence, and monitoring thoughts. However, less focused, more abstract approaches, such as exploring the meaning of thoughts and discussing the therapy, did not predict improvement.
What predicts whether someone will respond to CBT for depression (a prognostic indicator) and whether someone will respond better to CBT than to another treatment (a prescriptive indicator)? Various client variables predict poor outcome to CBT (see: Hamilton and Dobson, 2002), including increased severity and chronicity of the depression and perfectionistic beliefs (Shahar et al., 2003), although these variables predict poor outcome for all interventions. Married clients do better with CBT than single clients (Jarrett et al., 1991). People with avoidant personality disorder may respond better to CBT than to interpersonal therapies (Barber and Muenz, 1996), although higher levels of endorsement of avoidant beliefs predicts poorer outcome in CBT (Kuyken et al., 2001).
In summary, there is now a large and converging body of evidence to indicate that CBT is an effective acute treatment for unipolar depression and is an effective relapse prevention treatment for unipolar depression, and, potentially, a relapse prevention treatment for bipolar disorder. While early studies failed to show that changes in cognition precede symptom changes in CBT, more recent work suggests that sudden gains are preceded by important shifts in beliefs and that CBT effects changes in the process (rather than the content) of cognition. Process-outcome research suggests that CBT can be made more effective by explicitly and concretely teaching patients metacognitive skills in generating specific plans and evaluating their own thoughts.
Cognitive therapy for depression will follow the key practice principles of all CBT treatments (see Chapter 2 by Grant et al.). In the rest of this section, we will elaborate on how the key principles are applied to depression, using the case example of Sheryl as an illustration.
When treating depression, identifying, operationalizing, and prioritizing current problems and goals is a core aspect of therapy. Such goals direct the therapy and need to be reviewed regularly. These goals should be clear, mutually agreed, specific, and detailed in ways that are helpful to the therapy (including cognitive, affective, and behavioral elements). Identifying specific problems and goals can help patients to feel that their problems are more manageable and more optimistic about change. The problem and goal list for Sheryl are shown in the box and were reviewed at session 8, 16, and at the final session of therapy.
CBT case formulation has been defined as ‘as a coherent set of explanatory inferences about the factors causing and maintaining a person's presenting problems that is derived from cognitive theory of emotional disorders’ (Bieling and Kuyken, 2003) or as ‘the linchpin that holds theory and practice together’ (Butler, 1998). A case formulation should guide treatment and serve as a marker for change and as a structure for enabling practitioners to predict beliefs and behaviors that might interfere with the progress of therapy. The case formulation provides a psychological explanation that can help the therapist and client understand what is maintaining the depression and a clear rationale for intervention. There have been several attempts to provide individualized case formulation systems firmly based in cognitive theory that can be used by cognitive therapist in day-to-day practice and in treatment process and outcome research (Muran and Segal, 1992; Linehan, 1993; Persons, 1993; J. S. Beck, 1995; Needleman, 1999).
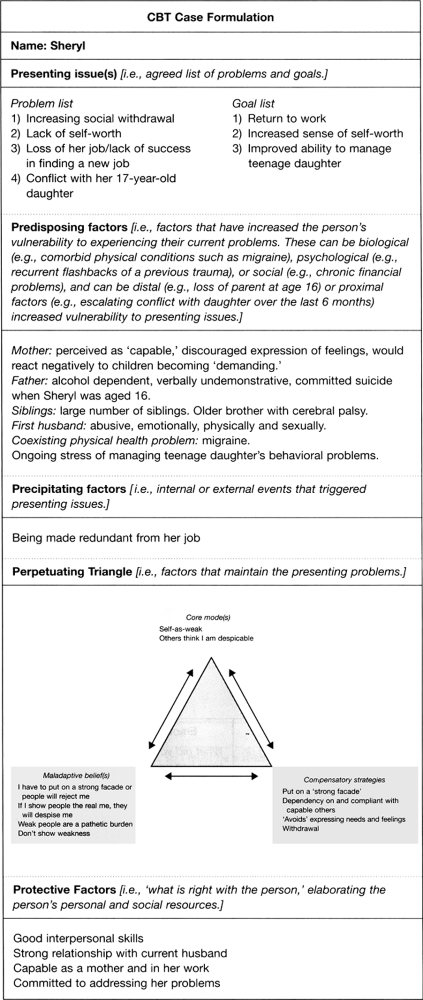
A CBT formulation rubric for clients with mood disorders makes use of the main elements of a standard case formulation as well as using cognitive theory in its explanatory elements (Figure 11.4). Standard case formulation rubrics describe: (1) the presenting issue(s); (2) predisposing factors; (3) precipitating factors; (4) perpetuating factors; and (5) protective factors. A general depression formulation rubric and the formulation for Sheryl are shown in Figure 11.4.
The formulation for Sheryl ties together in a coherent way how her presenting problems are explainable in CBT terms. It was essential to be able to explain her social withdrawal, low self-worth and conflict could be understood developmentally in terms of what had acted as predisposing and precipitating factors and crucially what core modes, dysfunctional assumptions, and compensatory strategies were maintaining her presenting problems. This formulation was continually revised and updated as new information became available and formed part of the rationale for intervention choices.
