The terms psychoanalytic and psychodynamic have increasingly been used synonymously in discussions of psychotherapy. Both psychotherapeutic approaches derive from a set of core principles derived from psychoanalysis. Among these principles are transference, countertransference, resistance, the dynamic unconscious, a developmental lens to view adult experience, and psychic determinism. The historical origins of this approach date back to the development of psychoanalysis by Sigmund Freud in the late 1890s and the early 1900s.
Although Freud originally was trained as a neurologist, under the influence of the French neurologist Jean-Martin Charcot, he became intrigued with the mysteries of hysteria. He later collaborated with Josef Breuer on the use of hypnotic suggestion in the treatment of patients suffering from hysteria. In their classical contributions to the subject, Breuer and Freud argued that hysterical patients suffer from ‘reminiscences,’ suggesting that an unacceptable and repressed idea was responsible for the symptoms of the illness. This understanding led to a therapeutic approach that came to be known as abreaction. Freud was initially convinced that bringing a repressed memory of a traumatic event back into the patient's conscious awareness through hypnotic suggestion would produce a catharsis that would result in removal of the patient's symptoms. In other words, the patient would be able to recover and verbalize the feelings that were associated with the original trauma.
Freud soon became frustrated with the use of hypnosis and cathartic abreaction because he learned that this therapeutic approach was often not acceptable and reflected the patient's wish to please the doctor. He also observed that some patients manifested resistance to this therapeutic approach. Either they were unable to be hypnotized or incapable of recovering memories that had etiological significance.
In addition, Freud began to recognize that a powerful relationship developed between patient and doctor that had a significant erotic component. One of his patients awoke from a hypnotic trance and threw her arms around Freud's neck. This experience and others led him to develop the concept of transference, which referred to the fact that patients displace on to the analyst the feelings, thoughts, and attitudes that were originally linked to parents or other significant figures from the past.
He then modified his technique in such a way that hypnosis was discarded and replaced with the method of free association. This technique, involving asking the patient to say whatever comes to mind, is still a cornerstone of technique used by psychoanalysts throughout the world.
Freud went on to immerse himself in the study of dreams, which he viewed as the ‘royal road’ to the understanding of the unconscious. He recognized that sexualized aspects of childhood life persist into the present and influence adult behavior.
The psychoanalytic approach to psychotherapy has undergone profound transformation since the era of Freud. Each of the core principles retain the remnants of Freudian thinking, however, and much of Freud's edifice remains relevant to our current understanding of patients and the therapeutic strategies used to share that understanding with the patient. While Freud viewed transference and resistance as the essential features of any psychoanalytic approach, today we would expand the fundamental set of concepts to include countertransference, the unconscious, psychic determinism, and a developmental perspective. These basic tenets will be introduced here and elaborated later in the chapter.
Patients unconsciously relate to the psychotherapist as though the therapist is someone from their past. Although Freud regarded transference as a simple displacement of a past relationship into the present, we now recognize that the therapist's actual characteristics and behavior continuously contribute to the nature of transference (Renik, 1993; Hoffman, 1998). The physical characteristics, way of relating to the patient, gender, and age of the therapist all influence the patient's perception of the therapist. These features trigger neural networks within the patient that contain representations of past figures and revise these ‘ghosts’ from the past in the present (Westen and Gabbard, 2002a). In addition to the repetitive dimension of transference, the patient also may harbor a longing for a healing or corrective experience to compensate for the problems that occurred in childhood relationships. Hence a longing for a different kind of relationship may be inherent in transference.
Patients still resist psychotherapy as they did in Freud's day. One of the great discoveries of Freud was that patients may be ambivalent about getting better and unconsciously (or consciously) oppose attempts to help them. Resistance may manifest itself as silence in therapy sessions, as avoidance of difficult topics, or as the forgetting of sessions. In essence, resistance can be viewed as any way that patients defend themselves against changing in the service of preserving their illness as it is. Resistance is no longer viewed as an obstacle to be removed by the therapist. Rather, it is viewed as a revelation about how the patient's past influences current behavior in the relationship with the therapist (Friedman, 1991). If, for example, a male patient experiences his male therapist as critical, he may be reluctant to say much. This reticence may reveal a great deal about his relationship with his father and with other male authority figures. Helping the patient to understand resistance is a central feature of psychodynamic therapy.
Freud wrote very little about countertransference. He originally defined it as the analyst's transference to the patient. He generally regarded it as an interference in the analyst that paralleled transference in the patient. In other words, the analyst would unconsciously view the patient as someone from the past and therefore have difficulty treating the patient. Countertransference is now regarded as an enormously valuable therapeutic tool in psychoanalytic therapy. It is a joint creation that stems in part from the therapist's past but also in part from the patient's internal world. In other words, patients induce certain feelings in the therapist that provide the therapist with a glimpse of the patient's internal world and what sort of feelings are evoked in other relationships outside of therapy (Gabbard, 1995).
