In this chapter we shall consider psychotherapy integration not just as a specific therapeutic modality, but also as a theoretical and research viewpoint that encompasses several of the distinct psychotherapeutic approaches reviewed in this section. Psychotherapy integration will thus be considered as a general ‘tendency’ within contemporary psychotherapy, and a modality in its own right.
We start by describing the historical background of psychotherapy integration. After defining the several theoretical approaches in psychotherapy integration, integrative treatment modalities and ‘common factors’ will be discussed. Some examples of clinical applications and empirical evidence on the effectiveness of treatment modalities will also be given.
In the opening address of the Second Psychoanalytic Congress in 1910, Freud stated that the psychoanalytic technique has to be altered in phobic patients, because ‘these patients cannot bring out the material necessary for resolving their phobia so long as they feel protected by obeying the condition which it lays down’. Only after they can do without the protection of their phobia, does ‘the material become accessible, which, when it has been mastered, leads to a solution of the phobia’ (Freud, 1910/1975, p. 145).
The integrative implication of Freud's comment is the possibility that the ‘protection of the phobia’ may not be removed by interpretation alone, and that a preliminary, concurrent, or even alternative approach involving exposure, may also be necessary.
Polarization of different psychotherapeutic camps, rivalry, misunderstanding, ‘straw-man-ism’, and dogmatic pseudocertainties have characterized battles between different psychotherapeutic modalities, especially between behaviorism and psychoanalysis. The fundamental theoretical antitheses lie between therapeutic monism and therapeutic eclecticism, and between specificity and universality (Karasu, 1986).
Therapeutic monism (called sectarianism by Karasu, 1986) is based on the premise that psychotherapeutic modalities have unique qualities differentiating them from other modalities. Each treatment modality, it is held, uses specific and unique therapeutic approaches, producing greater effectiveness compared with other methods, sometimes related to specific diagnostic categories or problems [e.g., cognitive-behavioral therapy (CBT) in obsessive-compulsive disorder, q.v.], or to effects not dealt with by other methods (e.g., psychoanalysis's view that it alone can bring about ‘structural’ as opposed to ‘symptomatic’ change).
At worst, therapeutic monism leads to: (1) downplaying the significance of interventions and processes that are relevant to all psychotherapeutic treatments; (2) Procrusteanism—i.e., offering potential patients only one type of treatment, irrespective of the presenting problem and personality of the sufferer, and withholding more appropriate treatments; and (3) splitting of the professional world, power struggles, and denigration other treatments.
Eclecticism, by contrast, is based on an empiricist view of treatment, and is concerned with developing ways of predicting change under specific circumstances irrespective of the model. Seeking the best treatment for the person and the problem, it is essentially pragmatic (Norcross and Newman, 1992). Dissatisfaction with ‘grand theories’ and technical procedures derived from these theories (‘a plague on all your houses’), as the motive force behind eclecticism (or technical eclecticism), is sometimes construed as atheoretical and even antitheoretical, leading to syncretism (the uncritical and unsystematic application of procedures; Norcross and Newman, 1992). Eclecticism distances itself from ‘schoolism’, and disavows any claims for itself as a separate school, but, rather, uses treatment interventions shown to be effective, irrespective of the particular theory from which they derive.
This chapter is not anti-‘monism’—indeed there is good evidence that therapists who stick to one model, albeit flexibly, get better results than either model-hopping eclecticists or rigid monists (Beutler and Consoli, 1992). Effective eclectic psychotherapy needs to be based on a thorough problem analysis and a well-founded treatment plan, leading to optimal use of various interventions. In short, neither monism nor eclecticism is contrary to good clinical practice, nor can either lay exclusive claim on effectiveness.
The specificity model is based on a natural science paradigm, and implies that under optimal circumstances, particular interventions will result in the intended effects. The universality model draws on anthropology and sociology and assumes that any socially sanctioned method of healing believed to be effective, and applied within a healing relationship by a healer to a sufferer seeking relief, may produce changes in feelings, attitudes, and behavior (Frank and Frank, 1991, pp. 2–3).
The model of psychotherapeutic specificity—or ‘drug metaphor’ (Shapiro, 1995)—in psychotherapy has provided the main paradigm for outcome studies in psychotherapy. Given that professionals are required to deliver psychotherapeutic treatments that are scientifically supported, to uphold professional standards, and to offer financially and ethically acceptable services, it is necessary to offer treatments of proven effectiveness. Governments, insurance companies, and patients increasingly insist on this.
Cognitive-behavioral therapists have led the way in using the specificity paradigm in psychotherapy. Methodologically sound studies, especially randomized controlled trials (RCT), of cognitive-behavioral treatments have shown that psychological therapies stand up well in comparison with drug treatments in psychiatry. This led the American Psychological Association's Society of Clinical Psychology's (Division 12) Task Forces (now the ‘Standing Committee of Science and Practice’) to develop lists of so-called ‘validated’ therapies (Task Force on Promotion and Dissemination of Psychological Procedures, 1995; Chambless et al., 1996, 1998; Chambless and Hollon, 1998).
Although the ideal of a list of ‘validated treatments’ was changed into the less definitive and dogmatic concept of ‘empirically supported therapies’, the work of the Standing Committee remains problematic (e.g., Lambert and Barley, 2002; Norcross, 2002a; Elliott et al., 2004; Lambert et al., 2004). It has inspired another APA Division Task Force (APA Division of Psychotherapy Task Force) to come up with a list of ‘empirically supported therapy relationships’ (Norcross, 2002a). This contrast between ‘therapy’ (i.e., a drug-like ‘pure’ treatment) and ‘relationship’ (i.e., a possible component of any effective therapy) vividly illustrates the antithesis between specificity and universality.
One of the more problematic aspects of the RCT model is that the evidence does not consistently or clearly show the superiority of one school over another (Lambert, 1992; Lambert and Bergin, 1994; Lambert and Ogles, 2004). Others, however, conclude that the way in which these critics used meta-analysis led them to a premature, or even false, determination that treatments are equally effective. For example, research techniques may not have been sophisticated enough to show differences in effectiveness, or similar outcomes may have been reached via different pathways.
Frank and others (Karasu, 1986; Frank and Frank, 1991) have argued that the crucial factor in any helping situation is the quality of the relationship between helper and recipient. The relationship is influenced by many factors. For patients these comprise, among others motivation, trust, hope, and idealization. In therapists, powers of suggestion, persuasion, warmth, empathy, involvement, directivity, and expert status. Interactional factors include contact, bond, agreement, rapport, and contract. Such interactional and relationship factors are important in every psychotherapeutic treatment.
In line with the ‘drug metaphor’ model these universal factors are viewed as ‘nonspecific’, because, in comparison with the specific factors, they are considered to be therapeutically neutral. However, here the drug metaphor breaks down, because both specific and nonspecific factors are based on psychological mechanisms (Lambert and Bergin, 1994; Lambert and Ogles, 2004). For instance, Lambert and Bergin (1994) showed that ‘placebo therapy’ (e.g., minimal attention) produces better outcomes than no-treatment or waiting-list controls. Nonspecific factors are often inadequately operationalized in placebo treatments, thus it is not clear to what extent ‘minimal attention’ compares with more intensive ‘specific’ attention. This leaves the question open how great the differences in effectiveness between active and ‘placebo’ treatments would be if nonspecific factors would be adequately defined, operationalized, trained, applied, and checked for adherence and competence (Arkowitz, 1992). Indeed, it would then be difficult still to view these factors as nonspecific instead of specific (Lambert and Bergin, 1994). In conclusion, it is inherently impossible for psychotherapeutic treatments to employ specific factors to the exclusion of nonspecific factors, and vice versa.