From the first meeting the client and therapist engage in a process of ‘collaborative empiricism’ (J. S. Beck, 1995). The therapist takes an active stance, supporting the client in working towards the therapy goals. The initial building of collaboration with Sheryl involved a preliminary description of her depression in biological, cognitive, behavioral, and affective terms (Greenberger and Padesky, 1995). With Sheryl describing her symptoms and the therapist mapping these out on a whiteboard it was possible to build a descriptive picture in CBT terms.
Cognitive therapy for depression typically involves 16–20 meetings, although brief versions have been developed for particular circumstances (e.g., Bond and Dryden, 2002) and more sessions are indicated for chronic and recurrent depression (e.g., Moore et al., 2003). Initial sessions tend to be frequent (either twice a week or weekly) to initiate the change process, manage suicide risk, and achieve symptom relief, and later sessions tend to be less frequent (monthly and perhaps even 3-monthly) to consolidate gains and prevent relapse.
|
|
Fig. 11.4 Cognitive-behavioral formulation diagram for depression. |
The first class of therapeutic approaches focus on the client's behavior. The rationale is that for some people behavior monitoring, BA, and behavioral change can lead to substantive gains. For example, people with more severe depression often become withdrawn and inactive, which can feed into and exacerbate depression. The person withdraws, and then labels him/herself as ‘ineffectual,’ thereby fuelling the depression. By focusing on this relationship and gradually increasing the person's sense of daily structure and participation in masterful and pleasurable activities the person can take the first steps in combating depression (A. T. Beck et al., 1979). Other behavioral strategies include scheduling pleasurable activities, breaking down large tasks (e.g., finding employment) into more manageable graded tasks (e.g., buying a newspaper with job advertisements, preparing a resume…), teaching relaxation skills, desensitizing a person to feared situations, role-playing, and assertiveness training. To maximize the likelihood of success, plans need to be operationalized at a very concrete, detailed level, including consideration of when, where, how, and with whom the plans will be implemented, as well as potential obstacles and how to overcome them. It is important to note that within CBT, these behavioral techniques are used with the ‘collaborative empiricism’ approach, such that before plans are implemented, thoughts and beliefs relevant to the activity (e.g., ‘It is pointless to try’, ‘I won't succeed’, ‘I am too tired’, ‘I am not interested’) can be set out as hypotheses to be tested. Recent adaptations to CBT suggest that the changes in behavioral contingencies may be particularly important in treating severe and recurrent depression (see: McCullough, 2000; Martell et al., 2001).
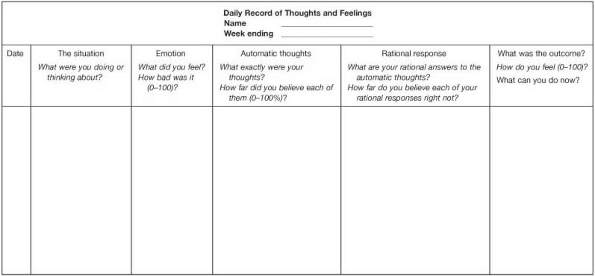
The second class of therapeutic approaches focus on the client's negative automatic thoughts and maladaptive beliefs. Cognitive techniques are designed to increase clients’ awareness of these thoughts, challenge them by evaluating their basis in reality, and providing more adaptive and realistic alternative thoughts. The Dysfunctional Thought Record is used as a primary tool for developing this skill (Figure 11.5). Repeated practice at dealing with negative thinking is required for thought challenging to become a robust skill. Useful approaches to challenging automatic thoughts include listing evidence from past experience that supports and refutes each hypothesis, generating alternative explanations, checking whether a thought may reflect a cognitive error, and reattributing negative events to factors other than the client's personal inadequacy.
|
|
Fig. 11.5 Dysfunctional thought record. From Beck, A. T., Rush, A. J., Shaw, B. F., and Emery, G. (1979). Cognitive therapy for depression. New York: Wiley. Copyright 1979 by Wiley. Reprinted with permission. |
In cognitive theory maladaptive beliefs (e.g., ‘If I drop my façade, others will despise me’) and higher-order core mode beliefs (e.g., ‘self-as-weak’) underlie automatic thoughts and are the next focus of cognitive interventions. Careful questioning about and exploration of client's unrealistic and maladaptive beliefs is carried out to examine if beliefs are based in reality, and to correct the distortions and maladaptive beliefs that perpetuate emotional distress. The advantages and disadvantages of the assumptions are explored and the possibility of adopting more functional, alternative rules is discussed. Early, often childhood, events that may have led to the adoption of these rules are explored and can be challenged, for example by using imagery to relive the event coupled with questions to introduce new perspectives. For Sheryl growing up in her family of origin a family maxim was ‘stiff upper lip’ or ‘don't show weakness.’ Behavioral plans designed to act against assumptions are a powerful way to change beliefs by providing personal experience that counters the assumption. For Sheryl this involved a process of applying the same standard to herself that she applied to other people, i.e., ‘a ‘capable’ person can be both strong and vulnerable and it is OK to show both these sides of the coin.’