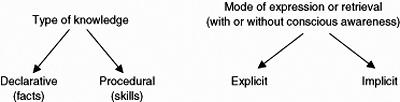
Freud's premise that much of mental life is unconscious has been extensively validated by research in the field of experimental psychology (Westen, 1999). However, psychoanalytic psychotherapists are more likely to refer to unconscious representations or unconscious mental functioning rather than the unconscious. The notion of ‘the unconscious’ as a storage place or reservoir is no longer in keeping with contemporary neuroscience research. We now recognize that memories are stored differently, depending on the type of knowledge being stored. Declarative memory involves facts and episodes of one's life, while procedural memory involves skills or procedures. Defense mechanisms, for example, are automatic unconscious procedures that regulate affect states. Memories of difficult times in one's life are aspects of declarative knowledge that may be conscious and easily recalled or may be repressed and therefore unconscious. Declarative knowledge is knowledge ‘of’, whereas procedural knowledge is knowledge ‘how’ (Westen and Gabbard, 2002b).
In current thinking that integrates psychodynamic and neuroscience data, both procedural and declarative memories can be viewed as either conscious or unconscious (see Figure 1.1). A distinction between explicit and implicit memory relates to whether knowledge is expressed and/or retrieved with or without conscious awareness. Hence the explicit versus implicit distinction can be understood as equivalent to conscious versus unconscious (Westen and Gabbard, 2000a, b).
Within this model defense mechanisms are primarily in the domain of implicit procedural memory. Suppression, though, one of the few conscious defense mechanisms, lies in the realm of explicit procedural memory because it involves the conscious banishment of certain thoughts and/or feelings from one's mind. Implicit declarative knowledge involves repressed ideas and repressed memories of events in one's life and knowledge that involves various kinds of expectations about how others will react in response to what one does. This latter category may be retrievable if one shifts one's attention to it, a category Freud called preconscious. Explicit declarative knowledge consists of facts and events that are fully conscious.
Unconscious aspects of mental functioning may reveal themselves as slips of the tongue, forgetting, or substituting names or words. Nonverbal behavior is also a reflection of unconscious and internalized modes of relating to others. In other words, how the patient relates to the therapist may say a great deal about unconscious representations of self and other within the patient.
The principle of psychic determinism asserts that our internal experience, our behaviors, our choice of romantic partners, our career decisions, and even our hobbies are shaped by unconscious forces that are beyond our awareness (Gabbard, 2000a). The psychodynamic therapist approaches a patient with the understanding that any symptom or problem may serve multiple functions. A variety of conflicts from different developmental levels all may converge to form the end result of a behavior or symptom. A psychoanalytic therapist recognizes that many of the reasons for the patient's difficulties lie outside the patient's awareness, and both therapist and patient must be willing to explore a variety of converging causes.
|
|
Fig. 1.1 Type of knowledge versus mode of expression. Reprinted from Gabbard, G. O. (2000). Psychodynamic psychiatry in clinical practice, 3rd edn, p. 8. Washington, DC: American Psychiatric Press. |
All psychoanalytic thinking is based on a developmental model of behavior. A fundamental assumption is that childhood events shape the adult person. The repetitive patterns of problematic interactions with others stem from intrapsychic issues that are internalized during childhood. In contemporary thinking about the interface between genetics and environment, we know that the genetically based temperament of the child shapes much of the interaction with the parents. In other words, characteristics that are genetically determined evoke specific parental responses, which in turn shape the child's personality (Reiss et al., 1995). Psychoanalytic therapists do not blame parents for their patient's difficulties. They see the patient's difficulties as a complex interaction between the child's characteristics, the parents' characteristics, and the ‘fit’ between them (Gabbard, 2000a).
During the time that Freud toyed with the idea of cathartic abreaction as his preferred model of healing, he was influenced by the topographic model of psychoanalysis. The unconscious mind harbored repressed pathogenic memories. Through the work of psychoanalysis, these memories would become conscious. They would lose their pathogenicity after becoming available to the patient's conscious awareness. The preconscious resided between the conscious and unconscious. The memories residing in the preconscious were available by shifting one's attention and hence were not truly repressed.
As the cathartic abreaction method failed Freud, he developed the tripartite structural model involving, ego, id, and superego. The structural model lends itself to a conflict-based theory that forms the foundation for ego psychology. The id is regarded as the seat of powerful instinctual drives—specifically aggression and sexuality/libido that struggle to emerge into conscious awareness. The superego, which has both conscious and unconscious aspects, is the moral agency that results from the internalization of parents and their value systems. Cultural or social values may also be internalized as part of the superego. The ego itself is partly conscious and partly unconscious, like the superego, and is thought of as the executive organ of the psyche. Conscious aspects of the ego are involved in decision making, perception, calculation, and anticipation of consequences. Among the many unconscious aspects of the ego are most of the defense mechanisms.