Another aspect has arisen from variance studies in treatment delivery in RCT. Initially these studies treated such differences as ‘error’ variance (Lambert, 1989; Lambert and Barley, 2002). Determined attempts were made to minimize individual differences between therapists within a treatment condition, e.g., by training therapists to offer the prescribed treatment using manuals, by supervision, and by monitoring adherence and competence. However, therapist variability appears to be the rule rather than the exception (Luborsky et al., 1985; Shapiro et al., 1989). For instance, Luborsky et al. (1985) found that interactional variables, especially the quality of the working alliance, were responsible for differences between therapies, more so than the quality of the individual therapies. The conclusion is that, irrespective of model, the role of the individual therapist and the working alliance with the patient cannot be neglected in psychotherapy (Lambert, 1989; Lambert and Barley, 2002).
These and other considerations have led to the redefining of nonspecific aspects of psychotherapy as ‘common factors’, i.e., those that were held in common by most or every psychotherapeutic treatment (Lambert and Ogles, 2004).
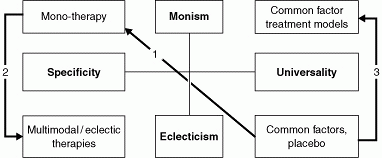
To summarize the argument so far, neither monism and specificity, nor eclecticism and universality can grasp clinical reality in its totality. A historical/ structural model can explain their various roles (see Figure 10.1).
|
|
Fig. 10.1 Psychotherapeutic models (after Karasu, 1986). |
Figure 10.1 shows that first, at the time of the founding of modern, scientific, ‘Western’ psychotherapy (to begin with Freud), common factors, originating in the prescientific era (Frank and Frank, 1991), were replaced by monistic (scientific) treatments of psychiatric disorders. Examples of this are psychoanalysis and CBT. Secondly, the plethora of these approaches gave rise to eclectic therapies. One example of this is multimodal therapy (Lazarus, 1976, 1989, 1992, 1997). Lastly, with the growing ‘postmodern’ scientific awareness of the importance of common factors and the realization that most so-called ‘monistic’ therapies in reality consist of a mixture of change-producing strategies, theoretical models were developed and new types of treatment were designed, including the Common Factor Model of Arkowitz (1992), interpersonal therapy (see Chapter 3 this volume), cognitive analytic therapy (CAT; Ryle, 1999), psychodynamic interpersonal therapy (Margison, 2002), the Cyclical Psychodynamic Model (Wachtel, 1997; Wachtel and Seckinger, 2001) among others.
The impact of different groups of interventions can be analyzed in this model. It is reasonable to assume that interventions from the monistic and the universal models are complementary. Thus specific interventions add value to the common factors and reinforce their effects (Strupp and Hadley, 1979). Equally, common factors reinforce the effects of specific interventions. Also, adding specific interventions derived from other models to a monomethodical approach may enhance the effects of the latter. In their turn, monomethodical approaches are necessary for the development of new interventions which then find their way into eclectic psychotherapies. There is currently an overall trend towards psychotherapy integration, or at least cross-fertilization, which advocates dialogue between theoreticians, researchers, and practitioners from different therapeutic orientations.
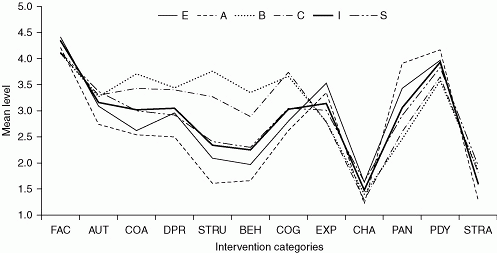
Surveys of therapists’ orientations show that integrative approaches are the most commonly practiced. Thus one-half to two-thirds of providers prefer to offer their clients a variety of interventions from major theoretical schools rather than a single modality (Lambert et al., 2004). A recent survey of Dutch psychotherapists (Trijsburg et al., in press) showed that therapists with various primary orientations used the full range of interventions to varying degrees. Figure 10.2 shows that subjects with a primary cognitive or behavioral orientation use more directive interventions than those with a primary client-centered, experiential, psychoanalytic, or psychodynamic orientation, whereas the latter use more nondirective interventions. Psychotherapists with a primary integrative and eclectic orientation are positioned in between and show a mixture of both nondirective and directive interventions. Importantly for our argument here, self-attributed monotherapists of all orientations appeared to use interventions derived from other theoretical schools.
|
|
Fig. 10.2 Mean scoring level of the intervention categories for six psychotherapeutic orientations. Reprinted from Trijsburg, R. W., Lietaer, G., Colijn, S., Abrahamse, R. M., Joosten, S., and Duivenvoorden, H. J. (2004). Construct validity of the Comprehensive Psychotherapeutic Interventions Rating Scale. Psychotherapy Research, 14, 346–66. A = Psychoanalytic–psychodynamic; B = Behavioral; C = Cognitive; E = Client-centered—experiential; I = Eclectic—integrative; S = Systemic; AUT, Authoritative support; BEH, Behavioral; CHA, Chair work (experiential procedures); COA, Coaching; COG, Cognitive; DB, Directive-Behavioral; DPR, Directive Process; EXP, Experiential; FAC, Facilitating; PAN, Psychoanalytic; PDY, Psychodynamic; STRA, Strategic; STRU, Structuring. |
Power emphasizes the ‘accidental’ nature of model-specific theories and interventions, and argues that free association and transference might just as well have been be applicable to CBT as to psychoanalysis had the history of psychotherapy been different. Similarly, Alford and Beck (1997) argue that CBT is as much an integrative as a monotherapy. Eclecticism is surveyed from a psychoanalytic perspective by Gabbard and Westen (2003) who describe a range of different interventions considered likely to produce change, including working not just with the unconscious and defense mechanisms, as in classical theory, but also with conscious conflicts and using such ‘facilitative’ strategies as support and humor which would be more likely to emerge from a cognitive therapy or humanistic background.
The trend toward eclectic and integrative psychotherapies is evidenced by the formation of societies that support the idea of psychotherapy integration (the Society for the Exploration of Psychotherapy Integration, SEPI and the Society of Psychotherapy Research, SPR), journals, and handbooks (Norcross and Goldfried, 1992; Stricker and Gold, 1993; Snyder and Ingram, 2000). Lambert et al. (2004) stated that the encyclopedic Handbook of psychotherapy and behavior change ‘has been eclectic from its inception in 1967 and its first publication by Bergin and Garfield in 1971’ (p. 7).
Norcross and Newman (1992) differentiated three forms of integration: technical eclecticism, theoretical integration, and the common factors approach. All three combine aspects of psychotherapeutic treatment originating from different sources.
Holmes and Bateman (2002) similarly differentiate organizational integration (making available a range of therapies so that the patient can be assigned to whatever fits his or her needs best), theoretical integration (showing how similar phenomena may be described in different languages, e.g., psychoanalysis's ‘internal objects’ and CBT's ‘schemata’), and practical integration (a pragmatic use of whatever therapeutic approach seems useful for a particular patient and problem). The latter, they argue, often characterizes the work of ‘mature clinicians’ of whatever basic persuasion, who feel free to borrow elements from other orientations when clinical need dictates.
Messer (1992) describes the latter as ‘assimilative integration’. This form of integration advocates a firm grounding in one system of psychotherapy and ‘a willingness to incorporate or assimilate, in a considered fashion, perspectives or practices from other schools’ (p. 151).
Below, we discuss technical eclecticism, theoretical integration, and the common factors approach. In each case we define the model, and give examples of treatment models and their applications. It has to be noted that most integrationists, e.g., Norcross and Newman (1992), stress the importance of combining specific interventions, shown to be effective in empirical research, with common factors in treatments. Nor are the three forms of integrationism mutually exclusive. Other aspects of integration, e.g., the combination of psychotherapy with drug therapy (q.v. Chapter 39), are discussed elsewhere in this volume.