Core modes require a further set of therapeutic strategies (J. S. Beck, 1995; Young et al., 2003). For example, when core modes such as ‘self-as-weak’ are identified, more adaptive beliefs (e.g., ‘I am basically capable and likeable’) can be established through Socratic questioning, examining advantages and disadvantages of the old and new core beliefs, acting ‘as if’ the new core beliefs were true, using coping cards, developing metaphors, subjecting the beliefs to tests across the person's life history and reconstructing associated memories and images (J. S. Beck, 1995). For many clients, automatic images, rather than thoughts, are powerfully associated with emotions and behaviors. Images are central to the sequelae of trauma and to psychiatric disorders such as posttraumatic stress disorder (PTSD) and other anxiety disorders that are often comorbid with depression. Images are handled in similar ways, but instead of verbally evaluating and challenging images, more visual techniques are used (J. S. Beck, 1995).
The third range of approaches takes place between therapy sessions as homework assignments. Homework is an essential element of cognitive therapy, aimed at building understanding and coping skills throughout the week, increasing self-reliance and rehearsing adaptive cognitive and behavioral skills. Homework moves the discussions in session from abstract, subjective discussion of issues to real day-to-day experiences. The therapist acts as coach, guiding and debriefing the client from week to week. Homework assignments are tailored to the individual, are set up as no-lose propositions, and may range from the therapist suggesting a relevant book, to the person undertaking a long procrastinated assignment (e.g., telephoning a friend to resolve an area of unspoken conflict), while monitoring the thoughts and images that come to light in preparing for the assignment (e.g., ‘the friend will be angry towards me’). As therapy progresses, the client takes on more responsibility for setting and reviewing the homework.
Having outlined the principles that underpin cognitive therapy, we aim to convey a sense of how cognitive therapy works in practice. We will outline a typical therapy session, as well as the progression of therapy as a whole, illustrating this through the case of Sheryl.
This involves checking how the client has been doing, reviewing the previous session, setting an agenda, working through the agenda items, setting homework, reviewing/summarizing the session, and eliciting feedback. The therapist will usually ask the client for a brief synopsis of the time since they last met, and as far as possible will try to enable a linking of both positive and negative experiences to thoughts and behaviors. For example, in one session when Sheryl's depression had moved from the severe to the moderate range, she attributed this change to ‘being able to see the depressive thinking as a part of the depression rather than as a part of me.’ A session would then review the homework from the previous session, again seeking to link progress or lack of progress to the therapy goals. For example, following session 1 Sheryl was asked to monitor her hour by hour activity, assigning mastery and pleasure scores (-5 to +5) to each activity. At the subsequent session Sheryl appeared demoralized and linked this to her diaries indicating that no event was associated with any mastery or pleasure. Having explored her meaning in more detail, this proved to be an opportunity to introduce the idea of depressive cognitive distortions (see Table 11.2): it became clear that she was discounting any positives (e.g., ‘anyone can get their kids to school in the morning’).
The session then moves on to the further agenda items. As they work through the items, the therapist and client seek to examine how the issues can be understood in terms of the cognitive formulation and how the issues relate to the therapeutic goals. Once there is a hypothesis about how the issue can be meaningfully understood, an appropriate intervention can be suggested. This is done collaboratively, with the therapist setting out the rationale and proceeding where there is a clear basis for collaboration. Sheryl's tendency to present a high functioning façade to her family was based on the belief ‘If I tell them how I feel they will think I am weak.’ Through collaborative empiricism and homework, it emerged that when Sheryl spoke to her husband about how she was feeling, he was understanding, amused (you're not as good at pretending as you think you are’) and relieved (it emerged that he lived in fear he would return home to find her following a suicide attempt). This sort of collaborative empiricism provides the basis for socializing to the cognitive model and the beginnings of thought challenging. As the therapist and client work through the agenda items, the therapist makes use of frequent capsule summaries. These serve to ensure therapist and client agree about what has been said, provides a chance to review the session as it proceeds and build a strong therapeutic relationship. Because people with mood disorders experience negatively distorted thinking, they may see the therapy and the therapist in negative ways (e.g., Sheryl would often say, ‘I don't deserve this help’). Capsule summaries can elicit these distortions and provide an opportunity to challenge this undermining negative thinking.
At the end of the session, the therapist asks the client for a summary of the session (e.g., ‘What do you think you can take away from today's session that might be useful to you?’). The therapist and client agree homework that will move the client on towards his or her goals and problem solve any anticipated difficulties with the homework. Finally, the therapist asks for any feedback, both positive and negative, on the session (e.g., ‘What did you like and not like about how today went so that we can ensure next time things are working well for you?’).