Ego psychology is characterized by a view of the intrapsychic world as one in which the three agencies are in constant conflict. Conflict, in turn, produces anxiety, which then results in the activation of a defense mechanism. Symptoms are formed as a result of conflict. The result of the anxiety and defense is a compromise formation. Instinctual drives seek to surface, but the ego and/or superego marshals defensive forces to stop the unacceptable drive from surfacing. The resulting compromise formation contains both the original wish arising from the id and the defense against that wish. Hence compromise gratifies the wish in a disguised and attenuated form. Both neurotic symptoms and character traits can result from these intrapsychic clashes and can be referred to as compromise formations.
Ego psychology de-emphasizes the need to plumb the depths of the unconscious for buried memories. Instead, it focuses on the fact that within the typical defensive operations, one finds the compromises and conflicts that make up the patient's character. A systematic analysis of defenses, as they enter into the treatment in the form of resistances, is a cornerstone of ego-psychological technique. Some common defenses are listed in Table 1.1 and are organized hierarchically from the most immature or pathological defenses to the most healthy or mature.
The developmental model associated with ego psychology involves the epigenetic developmental scheme linked to oral, anal, and phallic libidinal zones. Erik Erikson (1959) described the child's psychosocial crisis that occurred at each developmental phase. In the first month of existence, the infant struggles with basic trust versus basic mistrust while negotiating the oral phase of development. Autonomy versus shame and doubt is typical of the anal phase. Initiative versus guilt characters the phallic-oedipal phase. At about age 3 years and ending somewhere between 6 and 7 is the oedipal phase of developmental where the genitals are the primary source of pleasure. The child wishes to be the exclusive love object of the opposite-sex parent. During this phase the child becomes acutely aware of the triangle of mother, father, and child, having transcended the dyadic mother-child frame of reference in earlier developmental phases. The negative Oedipus complex is often used to describe the child's longing for the same-sex parent, wherein the opposite-sex parent is seen as a rival.
|
Table 1.1 A hierarchy of defense mechanisms
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the positive Oedipus complex, the child wishes to possess the opposite-sex parent exclusively and may harbor murderous wishes toward the same-sex parent. The superego is seen to result from a reluctant resignation that it is better to identify with the same-sex parent rather than risk that parent's retaliation in response to incestuous wishes. The male child may fear that father will retaliate in the form of castration, creating castration anxiety. The boy then identifies with the aggressor (father) by deciding to search for a woman like his own mother because he cannot compete with his father.
Freud used the model of male development to understand female psychology. He imagined that a little girl felt like a boy until she discovered the existence of the penis. She then felt inferior and suffered from ‘penis envy.’ Lack of empirical support for this model of development has led to major rethinking of female developmental experience (Benjamin, 1990; Chodorow, 1996). Current thinking about the construction of gender focuses on the influence of culture, identifications with parents, and internal object relations rather than rigid assumptions about anatomical differences (see Chapter 34, Gender issues in psychotherapy).
Object relations theory has become perhaps the predominant theoretical model in contemporary psychoanalytic therapy. The origins of the theory can be linked to the work of Melanie Klein in London in the 1930s and 1940s. Based on her psychoanalytic treatment of children, she developed a theory that emphasized unconscious intrapsychic fantasy and pre-oedipal development.
Klein theorized that the infant began life with a primal anxiety about annihilation. She postulated that to deal with this terror, the ego underwent a splitting process in which the ‘badness’ or aggression associated with the death instinct was projected into the mother's breast. The child then developed paranoid anxieties about the possibility that the mother would attack the infant. This concern is the primary anxiety of the paranoid-schizoid position, an early mode of organizing experience that involves splitting and projection. The good aspects of mother are split off and kept separate from the bad or persecuting aspects so that they will not be contaminated by hate or aggression. In other words, the loving aspects of the mother and the self are kept pure from the contamination of murderous rage and hatred.
The paranoid-schizoid position was proposed as the predominant way that infants organize experiences during the first 6 months. The bad object is projected and then reintrojected throughout this period. The good object may also be projected to keep it safe from ‘badness’ within the child.