Technical eclecticism is empirically oriented. Technical eclecticists combine different empirically supported interventions in any given treatment. Examples are the treatment models developed by (1) Beutler's systematic eclectic psychotherapy (SEP; e.g., Beutler and Consoli, 1992; Beutler and Harwood, 2000; Beutler et al., 2002a), and (2) Lazarus’ multimodal therapy (e.g., Lazarus, 1976, 1989, 1992, 1997). Essentially, different practical approaches are used and combined without adopting wholesale the theoretical model behind these interventions.
Beutler's SEP starts from the need for pragmatic forms of eclectic treatments and is based on the belief that different interventions are effective for different types of patients in different phases of treatment. It seeks its inspiration in clinical practice, empirical research, and the philosophy ‘that psychotherapy is a social-influence or persuasion process in which the therapist's operational theory forms the content of what is persuaded, and the therapist's technology functions as the means of influence. The quality of the therapeutic relationship is thought to define the limiting influence of the procedures used’ (Beutler and Consoli, 1992, p. 266).
Essentially, SEP represents a model of treatment selection that encompasses both established common factors as well as specific procedures. It formulates indications and contraindications for the application of these procedures. SEP contends that operational theories from different origins are applicable in different types of patients, provided that such theories permit the therapist to offer the patient an explanation of change, a perspective on change, and treatment goals that can be reached. One advantage of this approach is that theoretical integration at the explanatory level is not necessary; instead the theoretical (explanatory) considerations will have to be translated into the (descriptive) language of social persuasion theory.
The model emphasizes:
Matching of patient and therapist. SEP states that some communalities in the backgrounds of therapists and patients are necessary for patients to develop initial trust in the therapist. Equally, differences of viewpoint matter, in that it is through difference that new experience arises. Also, the severity of problems is important in formulating a treatment plan, as the initial patient motivation is directly dependent on the extent to which suffering is acute and immediate or long term and chronic.
Tailoring procedures to patient characteristics. Special attention is given to the reactance and the coping style of patients, in deciding how directive, or exploratory to be. Thus more extravert practically oriented patients may respond better to a directive style, while the reverse is true for introverted people (Beutler et al., 2002a).
Strategic change. For therapy to be successful, SEP states that intermediate goals (e.g., fostering the working alliance, identification of patterns in behavior, thoughts, feelings, and interpersonal relationships, change efforts, and termination) need to lead to structural change in the patient's psyche and that these in turn need to be reflected in changes in behavior and relationships.
Mr A, a 48-year-old married man asked for help ostensibly in order to ‘work through some issues from the past’. In fact he had been feeling depressed for at least a year, and was unhappy in his 25-year-old marriage. He stated that he felt angry with, and controlled by, his wife, and seriously was considering leaving her.
He was an only child, brought up by a single mother, who married when he was 10 to a stepfather who had no time for Mr A. At 16 he left home to join the armed services. He felt that he had been dominated by his mother and always had to do her bidding, and the same pattern repeated itself in his marriage. When, several years previously, his wife had an affair he decided he would do anything to keep her, and took responsibility for what happened on the grounds that he had been neglecting her.
The assessment interview focused on his chronically low self-esteem, difficulty in asserting himself, anxious attachment to the insecure base of his mother and then his wife, and unresolved oedipal conflicts around separation from the mother figure in the absence of a ‘good enough father’ with whom to identify.
The early sessions of therapy included systemic therapy techniques in the form of role-play, in which Mr A rehearsed what he would like to say to his wife. His compliance and dependency were evident in that it was clear that he was asking her permission to leave, even though he was well aware she wanted the marriage to survive. Using a cognitive therapy technique he was asked as homework to list on paper the pros and cons of asking his wife's permission for something basically unpalatable to her.
The therapist also felt that Mr A was unhappy with role-play, but went along with it in a compliant slightly sulky fashion, reminiscent of his attitude to those in authority.
This countertransference response—a psychoanalytic concept—was then used to illustrate Mr A's hostile dependency, a theme that he worked on in subsequent sessions.
Therapy was eclectic in the sense that techniques from three distinct therapeutic techniques were combined in order to produce an appropriate ‘tailor-made’ therapy for this patient. He needed help in his immediate marital crisis (systemic); he needed to understand the dynamics underlying his long-term relationship difficulties (psychoanalytic); and he needed the structure provided by a homework assignment (CBT). These approaches were synergistic in the sense that dynamic themes manifested themselves in the way in which Mr A responded to the systemic and cognitive-behavioral interventions.
Colijn (1995) uses a culinary metaphor to explain the difference between eclecticism and integrationism: eclectic therapists assemble a meal by putting together different dishes on one plate, whereas integrationists will create a new dish, based on several ingredients (p. 436). Thus theoretic integration draws on apparently antithetical existing theories, but synthesizes them to produces a new structure with its own theoretical basis. Examples of this are Ryle's CAT (Ryle, 1990), Wachtel's integration of psychoanalytical and behavioral treatment in the ‘Cyclical Psychodynamic’ model (Wachtel, 1997), and the transtheoretical model of Prochaska (e.g., Prochaska and DiClemente, 1992; Prochaska and Norcross, 2002).
Ryle (1990) decided to bring together the best of cognitive-behavior and psychoanalytic practice into a well-structured time-limited therapy applicable for work in third-party funded settings. Key features of CAT include:
The use of the ‘psychotherapy file’, a pen and paper form filled in by the patient, which aims to identify ‘snags, traps, and dilemmas’ that have led to the need for help. For example, a dilemma relevant to Mr A above might encapsulate dysfunctional dichotomous thinking such as ‘either I am submissive, stay close to those that matter to me, but must bend to their will, or I assert myself but run the risk of antagonizing those I love and ending up alone’.
An initial four-session assessment phase at the end of which a written and diagrammatic formulation is arrived at collaboratively between patient and therapist. This ‘sequential diagrammatic formulation’, unique to CAT, is based on the idea that neurotic procedures are often self-sustaining. For example, someone whose core belief is that they are unlovable will shy away from close involvement with others and thus reinforce his view that no one cares about him. The importance of the CAT diagram is that it shows the patient in ‘black and white’ what they are up to, and also how their own attitudes contribute to the problem that hitherto has been attributed either to a hostile world or to malevolent fate.
Homework assignments between sessions, with analogue scales agreed between therapist and patient to monitor progress.
A nondirective atmosphere in the sessions in which the therapist responds to whatever material the patient brings.
The use of transference and countertransference to identify ‘reciprocal role relationships’—i.e., an attachment/object-relations model in which the patient occupies one of a limited range of relational strategies such as victim/abuser, placator/bully, isolate/clinger. Mr A might well describe have described himself as assuming a placatory/secretly resentful role. Therapy then tries to help extend the range of possibilities, in CAT terminology called ‘exits’, in Mr A's case to find ways to be assertive but not enraged.
A strong emphasis on working through termination, after 16 or 24 sessions, culminating in a collaborative ‘good-bye’ letter summarizing the course of therapy, its achievements and work for the future.
Thus CAT brings together elements from CBT (1, 2, 3 above) and psychoanalysis (4, 5), but also adds its own theoretical and practical stamp. The shared formulation and goodbye letters are unique to CAT, as are the notion of reciprocal role procedures, and a psycholinguistic emphasis on the ‘interpersonal gesture’ and finding a language to name it.
The discussion of CAT raises the question of at what point a therapy ceases to be ‘integrative’ and becomes a ‘monotherapy’ in its own right. A comparable case might be that of dialectical behavior therapy (DBT, q.v.), designed originally to reduce self-harming borderline personality disorder. DBT uses ideas derived from behavior therapy, CBT, and Zen Buddhism, but is in fact a highly prescribed set of therapeutic procedures specific to itself.
The model of cyclical psychodynamics (Wachtel, 1997) was originally conceptualized as a way to bring together cognitive-behaviorist and psychoanalytical points of view, but was later extended to incorporate systemic, and even social and cultural dimensions. The model focuses on the vicious circles originating in early childhood experiences, and investigates the ways in which these patterns are reinforced in actual daily life.