This might comprise four phases. The first involves ensuring a sound therapeutic relationship, socializing the client to cognitive therapy and establishing the problem/goal list. The therapist aims for some symptom relief very early (preferably in session 1), to build a sense of hope about the therapeutic process. With Sheryl this early phase was quite straightforward as she had been waiting some time to see a CBT therapist and had used this time to read a self-help book (Mind over mood, by Greenberger and Padesky, 1995) and to consider her goals for therapy. The CBT model made sense of her symptoms and this provided early relief from the experience of being overwhelmed by her symptoms. She also read several first person accounts of depression for people who suffer depression, which was helpful in making her feel less isolated and in countering some of her negative beliefs about depression (e.g., Lewis, 2002; McDonnell, 2003).*
|
Table 11.2 Cognitive distortions
|
||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The second phase involves behavioral strategies that will activate the client and begin to provide more significant symptom relief. This phase was more problematic because Sheryl tended to discount positive reinforcers and at difficult times passivity acted as a negative reinforcer. Changes in behavior for Sheryl operated in parallel with changes in beliefs. The third phase typically involves identifying and evaluating the client's thoughts and behaviors that are involved in maintaining the presenting problems. As appropriate, client and therapist work together to challenge maladaptive thought patterns (e.g., all-or-nothing thinking) and develop more adaptive ways of thinking. Similarly, maladaptive behaviors (e.g., avoidance) are identified, evaluated, and alternative behaviors are tried out. Sheryl described the main gains during this phase as a greater acceptance of ‘the committee meeting in my mind,’ regular use of thought records to break down and challenge negative thinking styles and the building up of alternative higher-order beliefs around ‘self-as-capable.’ An important aspect of this work involved dropping her high functioning façade and being able to ask for help when she needed it, and challenging the associated negative automatic thoughts (‘they'll think I'm pathetic’). The third and final phase of therapy focuses on relapse prevention. The goal of cognitive therapy is to enable clients to ‘become their own cognitive therapist,’ anticipating problematic situations, challenging their maladaptive thinking in these situations and experimenting with new and more adaptive ways of thinking and behaving. The therapist increasingly assumes the role of consultant to the ‘client cognitive therapist,’ reviewing what the client learned in therapy, reinforcing the client's effective problem solving, supporting the client in preparing for setbacks and supporting the client with learning effective problem-solving skills. Sessions tend to become less frequent and discontinue as the client and therapist have confidence that the therapeutic goals have substantively been attained and the client has the cognitive and behavioral skills to manage both everyday and anticipated future problems. The CBT case formulation should enable a good prediction of what future difficulties are most likely to prove problematic. This is used to rehearse how the client might manage these difficulties and thereby prevent future relapse if these difficulties occur.
Behavioral approaches to mood disorders are further elaborated in BA for depression (see: Martell et al., 2001). Practically, BA focuses on the context and functions of thoughts and behaviors rather than their form or content. The formulation for any client will be focused on variability and situatedness rather than stability, examining what differences in environment and behavior influence the client's feelings and their success at achieving goals. Every session the client and therapist will monitor the relationship between situation/action and mood and do a fine-grained analysis of day-to-day activity as it relates to mood.
For example, when making plans, it is useful to ask questions such as ‘Under what conditions have you failed and under what conditions have you not failed?’, and use the information arising to manipulate situational contingencies to maximize success. Similarly, when dealing with negative thoughts, BA focuses on their context and consequences rather than challenging them directly. Thus, if the thought ‘I'm a failure’ regularly occurs when a client is faced with a potentially difficult situation and has the consequence of stopping her from approaching and dealing with the situation, it may be hypothesized that the thought has the conditioned function of avoiding risk. In BA, a core aspect of therapy involves identifying these avoidance patterns, using the mnemonic TRAP (Trigger, Response, Avoidance Pattern) and coaching clients to get back on track by developing alternative coping using the mnemonic TRAC (Trigger, Response, Alternative Coping). In this case, the alternative coping would be to approach the feared situation despite the presence of the thought.
Changes in routine, such as sleeping late in the day, missing meals, and changes in patterns of social contact, can further maintain depressed mood, and, therefore, BA focuses on building clients back into more regular routines. To reduce passive coping and to increase awareness of the effects of behaviors on outcome, clients are encouraged to be proactive. In particular, clients are coached to act in line with their goals rather than their feelings. For example, if the goal was to have better self-esteem, the behaviors associated with better self-esteem would be determined in detail, e.g., more assertive, more eye contact, more erect and dignified posture, and plans made for the client to act out these behaviors as if they had better self-esteem. Clients are given the rationale that it is easier and faster to change their actions, over which they have direct control, which may in turn influence their feelings (to change from the ‘outside-in’), than to change their feelings in order to act differently (e.g., acting when it feels right, i.e., from the ‘inside-out’). Clients are encouraged to divorce action from their mood state and to learn that they rather than their mood can control their actions by acting even when they don't feel like acting.
Throughout BA, the mnemonic ‘ACTION’ is used to focus clients on the key principles:
Assess the function and context of a behavior
Choose to activate or avoid
Try out behavior chosen
Integrate behavior into a routine
Observe the outcome of the behavior
Never give up.
In BA the first sessions will be used to socialize into the model, provide a rationale and establish rapport. The main body of the sessions will use whatever behavioral approaches are appropriate to the idiosyncratic functional analysis of each client. The final sessions will work on relapse prevention by reviewing what has been learnt, reviewing patterns of avoidance identified and drawing up a response plan to maintain activation strategies.
* When recommended thoughtfully to clients (and therapists), these books can greatly increase understanding and hope by illustrating the feelings, thoughts, behaviors, and somatic features that make up ‘the territory of depression.’ Clients find them compelling because they are written by people who have experienced mood disorders first hand. For example, Gwyneth Lewis writes of her depression: ‘Under the duvet, an internal ice age had set in. I had permafrost around my heart. This is what dying of cold must be like, once the numbness has started’ (Lewis, 2002, p. 1).
CBT for bipolar disorder adapts the classic cognitive therapy approach for depression in several ways (see: Basco et al., 1996; Lam et al., 2000). First, there is psychoeducation explaining the diathesis-stress model, outlining the joint role of medication and psychological treatment in reducing acute episodes. Therapists help clients to recognize that bipolar disorder involves a biological vulnerability, perhaps in the form of heritable changes in brain chemistry, which interact with stress to produce episodes of mania or depression. Cognitive therapy is emphasized as a means of reducing stress by learning improved coping skills and through testing personal perceptions that can themselves be stressful (e.g., self-critical thoughts).
Second, clients are taught self-monitoring and self-regulation skills, with an emphasis on identification and early recognition of prodromes and development of good coping strategies in response to prodromes. An idiosyncratic evaluation of early, late, and middle warning signs of an impending episode are drawn up with each client and useful coping plans made for each symptom. Encouraging clients to keep daily activity schedules and mood charts can be very helpful in facilitating effective self-monitoring, and ensuring that potential episodes are caught early enough.
Typical prodromes for mania include reduced sleep/need for sleep, increased goal-directed activity, reduced anxiety, increased optimism, irritability, increased libido, increased sociability, racing thoughts, and distractibility. Typical prodromes for depression include reduced interest in people or activities, feeling sad or depressed, disturbed sleep, tiredness, low motivation, increased worry, and poor concentration. For mania prodromes, engaging in calming activities, increasing rest, reducing stimulation and decreasing activity would be useful strategies, whereas increasing levels of activity, enjoying the ‘high’, and ‘making up for lost time’ would be unhelpful strategies likely to increase the risk of a full-blown manic episode. Similarly, for depression prodromes, keeping busy and maintaining routines are associated with better outcomes, while cutting down on activities, withdrawing from other people and going to bed are associated with worse outcomes. For each client, an individual case formulation is required to determine the idiosyncratic prodromes and the most functional responses, as there is a great degree of individual variability. For example, some clients report changes in sensory experiences, such as colors becoming brighter or noises sharper, or increased pleasure at the sensation of moving at speed, when they are becoming hypomanic. For such clients, behavioral plans would need to modulate their experience of such sensations, e.g., pacing their exposure to stimulating environments such as art galleries, museums, shopping malls, and temporarily reducing travel by car, plane, or train.
Third, behavioral plans are made to promote good sleep and good daily routine, in recognition of the evidence that disruptions in sleep and working routine are implicated in the onset of bipolar episodes (Healy and Williams, 1989; Malkoff-Schwartz et al., 1998). Maintaining regular times to go to bed and get up, as well as meal times, can significantly help to stabilize mood. Clients learn to balance their activity schedules, not to do too much or too little, and to pace their own activities. The role of social activity needs to be carefully monitored and paced—social withdrawal is a warning sign for depression, while increased social contact can be overstimulating and feed into the development of mania. The roles of medication, substance, and alcohol use also need to be explored in detail with clients as potential risk factors for episodes. For a number of clients, discontinuation of their mood stabilizer is associated with the recurrence of a bipolar episode, as is very apparent from reviewing their life history—for these clients, explicit recognition of what their own experience tells them about the effectiveness of medication can be very productive. Given the high rates of alcohol and substance abuse in bipolar disorder, close monitoring of usage and explicit plans to keep use to a level that is not associated with the spiraling of mood is also important. As with all plans with bipolar clients, such plans need to be arrived at collaboratively and from an open exploration of the advantages/disadvantages of the options.
Fourth, as in CBT for unipolar depression, therapists challenge unhelpful automatic thoughts and clients use Daily Thought Records. However, as well as challenging negative thoughts associated with depression, therapists can also challenge excessively positive thoughts that may be involved in the development of mania. When focusing on hypomanic thoughts, it is important to be open, giving clients plenty of autonomy in their responses, as well as to review with clients the consequences of hypomanic thoughts, in order to overcome reluctance to dwell on positive thoughts. For example, clients can be taught to examine grandiose thoughts such as ‘I know better than everyone else’ and check whether these thoughts accurately reflect their past experience, and whether such thoughts are dependent upon their mood. Similarly, clients can be encouraged to examine the longer-term costs and benefits of their more-impulsive and grandiose thoughts. For example, questions such as ‘How many of your ideas still seem a good idea a week later? If this is genuinely a good idea, it should still be a good idea next week. Can you try and leave it for a week?’ can help to reduce impulsivity.
It is useful here to explore client's ambivalence about their manic episodes—many bipolar clients experience the initial stages of mania as positive, as they are no longer depressed, feel more confident, have more energy, and are more creative, but also report that more extreme mania is distressing because they feel out of control, act in self-destructive ways, and, in some cases, experience extreme anxiety and/or unpleasant psychotic experiences. As the cognitive model would expect, however, the information processing biases afforded by the hypomania mean that clients tend to focus on the positives of their mood state and forget the negative experience of the mania. Exploring both sides of the mania with clients in a Socratic way can be very helpful for facilitating rapport and for helping clients maintain the perspective necessary to motivate themselves to maintain therapy plans during an incipient hypomania.