Mr J came into therapy with a presenting problem of a pigeon phobia. Because pigeons are ubiquitous in New York, almost every dimension of Mr J's social and professional life was affected by his phobia. Avoiding pigeons was almost a full-time occupation. As a consequence of his phobia, Mr J was severely limited in both his social and occupational activities. He was not completely socially isolated, but he had a ready-made excuse whenever he felt the slightest bit anxious about socializing. The limitations and restrictions in his life could thereby be experienced by him not as a product of deeper anxieties, which he was initially quite hesitant to approach, but as an unfortunate side-effect of his pigeon phobia.
In exploring the origins of Mr J's pigeon phobia, Mr J's earliest relevant memory was not directly about pigeons but about a parakeet, a friend's pet that had bitten him when he was about 9 years of age. The event was not experienced as significant at the time (it was just a minor nip), but about 6 months later Mr J began to show signs of anxiety around birds in general, which before long became a terror specifically of pigeons. The momentous occurrence that intervened during those 6 months was Mr J's mother's becoming seriously ill with a progressive degenerative disease. Her illness, which led to her being in and out of hospitals for the next 20 years, was devastating for the family, but although its impact was vividly palpable, Mr J's parents decided it would be best not to tell him about it. When she was home and bedridden, and very obviously severely weakened, they would say things such as that she had a very bad cold or a flu. When she was hospitalized, they would give some minimizing explanation, and convey that she would be home in just a few days, which rarely came to pass.
The therapist's understanding of Mr J's phobia, which was communicated to Mr J, was that in large measure it was a way, in the course of his growing up, of his being able to convey to his parents how frightened he was. The atmosphere in the home was such that there was no space for him to convey what he was anxious about (that was a taboo topic) but via the phobia he could at least convey that he was anxious. The nip by the parakeet thus provided a language for his fear; as the memory of it resonated, it became the foundation for a psychological structure that served to provide some way of addressing his terror in the face of the family prohibition on discussing the mother's illness.
In approaching Mr J's phobia, the therapist assumed that helping to understand its meaning would be useful to him. The explorations that led to the understanding were of value in a number of ways. They provided a model of open and mutual engagement with a problem that was in sharp contrast with Mr J's experience growing up; they helped him to make sense of his experience and, simply by virtue of that, to feel somewhat more in control of his life; they also provided an opening and a rationale for addressing the larger set of issues that had become entwined with Mr J's phobia. Mr J manifested a pervasively avoidant way of living that was aided and justified by the phobia. The fantasy of ‘I would if only I could’ of the phobia as the explanation for his social and occupational avoidance, was an important target for therapeutic work, which needed to be addressed first before moving on to Mr J's social and occupational anxieties.
Nonetheless, and consistent with much evidence, the best way to help him get over the phobia per se was straightforward systematic desensitization. Hierarchies were created along dimensions such as the number of pigeons Mr J encountered and how far from the pigeon or pigeons Mr J was, and a desensitization procedure based on the hierarchy was applied. Mr J made significant progress with a combination of imaginal and in vivo desensitization, but the nature of his resistance was quite interesting. For more insight-oriented therapists, the use of methods such as systematic desensitization is often seen as compromising or impeding the process of exploration. In Mr J's case, however, much of the resistance was in the opposite direction, Mr J using wanting to talk and explore as a means of avoiding the systematic desensitization. Thus, the systematic desensitization, as a path to overcoming the phobia, threatened the rest of the defensive psychological structures that had evolved around the phobia.
As the work proceeded, systematic desensitization and work on Mr J's social skills were intertwined with more insight-oriented work that examined the anxieties, inhibitions, and conflicted anger and identifications in relation to his parents.
The systematic desensitization, far from being mechanical and manualized, was often a source of new associations and directions for exploration. The psychodynamic exploration, far from being neutral or focused exclusively on the ‘inner world’ or ‘psychic reality’, was engaged throughout with the choices Mr J was making in his life and the realities he confronted as a result of still earlier choices and their consequences. The cyclical psychodynamic vantage point aimed to free Mr J from the specific symptoms that constituted his presenting complaint and, to the degree that he embraced such an aim, to help him expand the possibilities that life offered him by fostering the kind of insight psychodynamic working through can provide.
The third approach is the common factors approach, which aims at utilizing and combining aspects that are common to all psychotherapies. Therapeutic warmth would be one such example (described by Gabbard and Westen, 2003, as a ‘facilitative factor’). This approach is advocated by, among others, Beitman (1987, 1992), Frank and Frank (1991), Arkowitz (1992), and Garfield (1995). Colijn's (1995) culinary metaphor would imply here that meals have to be served hot.
The common factors therapy for depression developed by Arkowitz (1992) is based on the view that efficacy studies fail to show differential effectiveness of different therapies. Moreover, it is often shown that attention-placebo controls are effective in their own right. Because depression is associated with low social support, the therapeutic relationship with all its supportive elements can be very important for patients. Arkowitz's idea was to develop a systematic—as opposed to the unsystematic attention-placebo treatments—psychotherapeutic treatment based on common factors. He based this treatment on Frank's ideas about helping relationships. The most important elements for a common factor treatment are:
A warm and positive relationship.
The application of procedures believed to be effective (e.g., support, encouragement, acceptance, opportunity for emotional expression).
A plausible explanation of symptoms, and a treatment rationale connecting the therapeutic procedures alleviating these symptoms.
Inducing positive expectations of the treatment.
Arkowitz articulated guidelines based on existing treatment manuals, and on Rogers’ work (the necessary and sufficient conditions of change, i.e., empathy, genuineness, and unconditional positive regard, cf. ‘Empathy, positive regard, and congruence’ section). Other therapist behaviors include encouraging affective expression, providing empathic reflections of thoughts and feelings, and providing realistic support and encouragement.
Arkowitz' guidelines can be viewed as a common factors treatment because the therapist is explicitly advised not to engage in specific interventions derived from specific theories, e.g., interpretations, active attempts to correct negative and distorted thinking, a persistent focus on interpersonal conflict, or specific behavioral instructions or assignments.
The common factors approach delineated by Arkowitz is reminiscent of the general model of supportive therapy (cf. ‘Common factors in practice: supportive psychotherapy’ section, see below) but differs in that it is specifically designed for milder depression and explicitly eschews designating itself as a modality—even as a ‘nonmodal modality’!
Supportive psychotherapy (ST) is nevertheless perhaps best seen as the day-to-day clinical manifestation of the common factors approach described above. ST is paradoxical in that it is widely practiced by mental health professionals, and yet is the least theorized, recognized, regulated, or researched. It is provided to clients by psychiatric nurses, psychiatrists, counselors, social workers, general practitioners (family physicians), and clinical psychologists, often in combination with pharmacotherapy and social interventions.
Rockland (1989) and Van Marle and Holmes (2002) provide accounts of the theoretical, research, and clinical aspects of ST—minimal though they are compared with other modalities. The aims of ST are to enhance coping; to maximize strengths; and to maintain the positive aspects of the status quo, including preventing deterioration, especially in the case of clients with major mental illnesses. Regression in the service of personality restructuring is discouraged. Dependency on the therapist is assumed, but kept within manageable bounds by titrating a ‘minimal necessary intervention’ (i.e., contact frequency) against clinical need.
Therapists accept that they may need to act as an ‘auxiliary ego’ for the patient, and to facilitate major life decisions in the areas of housing, employment, marriage, and the use of medication. There is always an attempt to bolster and buttress the patient's ego strengths, and to counteract tendencies to self-destructiveness.
The development of transference, especially negative and regressive transference, is discouraged by the relative nonopacity of therapists who, within limits, will allow themselves to be more ‘real’ than in traditional psychoanalytic approaches. This might entail making ‘joining’ remarks, offering limited self-revelation, and occupying a more definite professional role as a doctor or psychologist, rather than cultivating psychoanalytic neutrality. Equally, a CBT therapist working in ST would put much less pressure on the client to complete homework tasks, or carry out challenging psychological ‘experiments’ to test their assumptions as compared with their formal CBT practice.
The indications for ST include any psychiatric illness where the ego is felt to be too fragile for exploratory or regressive therapy. Thus patients with psychotic illnesses, severe personality disorders or somatization disorders may all be candidates for ST, often after a period of more formal therapy has been tried and failed. Equally, as the patient matures, ST can be a precursor to more intensive monotherapy.
Mrs B, a married high school teacher in her 30s, suffered from major depressive disorder and borderline personality disorder and was referred for psychoanalytic psychotherapy. She had had a very disturbed period in her 20s, spending 2 years in an inpatient psychiatric unit. Her arms were a mass of self-inflicted scars. Her capacity to cope with her daily life of work and looking after her small son were severely compromised and she spent most of her weekends in bed, recovering from the week and being waited on hand and foot by her dutiful and desperate husband.
Initially she embarked willingly on therapy but soon became increasingly suspicious and paranoid in the traditional psychoanalytic context. She did not like lying down on the couch, and felt that her therapist was laughing at her. She wondered if the smoke alarms were in fact secret microphones spying on her. She found the therapist's silence at the start of sessions unbearable, and his attempts to link current difficulties with her bleak and highly ‘unsupportive’ childhood (her mother ill with depression and her father sexually abusive of her) far-fetched and absurd.
Therapy increasingly approached an ‘impasse’ and things came to a head when Mrs B had to be readmitted to hospital as her depressive features worsened and she became suicidal.
At this point the therapist decided to switch to ST. Mrs B's sessions were reduced from thrice to once weekly, she sat up face-to-face, he initiated the sessions by asking her each time ‘how are things going’, and was generally smiley and supportive, using warmth and humor as much as was possible. He helped her identify her strengths and construed as ‘heroic’ (without irony) her capacity to negotiate her job, motherhood, and a marriage given her major mental illness. The first few minutes of the session were often spent discussing neutral topics such as the book she happened to be reading, holiday plans, or films she had seen. The therapist made practical suggestions when she brought problems concerning the upbringing of her son.
Therapy continued for the next 10 years during which time she left her unsatisfactory marriage, made a much better match, looked after her son effectively, found a less demanding part-time job, and had no further hospital admissions. The frequency of sessions gradually reduced from weekly, to fortnightly to monthly to bi-monthly.
Several conceptualizations of common factors are in existence (e.g., Karasu, 1986; Grencavage and Norcross, 1990; Lambert and Bergin, 1994; Lambert and Ogles, 2004; Trijsburg et al., in press). These are based on theoretical considerations (Karasu, 1986), study of the literature (Grencavage and Norcross, 1990), empirical findings (Lambert and Bergin, 1994; Lambert and Barley, 2002; Lambert and Ogles, 2004), and on surveys (Trijsburg et al., in press).
Karasu's (1986) system is based on three concepts: affect induction, cognitive control, and behavioral regulation.
This is viewed by Karasu as the primary instrument of primitive healing procedures. To this end, séances are held, often in groups led by healers, and with the aid of rhythmic music, chanting, dance, the use of intoxicating or hallucinatory drugs and exhaustion (e.g., lack of sleep). This results in trancelike states, accompanied by diminished resistance and heightened sensitivity to suggestions. By using suggestion, evil forces, demons, and spirit possession, held to lie at the root of the individual's sufferings, will be mastered or exorcized. The sufferer will be reconciled with life and his or her own situation.
Affect induction, Karasu claims, has found its way into official psychotherapy, e.g., in flooding and implosion (behavioral techniques) or as a catharsis (in the early days of psychoanalysis) and in so-called ‘chair-work’ (Gestalt, experiential therapy). However, most applications of affect induction can be found in the periphery of official psychotherapy, e.g., in bioenergetics, primal scream, and Morita therapy. Karasu argues that without working through, affect induction in itself does not lead to permanent psychological change. Nevertheless many treatment modalities use more subtle forms of affect induction, based on the assumption that affective experiences during treatment are superior in their effects than purely intellectual or cognitive experiences (Elliott et al., 2004).
This is used by more sophisticated therapies to render more permanent the transient changes conjured up by affect induction in primitive healing. Cognitive explanations and beliefs in primitive healing are based on irrational convictions. Moreover, the context is one of a highly charged and unexamined dependent relationship (Ehrenwald, 1966). According to Karasu, cognitive control is integral to any psychotherapeutic modality, implying the acquisition of new perceptions and patterns of thinking, leading to growing self-consciousness and understanding.
This is self-evidently the trademark of behavior therapy. But learning to act differently is also implicit in nonbehavioral treatment modalities, e.g., psychoanalysis and client-centered psychotherapy. ‘Insight’ without behavioral change is considered by psychoanalysts to be a sign of intellectual rather than emotional understanding. Behavior therapists induce behavioral change by direction, suggestion, and advice. In contrast, psychoanalysts and client-centered therapists refrain from engaging in such direct methods, but would challenge patients where there appear to be difficulty in generalizing from insights gained in therapy into everyday life.
Grencavage and Norcross (1990) collected publications concerned with common factors and counted the number of times each factor was named. Through this procedure they delineated five categories of common factors: patient characteristics, therapist characteristics, change processes, structure of the treatment, and the therapeutic relationship (see Table 10.1).
There is general agreement in the literature about the relevance of these five overarching topics, although most schools, competing in the psychotherapeutic market-place, stress their supposedly unique techniques for achieving change. According to Grencavage and Norcross, the relationship forms the bedrock of therapeutic change. They subdivide the elements contributing to the relationship into several components: client characteristics (e.g., positive expectation and hope or faith), therapist qualities (e.g., warmth, empathic understanding, and acceptance), treatment structure (e.g., a healing setting and communication), and relationship elements (e.g., development of working alliance and engagement). The research literature (q.v. Chapter 38 Psychotherapy Research, this volume) consistently shows that the therapeutic relationship is a crucial determinant of good outcomes in therapy. Apart from this, most authors agree on the importance of a degree of abreaction, the acquisition and practicing of new behaviors, and the offering of a treatment rationale.
Lambert and Bergin divide common factors into support, learning, and action factors. Theirs is a phasic model, in which support precedes changes in belief system and attitudes, which in their turn lead on to behavioral changes. Table 10.2 summarizes what they see as the relevant components of effective psychotherapy.
Lambert and Barley (2002) summarized the findings, based on more than 100 studies, underpinning the explanatory model of improvement in psychotherapy as a function of therapeutic factors (Lambert and Bergin, 1994). Extratherapeutic factors (e.g., diagnostic variables and the availability of social support) explain 40% of improvement, specific therapeutic techniques 15%, expectancy (placebo) 15%, and common factors, 30%. The latter group (also called ‘relationship factors’), consists of therapist variables (e.g., interpersonal style, personal attributes), facilitating conditions (e.g., empathy, warmth, and positive regard), and the therapeutic relationship (e.g., working alliance). These relationship (or common) factors largely resemble the support factors summarized in Table 10.2, and appear to predict a larger proportion of outcome variance than specific factors (summarized in Table 10.2 as learning and action factors).
Another approach to common factor research derives from a field survey of Dutch psychotherapists (Trijsburg et al., in press). In this study, 1142 psychotherapists of different psychotherapy orientations rated 72 interventions from the Comprehensive Psychotherapeutic Interventions Rating Scale. Factor analysis revealed specific and common factors. The specific factors were: behavioral, cognitive, experiential, psychoanalytic, psychodynamic, strategic interventions, and ‘chair work’ (i.e., ‘gestalt-humanistic’). The common factors were: facilitating, authoritative support, coaching, directive process, and structuring interventions (see Table 10.3).
|
Table 10.1 Common factors, mentioned in 50 publications (1936–89)
|
||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||||||||||||||
|
Table 10.2 Sequential listing of factors common across therapies that are associated with positive outcomes
|
||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||||||||||
Besides the facilitating factor, already established in the literature, authoritative support, coaching, directive process, and structuring interventions were more unexpected findings of this study. They are transmodal and in part confirm the lists produced by Karasu, Grencavage and Norcross, and Lambert and Bergin. This study shows that specific interventions themselves, traditionally associated with specific therapeutic approaches, are in fact common to several schools, thereby underlining the view that the combination between specific and common factors are both essential for therapeutic change.