Finally, as in standard CBT, therapy works to challenge dysfunctional assumptions that increase risk of relapse. Bipolar clients display the same dysfunctional assumptions as clients with unipolar major depression in the context of a depressed episode. However, bipolar clients also have more idiosyncratic assumptions centering on highly driven and extreme goal-attainment beliefs, e.g., ‘I should be happy all the time’, ‘If I put in enough effort, I should be able to achieve everything I want’. Bipolar clients with these attitudes are more likely to engage in extreme goal-pursuing behavior (‘trying to make up for lost time’), which is likely to disrupt their sleep and daily routines precipitating further episodes. Cognitive therapy can identify such beliefs collaboratively with clients and then explore how realistic and useful such beliefs are. Final sessions can also productively explore the losses and stigma that clients have incurred as a result of their illness and help clients to work through these issues, by grieving for these losses and developing more functional views. As the losses and stigma associated with bipolar disorder are genuine, Socratic questions more helpfully focus on people's approach to this reality (e.g., ‘What constructive lessons can I learn from my past?’ ‘How can I go forwards from here in a way that makes my life worthwhile?’), rather than by challenging the evidence for the losses. Clients’ own self-stigma can be challenged, particularly the relatively common beliefs that they are defective. Such beliefs often arose during adolescence when clients had difficult relationships with family and peers, as a consequence of mood swings that occur as the first manifestation of the illness. It is particularly helpful to refocus clients on their strengths and to encourage them to consider and pay attention to the multiple roles they occupy (e.g., parent, son, friend, worker) rather than exclusively focus on the label of bipolar disorder.
In this section, we will briefly consider what to do when faced with some of the most common difficulties and challenges that occur during CBT for depression, particularly when it is severe, chronic, and recurrent.
Suicidal thoughts, intentions, and suicidal attempts are common in depression and contribute to the significant mortality associated with depression (Brown et al., 2000). Furthermore, suicidal impulses fluctuate greatly and can rapidly and powerfully emerge in clients to even apparently minor setbacks. Thus, therapists need to be constantly alert for suicidal thoughts and plans, and for the concomitant hopelessness and sense of being trapped that often develops into suicidal thinking. Expressions suggestive of suicidal intent such as ‘I can't take it any more’, ‘It is all pointless’, changes in affect, such as increased calmness and resignation, and changes in behavior such as increased secretiveness should be explored. The Beck Hopelessness Scale provides an excellent measure of suicide risk and scores of 8 and above are associated with significantly increased risk of suicide attempts as well as eventual suicide (A. T. Beck et al., 1989). Suicidal intent and plans need to be directly and explicitly discussed with the client.
The first step in dealing with suicidal intent is to minimize the immediate risk of a suicide attempt. Reducing the risk will involve understanding the motives for wanting to attempt suicide. Typical motives include wanting to escape a situation that is perceived as intolerable and never going to change and/or attempting to engineer some interpersonal response, whether it be a ‘cry for help’ or an impulsive attempt to hurt others. Once the therapist and client are able to discuss the possible reasons for wanting to attempt suicide, with the therapist empathizing with the client's position, it is then possible to explore whether the situation is as intolerable and unchangeable as perceived. Socratic questioning can instill hope by helping clients to see that there might be alternative interpretations of their situation and that they have alternative options to deal with the problem. Drawing out both reasons for dying and reasons for living, including the advantages and disadvantages of each option, can help to produce a more objective view of the situation.
The most important practical step at this juncture is to work with clients on reducing their access to the means of killing themselves (e.g., pills, guns, etc.). As many suicidal attempts are impulsive, the simple expedient of removing the means significantly increases survival rates. A close analysis of previous attempts at suicide can reveal the series of events that escalate into a suicide attempt, and help to identify the decision points and key contingencies to target with further behavioral plans. For example, for many clients, the decision to try to reduce negative feelings through drugs or alcohol can be a critical step towards suicidal behavior. The therapeutic relationship is also an important tool, with therapists trying to keep clients involved and curious about the process of therapy and maintaining continuity between sessions, perhaps by explicitly asking the client to agree to not harm themselves in that time.
Once there is some progress at helping clients to consider the possibility of alternative views of their difficult situation, the next step is to facilitate problem solving in order to reduce the crisis or difficulties that contribute to the hopelessness. Problem solving is typically impaired in suicidal and depressed clients, and, thus, explicit attempts to define problems in specific detail and to work on generating alternative responses can be powerful.
As an active empirical therapy, it is important for therapists to monitor their client's progress—if after four to eight sessions of CBT, there seems to be no improvement, a comprehensive review is necessary. Several factors could conspire to impair improvement. First, the client may not be convinced by attempts at thought challenging. It is essential to check whether clients experience any changes in belief and emotion following a discussion of their thoughts. If there is no change, the therapist needs to explore what is maintaining the client's negative beliefs and what doubt's or objections he or she has about alternative interpretations or disconfirming evidence. It is also important to check that the challenging of thoughts is both emotive and experiential: that is, clients have their ‘hot’ cognitions activated, and the exploration of evidence and alternatives draws richly on their own personal experience rather than on dry abstractions. Second, it may be that the therapist is not being flexible enough and not selecting the approaches that best match the idiosyncratic concerns and abilities of the client. The more therapy can reflect and build from the client's own way of speaking, thinking, and acting, the more likely it is to be meaningful and helpful to the client.