Empathy, positive regard, and congruence were formulated by Rogers (1951) as the necessary and sufficient conditions of therapeutic change. Although referring to a basic attitude toward patients, these three conditions can be translated into concrete therapist behaviors, which then can be measured and correlated with outcome.
|
Table 10.3
Common factors according to the Confirmatory Factor Analysis of items
of the Comprehensive Psychotherapeutic Interventions Rating Scale
|
||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||||||||
Empathy may be defined as ‘understanding the client's frame of reference and way of experiencing the world’ (Bohart et al., 2002, p. 89). The construct is multifaceted and complex. It comprises attitudinal and behavioral, as well as cognitive and affective elements. Empathy operates in the dialogue between the therapist and the patient, and influences both of them. Empathy can be expressed in many ways, e.g., restating what the patient has said in different words, thus adding meaning or depth, or asking questions. The nonverbal aspects of communicating empathy, it's timing and wording, are highly important. In order to be effective, empathic understanding needs to be accurate and sensitive in confirming the experiences and feelings of the patient. Perhaps due to the multifaceted character of the construct, many different measures of empathy have been developed, e.g., observer-, client- and therapist-rated instruments, global measures as well measures that tap empathy on a moment-to-moment basis.
A meta-analysis of the effects of empathy on the outcome of treatment (Bohart et al., 2002) based on 47 studies and 190 separate tests of the empathy-outcome association in 3026 clients, yielded a weighted effect size of r = 0.32. This is a medium effect but which surpasses the effect sizes from studies of working alliance. Interestingly, empathy was at least as, and maybe somewhat more, effective in cognitive-behavioral therapies than in experiential, psychodynamic and other therapies. The authors suggest, somewhat paradoxically, that empathy may be more important in directive treatments, thus providing ‘an effective ground for intervention’ (p. 96).
Rogers's concept of positive regard is also complex and multifaceted. Its meaning is conveyed through many similar terms, e.g., affirmation, respect, acceptance (nonpossessive) warmth, support, caring, and prizing (Farber and Lane, 2002). In their 2004 research summary, Orlinsky et al. (2004) grouped positive regard under the heading of ‘therapist affirmation versus negation’, defined as ‘personal rapport in a relationship… manifested in the feelings that persons have towards one another (e.g., liking, warmth, trust vs. wariness, aloofness, resentment)’ (p. 353). In their 1994 review Orlinsky et al. concluded that therapist affirmation is positively correlated with outcome in 56% of process-outcome correlations (41% not significant, 3% negative). In the 2004 review Orlinsky et al. (2004) concluded that therapist affirmation is positively correlated with outcome in 56% of process-outcome correlations (41% nonsignificant, 3% negative). In the 2004 review they reported on 12 addition al studies and concluded that ‘a clear majority of findings showed affirmative therapist behaviour related to positive outcome’.
Congruence involves ‘both a self-awareness on the part of the therapist, and a willingness to share this awareness’ (Klein et al., 2002). Related concepts are openness, self-congruence, genuineness, and transparency. Again, this is a complex concept, involving, maybe more so than with empathy and positive regard, the quality of the relationship between therapist and patient. The empirical evidence on the association between congruence and outcome can be evaluated as mixed (Orlinsky et al., 1994, 2004; Klein et al., 2002). Klein et al. (2002) reported 34%, and Orlinsky et al. (1994) 38% positive results. As Orlinsky et al. (1994) found five studies published in the 1980s, and three in the period 1993–2001, there seems clearly to be a diminished interest in research on congruence in relation to outcome. Nevertheless, Klein et al. (2002) concluded that congruence, perhaps in interaction with empathy and positive regard, is likely to exert a positive influence on outcome.
Historically, self-disclosure has been viewed as an aspect of genuineness or transparency in client-centered therapy, defined as the functional use of personal information (Carkhuff, 1969). This definition implies that self-disclosures relate to verbal expressions and not to nonverbal behavior or personal characteristics of therapists (Hill and Knox, 2002). Clearly there is an important distinction between gratuitous personal revelations on the part of the therapist (‘I found myself getting depressed too, after my mother died last year’), and self-disclosure that aims to illustrate that the therapist has a ‘thinking mind’ and a specific point of view (‘what you said just now made me feel quite sad, and made me think how easily we tend to underestimate the impact of bereavement in our lives’).
Although self-disclosure is usually associated with client-centered therapy, current developments in psychoanalytic psychotherapy and CBT, suggest that the judicious and thoughtful use of self-disclosures may help in furthering the responsiveness of patients and in strengthening the therapeutic alliance, thereby leading to more effective treatments. For instance, some contemporary psychoanalysts acknowledge the current trend towards more therapist disclosure (Ehrenberg, 1995; Renik, 1995; Bernstein, 1999). Although Wolpe (1984) stated that therapist disclosure is not a behavior therapy technique, the possibility of a ‘dyadic effect’, meaning that therapist disclosure has the potential to encourage client disclosure, is acknowledged in behavior therapy (Pope, 1979). The dyadic effect can be explained by modeling (Bandura, 1970) and by social exchange theory. Other indications for self-disclosure in behavior therapy include applying modeling and behavioral rehearsal (Lazarus, 1985), or when the patient shows behavior toward the therapist resembling maladaptive behaviors toward other people (O'Leary and Wilson, 1975).
Hill and Knox (2002) offer several practice guidelines, related to intrapersonal self-disclosures, summarized below:
therapists should generally disclose infrequently;
the most appropriate topic involves professional background, and the least appropriate include sexual practices and beliefs;
disclosures should be used to validate reality, normalize, model, strengthen the alliance, or offer alternative ways to think and act;
therapists should avoid using disclosures that are for their own needs, remove the focus from the patient, or otherwise interfere with the therapeutic process or the therapeutic relationship.
Resistance, originally a psychoanalytic concept is defined in at least three ways in the literature: as a patient characteristic, as a response to accurate but unpalatable interventions applied by the therapist, or as a characteristic of the therapeutic relationship.
Resistance is a core element in psychoanalytic theory, and is inherent to the ‘basic rule’ of free association, which is designed to overcome it. Traditionally, the psychoanalytic model views resistance as being located at the level of the patient. However, newer models hold that resistance may be viewed as relationally determined (Trijsburg, 2003).
Treatment modalities that view resistance as being avoidable, rather than intrinsic to the therapeutic process, tend to apply specific strategies to improve compliance. Examples include structuring the treatment, stressing the gradualness of change (including setbacks), and structuring homework (Goldfried, 1982). However, noncompliance may also be thought as manifesting the problem behavior that brought the patient to therapy in the first place. Behavior therapy and CBT have developed specific techniques for conceptualizing and overcoming resistance. The following aspects of resistance can be distinguished (Goldfried, 1982): (1) resistance as a manifestation of patient's problems; (2) resistance resulting from other problems than the one treated; (3) resistance due to pessimism in the patient; (4) resistance arising from fear of changing; (5) resistance due to overburdening the patient; (6) resistance resulting from the patient not being motivated to change (defined by Jacobson and Margolin, 1979, in terms of costs–benefits: as long as benefits lag behind costs in terms of work to be done, there will be obstacles in the way of change, i.e., resistance); (7) reactance, i.e., an emotional response to demands.