Third, therapy may not work if it is not focused on the core problem or appropriate mechanisms identified in the formulation or if the formulation is incorrect. Careful assessment and formulation can help to avoid this difficulty and can remedy such an impasse when it occurs. However, depressed clients can be avoidant and find it difficult to share important information with a therapist because they find it shaming or have little trust of others. Turning to the example of Sheryl, there was little improvement in mood over the first six sessions, which focused on behavioral change with the intention of preparing her to return to work, even though she was making progress on this goal. Only in session 6 following the increased stress occasioned by her daughter's acting out and cutting, did Sheryl disclose her father's suicide when she was herself a teenager and the way that she felt shame and responsibility for his suicide. Her interpretations of this event and its implications for Sheryl's ongoing relationships (e.g., compliant, fearful of tipping others over the edge, perception of herself as weak and a burden) seemed central to her depression. Only when the formulation took into account this information did therapy begin to focus on core issues underlying her low self-worth.
The cognitions of the therapist are important in the progress of therapy, and, often, difficulties in therapy will be associated with, and exacerbated by unhelpful therapist thoughts. Unhelpful thoughts include therapists becoming too pessimistic about clients, therapists making negative interpretations of clients such as blaming them for not getting better, the therapist having self-critical thoughts about their own competence, and therapists having underlying assumptions of their own activated in therapy. It is important that therapists monitor their own thoughts and spend time reviewing them before and after therapy sessions, both individually, and, where possible, in supervision.
Depression is often associated with a past history of abuse or experience of trauma (Hill, 2003). Recent evidence suggests that CBT adapted for people with people with chronic depression and a history of early abuse is efficacious and superior to pharmacotherapy alone (Nemeroff et al., 2003). Histories of abuse can often lead to emotions such as shame and humiliation (see later section for more detail). Where clients have comorbid PTSD, adapting CBT for this disorder may make treatment more effective. Sheryl had distressing intrusive images of when her ex-husband raped her, which she found scary and shaming. Teaching her coping skills such as relaxation to deal with the strong feelings that accompanied these memories helped Sheryl to feel more confident about confronting these issues. The use of imaginal exposure coupled with cognitive restructuring was then used to work through and process the upsetting events.
Clients with chronic and severe depression often have difficulties with other people, including oversensitivity to other's responses, avoidant social behavior (e.g., reduced eye contact, submissive posture), passivity, anger, defensiveness, reduced assertiveness, and overly aggressive assertiveness. Furthermore, people with depression can elicit interpersonal cycles that maintain and accentuate their problems (Hammen, 2003). Therapists should be keenly tuned into how this might arise in the therapeutic relationship and seek to use this as further ‘grist to the mill’ for the cognitive-behavioral approach. For example, with Sheryl the therapist needed to monitor the risk of becoming overly controlling when Sheryl's behavior became passive and dependent. Skillfully noting these behavioral patterns, formulating the contingencies, and adopting an approach that leads to desired behavioral outcomes can provide a vehicle for change (McCullough, 2000). Furthermore, skillful use of feedback and capsule summaries will help develop a more accurate collaborative formulation of interpersonal-related cognitions and provide an opportunity to identify possible misinterpretations that therapists and clients are making.
Therapy also provides a forum for clients to practice changes in interpersonal behavior in a relatively safe environment, for example, less social avoidance, increased assertiveness, and disclosure of difficult feelings such as anger and self-hatred. Empathic, nonjudgmental yet ecologically valid responses from the therapist to these changes in behavior can be powerful learning experiences for clients, for example, discovering that one can be angry with someone else without them hating you. With Sheryl, a lot of her interpersonal difficulties came from finding it difficult to express her concerns and feelings to others. In her childhood, her parents had tended to discourage her from expressing her feelings and respond negatively when she did, to the extent that when her father killed himself, it strongly reinforced and exacerbated Sheryl's views that she should not express her feelings. With her teenage daughter, this meant that Sheryl was loath to express concerns and lay down rules, which in turn, led to further unhappiness when her daughter's behavior became unmanageable. Therapy focused on building up more assertive behaviors from Sheryl.
Many depressed clients suffer from an underlying negative view of the self, accompanied by destructive emotions such as shame and humiliation (Gilbert et al., 1996). These negative self-evaluations and the associated intense emotions are distressing to clients and often lead to interpersonal difficulties and dysfunctional behavior, by sapping motivation, increasing sensitivity to criticism, and by increasing passivity, avoidance and concealment. These difficulties will be manifest in therapy, interfering with forward therapeutic momentum. The depressed client who has an exaggerated sense of inferiority such as Sheryl (e.g., ‘self-as-weak,’ ‘Others think I am despicable,’ ‘I am worse than everyone else’) may well be loath to openly discuss their thoughts and feelings with a therapist, as this will be perceived as another shaming situation, confirming her personal inadequacy.