The concept of (interpersonal) reactance, colloquially ‘contrariness’, deserves special mention. This concept derives from empirical research on persuasion theory and models of interpersonal influence (Brehm and Brehm, 1981) and refers to the tendency to respond in an oppositional manner if someone feels thwarted in his or her autonomy. Directive interventions in reactant patients increases the risk of treatment failure. When confronted by such situations, interventions low in directiveness and paradoxical interventions may result in better effects.
Treatment techniques developed for the situations described above are switching the focus of treatment from the therapeutic work outside of therapy to therapy itself; changing the treatment goals; reformulation of the problem, often in more positive terms, enabling the patient to get a different view of the problem (e.g., when resistance results from anticipatory anxiety, the therapist may normalize anxiety, may stress the importance of anxiety as a signal of change, or as a challenge to experiment with the feeling), ambiguous assignment; and paradoxical interventions.
Ambiguous assignments are those that are given ultratentatively, suggesting that the assignment may or may not prove to be effective, relevant, or sensible, or may be too difficult for the patient (e.g., formulated as a rhetorical question ‘I'm thinking of this assignment, which may be quite helpful to address this problem. However, I'm wondering if this assignment is not too difficult for you? If you're interested, I can tell you how it goes. You want to hear about it?’). Also, the therapist confesses that the assignment may well be ill timed, the patient may not have enough time to follow the assignment up, etc. In this way, the patient has a chance to escape, without having failed the assignment. The hope is that he may become interested and still perform the task, thereby gaining positive feedback from accomplishment.
Paradoxical interventions often take the form of apparently unfitting interventions related to symptomatic behavior (e.g., ‘prescribing the symptom’, e.g., to an agoraphobic ‘I think it is important that you go continue not to venture outside, not even for a second’), cognitions (e.g., the instruction make an anticipated catastrophe worse by exaggerating it in one's mind), or to relational behaviors (e.g., the task of having an argument with one's spouse at a predetermined point in time). In the Trijsburg et al. (in press) study, paradoxical interventions and the ambiguous task assignment clustered in the ‘strategic interventions’ factor.
Other interventions, found in the Trijsburg et al. (in press) study to belong to a factor of ‘authoritative support’, may also be useful when therapy reaches an ‘impasse’ (a psychoanalytic concept, q.v.), e.g., direct reassurance, placing the responsibility for a problem outside the patient, and collaboration.
Two currently important models of the working alliance concept, i.e., Luborsky's two-factor model (Luborsky, 1976) and Bordin's pantheoretical model (Bordin, 1976). Luborsky distinguishes ‘Type I’ and ‘Type II’ working alliance. Type I working alliance defines the therapist as warm, helping, and supporting. Type II relates to the cooperation between therapist and patient. Research suggests that Type I working alliance is more important in the opening phase of therapy, whereas the Type II will be dominant in the later phases of treatment (Horvath et al., 1993).
In Bordin's (1976) view the central part of the working alliance is the active collaboration between patient and therapist. The working alliance involves three aspects, i.e., agreement on the therapeutic goals, agreement on the tasks to be done as the therapeutic work, and an emotional bond between the patient and the therapist.
Earlier studies showed the working alliance to be an important predictor of outcome, which is similar across various treatment modalities (Horvath and Symonds, 1991; Horvath and Greenberg, 1994; Martin et al., 2000). Estimations of the effect size (ES), based on correlational analyses, vary between ES = 0.22 (Martin et al., 2000), and ES = 0.26 (Horvath and Symonds, 1991). The study reported in Norcross (2002b), using partly overlapping data with earlier studies, resulted in an effect size of ES = 0.21 (weighted by sample size; Horvath and Bedi, 2002).
Horvath and Bedi (2002) suggest that the therapist's ability to maintain open and clear communication is related to the quality of the alliance. On the negative side, poor or deteriorating alliances are reported in therapists that take charge in the early phase of therapy, who are perceived by their clients as ‘cold’, or who offered insight or interpretation prematurely.
In all psychotherapeutic modalities, the working alliance is important, not as a goal in itself, but a means to an end, e.g., working through the transference neurosis, bringing about self-exploration, behavior change, or changes in a system. Where this goes wrong, therapy is in jeopardy. Alliance rupture and repair are therefore crucial to successful therapeutic work.
From a psychodynamic perspective, failure to repair minute-to-minute, or gross alliance ruptures, characterizes the unattuned care-giving characteristic of pre-borderline states. Via projective identification (q.v.) the therapist will characteristically be induced into such mis-attunements. Working with alliance ruptures in therapy help the patient to trust himself and his relationships with others, possibly for the first time in his or her life.
Over the past 10 years, Safran and Muran developed several techniques that may be helpful in overcoming ruptures in the therapeutic alliance. Their views were summarized in a ‘relational treatment guide’ (Safran and Muran, 2000). The authors distinguish between ruptures in the therapeutic process at the level of tasks and goals, and at the level of the therapeutic bond. They describe interventions that may help repairing these ruptures. The interventions are described in Table 10.4, and will be discussed in the following paragraphs.
Disagreements on tasks and goals can be approached in direct and in indirect ways.
Direct approaches are: (1) explaining the therapeutic rationale; (2) microprocessing; and (3) exploring core relational themes. Indirect approaches to disagreements on tasks and goals are (4) reframing the meaning of tasks and goals, and (5) changing tasks and goals.
Explaining the therapeutic rationale. Disagreement on tasks and goals may result from (simple) misunderstandings or a lack of understanding in the patient. In case of a misunderstanding, the therapist may (once again) explain procedures or tasks, or clarify the reasons why a particular procedure is applied. One example would be to discuss the importance of monitoring behavior between sessions, or why particular exercises may be helpful to the patient. In psychodynamic treatments the therapist may explain the nature of free association, or the reasons why the therapist refrains from giving advice. Explanations are focused on the content and procedural aspects of treatments.
Table 10.4 Therapeutic alliance rupture intervention strategiesDirect Indirect Disagreements on tasks and goals Therapeutic rationale and microprocessing tasks Reframing the meaning of tasks and goals Exploring core relational themes Changing tasks and goals Problems associated with the relational bond Clarifying misunderstandings Allying with the resistance Exploring core relational themes New relational experience From Safran and Muran (2000, p. 17). Microprocessing. Some patients may not have understood a question or explanation. This could be a simple misunderstanding, or due to unconscious resistance. At first, many patients react to the question ‘could you tell me what's on your mind?’ with something like, ‘Nothing. What do you expect me to say?’ Microprocessing techniques that may be helpful here could be exercises that may help patients understand the type of inner experiences that are important in therapeutic change (e.g., focusing, Gendlin, 1996, or the reconstruction of automatic thoughts). For example, when a patient was challenged about her apparent reluctance to talk about painful experiences as a child, she explained that she felt that she did not want to ‘keep whining about things in the past’, and was afraid her therapist would dislike her for this. She admitted that she always feared people thinking about her as being a whining and sulking person.
Exploring core relational themes. The tone of voice, nonverbal behavior, and the attitude of a patient may point to aversion, distrust, or skepticism and the collaboration in early phases of the treatment.
Reframing (an indirect approach to disagreements on tasks and goals) derives from the strategic (systemic) approach, and was described above as ‘reformulation, often in more positive terms’ (cf. ‘Working with resistance’ section). An example of this would be exposure to social situations in a social phobic patient. As exposure may induce feelings of anxiety and shame, the patient may react to an assignment of this kind with fear or aversion. Reformulation in terms of finding an opportunity to observe one's reactions (self-monitoring) in the situation, instead of just running the risk of being humiliated, may help the patient to accept the assignment.
Changing tasks and goals, another indirect approach, implies the empathic consideration of the therapist with respect to the problems patients may have with seemingly unfitting or too difficult tasks or goals (cf. ‘Working with resistance’ section). This could lead the patient to formulate more relevant goals and tasks. Also, the patient will then have the experience of being in charge, which in turn may also lead to increasing motivation to take on more difficult assignments later in the treatment.