Low self-esteem is an overlapping construct with shame. In CBT, low self-esteem has been usefully conceptualized as a global negative self-judgment, which is further maintained by the adoption of dysfunctional rules of living, typically extreme rules for self-validation (e.g., ‘I need to do everything perfectly’), which in turn lead to unhelpful compensatory behaviors, such as avoidance, concealment of feelings and overvigilance for success and failure. With Sheryl, her extreme rules included ‘I need to make sure everyone else is happy’ ‘I should avoid upsetting other people at all costs’, leading to a hypervigilance for other people's emotional responses and a lack of assertiveness.
Similar treatment issues arise for shame, humiliation, and low self-esteem. First, the therapist has to be sensitive to the potential effects of their choice of words and their nonverbal body language on clients who are highly sensitive to perceived criticism and likely to respond defensively. The client's concerns and sense of shame/inferiority needs to be gently explored, with an implicit recognition and explicit acknowledgment that she may be keeping upsetting or shaming material back and may find it difficult to talk about certain events. Rather than forcing a client to talk about these difficult themes directly, it may be more useful to look at her predictions about what would happen if she disclosed her ‘secrets’, and to respond with empathic reflections about how difficult or painful she must be finding this. With Sheryl, she predicted that expressing how she really felt and talking about what had happened to her, would lead to other people rejecting her. Talking about her father's suicide and the rape by her ex-husband tested this belief in the session.
Behaviors maintaining low self-esteem and shame can be identified (e.g., looking out for failure rather than for success; safety behaviors that prevent clients from discovering that they are okay just being themselves) and reduced, and, in contrast, more positive behaviors encouraged. The advantages and disadvantages of holding on to feelings of shame and humiliation can also be discussed, particularly in reference to getting revenge.
For all these themes, particular techniques may be helpful: (1) using a positive data-log so that the client is deliberately focusing and recording their positive qualities, positive interactions, and positive achievements every day, to counterbalance their bias towards negative views of the self, and (2) reviewing evidence for and against the negative view of the self, particularly through behavioral experiments and through a detailed life review in which periods of the client's past are examined to see if there is any evidence against the negative view of themselves or alternative interpretations for negative events that previously supported the sense of worthlessness. With Sheryl, a detailed examination of her childhood and adolescence helped to generate alternative explanations for her parents lack of emotional warmth and support for her: (1) they were overwhelmed with caring for her siblings, including her older brother who suffered from cerebral palsy, and (2) her father and possibly also her mother were suffering from depression themselves. Examples of when she had close emotionally-open relationships with people were used to counter her negative self-beliefs—e.g., her close school friend, her good relationship with her grandmother. In the same way, the various factors contributing to her father's suicide could be more objectively evaluated. Such interventions often require experiential approaches including imagery and role-play and sessions need to be organized that there is sufficient time for intense emotions to settle before the session finished. Other useful approaches might include helping clients to focus on being compassionate and forgiving towards themselves.
The last three decades have seen CBT for mood disorders develop as a treatment of choice for unipolar depression and a promising intervention for bipolar disorder. We would predict that the next 25 years will see a range of exciting developments in CBT research and practice. In the area of outcome research, the most obvious area for advancement is where promising initial research suggests that CBT may prove to be an evidence-based approach: depression that is comorbid with personality disorders, PTSD, and substance misuse, dysthymia and bipolar disorder. Similarly, psychotherapy outcome research is needed to examine how cognitive therapy fares when it is adapted to different populations (e.g., older adults) and to different service settings (e.g., primary care). As we increasingly recognize depression as a potentially chronic relapsing condition, efforts to address depression in young people are urgently required. Given the scale of depression as a public health problem (Murray and Lopez, 1997), alternative formats (e.g., Internet-facilitated group therapy) are required.
In a climate of managed health care, evidence-based practice, and practice guidelines, researchers, practitioners, and policy makers are increasingly asking the question ‘What works best for whom?’. Beyond the comparative outcome studies, this sets the stage for interesting psychotherapy process and psychotherapy process outcome research. The mechanisms by which cognitive therapy is effective are not well understood, and this research will inform practice and health care policy. The stepped care approach to planning services and interventions is likely to be important here, as we become increasingly knowledgeable about what works for whom and through what mechanism. Cognitive therapy for depression is amenable to contemporary stepped care approaches, whereby clients are assessed and offered increasingly specialized, intensive, and complex interventions based on an algorithm of clinical need and optimal cost-effectiveness. Using the range of established cognitive therapy approaches, steps might graduate from bibliotherapy (Jamison and Scogin, 1995), to computer-based approaches (Wright et al., 2002), to brief psychoeducational approaches in primary care, to brief group approaches in secondary care to more in depth and extended individual or group cognitive therapy in either secondary or tertiary care (DeRubeis and Crits-Christoph, 1998).
The recent focus on primary and secondary prevention of mood disorders is welcome and there is much mileage in building on initial successes (e.g., Jaycox et al., 1994; Segal et al., 2002). The acceptability of cognitive therapy to many children and adolescents with depression and to people with recurrent depression combined with an increasing acknowledgment that primary and secondary prevention are high priority healthcare areas suggests we are likely to see much innovative and important work in this area.
Cognitive therapy is established as a mainstream psychotherapy of choice and training, supervision and accreditation are areas that require further development that extends and builds on existing best practice. There is an increasing body of cognitive therapy practitioners and researchers who are well placed to continue this work.