Problems associated with the relational bond can be approached in direct and in indirect ways. Direct approaches are (1) clarifying misunderstandings, and (2) exploring core relationship themes. Indirect approaches are (3) going along with the resistance, and (4) new relationship experience.
Misunderstandings can be clarified in a direct way, if the therapist is able to be open about what may have caused the misunderstanding. Acknowledgement of one's own role in causing the misunderstanding and explaining this to the patient are necessary for this clarification to be effective. Clarifications need to be given in the here-and-now, and need not lead to disclosure about personal problems in the therapist, nor need they have to lead to interpretations of possible inner conflicts of the patient. One example would be the patient that falls silent during a session, seems no longer interested or absent. The therapist may ask what happened, and this could lead the patient to hint at being hurt by something the therapist has said. Repairing the rupture would imply that the therapist recognizes what s/he could have contributed to the patient's feelings (e.g., ‘I'm sorry if I said something that distressed you. What went through your mind when I said that?’, or ‘You know, I think I said that wrong. What I should have said is: ‘I'm worried that the vacation might not turn out well for you’).
Every rupture in the relational bond may eventually lead to the exploration of core relational themes. For instance, a therapist treating a stubborn, reticent, and sometimes unpleasant patient, sooner or later may feel tempted to ‘forget’ an appointment, or to say something out of place, which then of course will have rejecting implications (Horvath and Bedi, 2002). Focusing on these ruptures in the relational bond enables the therapist and patient to discuss the relational theme in terms of earlier experiences, to gain insight in these experiences, and to achieve therapeutic changes.
Allying with the resistance, an indirect approach, conceives of the negative attitude in the patient as his or her best answer in the situation. For example, the patient might say: ‘I don't like talking about this. You always bring this up, and every time I know you are going to do this, and I don't want it. I want to stop this. I'm leaving’. Saying ‘I think you find it difficult to talk about this’ might merely exacerbate the rupture. Instead, the therapist could say something like ‘You have made your point. It is obvious that you don't want to discuss this, and you have a perfect right to talk or not talk about whatever you like in your session’.
A second indirect approach is to attempt to create a new relational experience by the therapist's nonintrusive presence in the therapy, especially when things are very difficult. Here the nonintrusive presence of the therapist may be essential to prevent the working alliance from breaking down. Examples might be affect-storms, panic attacks, acute depersonalization, states of narcissistic injury, or persistent silence. In this type of situation, the therapist may stay in the background, acting as a ‘holding environment’ (Winnicott, 1976).
Safran and Muran's (2000) view of rupture–repair clearly goes beyond ‘schoolism’. Theirs is a truly integrative approach, in that they show that different theoretical views may each contribute in important ways to the maintenance of a good working alliance. For instance, self-disclosure and focusing derive from the client-centered approach, reframing from a strategic and systemic viewpoint, and exploring core relationship themes from the psychodynamic approach.
The number of studies of the effectiveness of repairing alliance ruptures is still limited. In their review, Safran et al. (2002), p. 251) concluded that there is preliminary evidence available that: (1) indicates that ruptures occur fairly frequently in psychotherapy; (2) supports the importance of specific procedures (e.g., nondefensive behavior of the therapist) in resolving ruptures; (3) indicates that for some patients, the development of an alliance characterized by rupture–repair cycles over the course of treatment, is associated with positive outcome; and (4) indicates that poor outcome is associated with disruptive patterns (therapists responding in a hostile way to hostile patients).
If integrative therapy (IT) is seen by its advocates as combining the best from all the traditional monotherapies then indications would be many, contraindications few. Also, given the lack of specificity of IT and the fact that it covers a range of different approaches including supportive therapy, eclectic therapy, aspects of the work of the mature monotherapy clinician, together with explicitly ‘integrative’ therapies such as interpersonal psychotherapy (combining psychodynamic, systemic, and supportive), DBT (CBT, behavioral therapy, and Zen), and CAT (analytic, DBT, and interpersonal) defining the indications is no easy task. The practice of IT is more likely to arise from adventitious conditions such as the habits and orientation of the therapist, the psychotherapeutic culture of a particular center and its often charismatic leaders, and the demands of those responsible for funding the therapy, rather than the specific needs of the client.
Nevertheless, indications might be considered as follows:
when traditional monotherapies have failed
where the presenting problem and its developmental background are uncertain, and a number of different approaches may be needed before it is clear which direction the client needs to go
where the therapist lacks experience in monotherapies but has basic ‘common factors’ counseling skills
where the patient is too disturbed for monotherapy and is more suitable the common factors approach embodied in ST
where the client has a number of different problems which need to be tackled sequentially by the same therapist, e.g., agoraphobia (therapist uses CBT), marital difficulties (therapist performs couple therapy) and depression (therapist uses interpersonal psychotherapy) (although monotherapy enthusiasts would try to find the common theme behind all three, low self-esteem, or lack of assertiveness for instance, and address therapy to that).
In a stepped care approach it would be conceivable to start with an ‘evidence-based’ monotherapy, aimed at the central problem of the patient, and to add other therapeutic approaches only when the complexity (e.g., comorbidity, chronicity) of the patient's problems would demand such extensions. As indicated above, an integrative approach is especially suitable for more complex relationship-based treatments for character problems or personality disorders.
The main contraindication arises from the fact that IT can become a ‘defense’ on the part of both therapist and client against recognizing the need for monotherapy. Thus a patient may ‘offer’ the therapist a number of disparate difficulties—e.g., difficulty in sustaining long-term relationships, uncertainty about choice of career, and bulimic symptoms. The integrative therapist might be tempted to take each of these in turn and ‘work’ on them, with varying degrees of success, rather than seeing all three as manifestations of a developmental disorder associated with disturbed care-giving in childhood, which would respond best to monotherapy, e.g., psychoanalytic, or ‘schema-focused’ CBT.
Offering IT in this circumstance would be a pitfall. This relates to the problem of ‘model-hopping’ in IT. Monotherapies have clearly developed theories and procedures for dealing with difficulty, encapsulated in such psychoanalytic concepts as impasse and working through. If the therapist changes tack every time the therapy meets resistance then conflicts will be skirted around and core problems left untouched.
A related problem concerns the ethical dimension of therapy. IT is perhaps inherently less clearly defined in its procedures and processes than monotherapies. Therapy that encourages warmth and empathy, and does not necessarily conceptualize countertransference or enactment, may lend itself to therapeutic abuse more easily than monotherapies (although we know of no specific empirical evidence to support this suggestion). The therapist who offers his female client a ‘supportive’ hug at the end of a session, or tells her how attractive she is in order to counteract her feelings of low self-esteem, or offers her sex therapy to help with her anorgasmia, in addition to psychoanalytic therapy and ‘chair work’, may have placed more than one foot on the ‘slippery slope’ that leads ultimately to the abuse of clients by therapists. Good supervision and reflective practice are an essential part of IT, as they are of all psychotherapeutic work.
Psychotherapy integration is a tendency present both within the traditional psychotherapy schools, which incorporate therapeutic ideas and methods from other orientations, and in the dialogue between therapy schools, which ultimately will lead to new forms of therapy. This tendency is likely to continue to grow, as the focus on evidence-based treatments gradually shift from empirically supported diagnosis–treatment combinations, to evidence-based relationship and contextual factors. Also, the growing number of studies into the dose–effect relationship in psychotherapy, closely related to managed care policy making (Lambert and Ogles, 2004) are likely to stimulate psychotherapy integration, as cognitive therapies discover the need for more extended treatments, and psychoanalytic therapies the need for greater brevity. More and more, the ‘pure-form’ psychotherapy modalities will be stimulated to integrate relevant therapeutic practices from other schools as well as common factors. Whether this will lead to one common general theory of psychotherapy is a question for future theoreticians and researchers to determine, some of whom we hope may be readers of this volume.