After 6 months, the child begins to integrate the ‘bad’ mother with the ‘good’ mother. The child realizes that the mother has both good and bad qualities and starts to integrate the two into a whole object representation of the mother as opposed to a part object of either ‘all bad’ or ‘all good’ qualities. This developmental phase is known as the depressive position. As part of this developmental epoch, the child has depressive anxiety related to the concern that the child will cause harm to the mother he or she loves. The child may attempt to resolve this depressive anxiety through reparation. In fact, Klein reconceptualized the Oedipus complex as involving the child's effort to address depressive anxieties and guilt through making reparation to those experienced as damaged (Segal, 1964). A child may choose to become a physician, for example, as a way of healing others to repair the damage she imagines she has done to her parents.
Another key component to Klein's theory is the role of envy as a derivative of the death instinct. Envy is a form of hatred directed to the good object rather than the bad object. The envy is partly responsible for the child's perception that he or she has caused damage to the ‘good mother’ (Klein, 1957). While jealousy involves three persons, envy occurs in a two-person context.
Developmentalists criticize Klein's thinking for attributing complicated forms of cognition and perception to infants in their first several months of life. Her thinking has also been challenged because of her emphasis on the death instinct, a theory that is not endorsed by any other psychoanalytic school of thought and by her tendency to minimize real trauma while emphasizing the child's intrapsychic fantasy life.
Wilford Bion, an analysand of Klein's, was instrumental in moving Kleinian theory away from drives and towards relationships (Bateman and Holmes, 1995). He focused on how the mother serves as a container for the infant's intense affects and ‘detoxifies’ them through her nurturing so they are taken back by the infant in a more manageable form. This interactional component is considered vital in Bion's model.
While Klein's views were closely linked to Freud's drive theory, the British independent tradition stressed that the infant's drives develop in the context of the mother–infant relationship and therefore must be viewed in that context. Fairbairn (1952) even argued that drives are primarily object seeking in nature rather than tension reducing in the sense of drive theory. A key principle is that relationships are internalized in the early years of life. The object relations building blocks of life involve a representation of self, a representation of the object, and an affect that links the two.
Splitting and projective identification are two of the defense mechanisms most associated with object relations theory (see Table 1.1). Splitting involves the tendency to divide everyone into ‘all bad’ or ‘all good’ groups. This polarization of objects involves a corresponding splitting of the self. Hence contradictory presentations of the self may alternate with one another, resulting in a confusing picture both for the patient and for those close to the patient. In a developmental sense, splitting is a defense that occurs prior to conflict. As a result, patients who rely on splitting may react with indifference or bland denial when confronted with contradictions in their behavior (Kernberg, 1975).
Projective identification works in tandem with splitting in that object or self-representations that are split off may be placed in others as a way of disavowing them. In projective identification in the psychotherapeutic context, the patient unconsciously projects the self- or object representation into the treater, who then unconsciously identifies with what has been projected. Through interpersonal pressure, the patient coerces a response in the treater that corresponds to what is projected. For example, a 26-year-old female patient with borderline personality disorder had been a victim of physical abuse at the hands of her mother. When she was with her female therapist, she accused the therapist of not listening carefully to what she said. She also accused her therapist of being insensitive toward her. She told her therapist she was convinced that the therapist did not like her and did not want to see her. This behavior in the sessions continued unabated for weeks. Finally, her accusations escalated to the point where the therapist became angry at the constant barrage of accusations, and she told the patient that she was getting fed up with the many distortions that the patient brought to the therapy. She also raised her voice at her patient and exclaimed, ‘I can't take your attitude anymore!’ Hence through the interpersonal pressure of her behavior, the patient influenced her therapist to conform to the projected bad object. The therapist, in effect, became an attenuated version of the patient's abusive mother. In the ideal therapeutic situation, the projected material is then psychologically processed and modified by the therapist so that what has been projected is transformed by the therapist before it is reintrojected by the patient. This processing generally does not occur in everyday life when patients project certain aspects of themselves into others in the course of their usual contact.
Object relations theory fits well with cognitive neuroscience, in that early self and object representations are etched in specific neural networks as a result of repeated experience with figures in the environment. A central tenet of object relations theory is that the internal representation may not be exactly the same as the external figure on whom the representation is based. Children may exaggerate tendencies in parents, for example, because of their fantasies about the parents. The earliest representations tend to be more polarized and are often referred to as part objects. From the age of 3 to about 6, the part objects and part self-representations are integrated into whole object and whole self-representations and involve both good and bad qualities. When a failure of integration occurs, adult patients may go throughout their lives splitting themselves and others and repeating past object relationships through the mechanism of projective identification.
The independent perspective also was influenced by the thinking of D. W. Winnicott. He stressed the inborn tendency to grow toward self-realization. He felt there was a true self whose growth could be either impeded or facilitated by maternal responses (Winnicott, 1965). If the mother, or other caretaking figure, cannot attune herself to the child's authentic self, the child may develop a false self designed to please or placate the mothering figure.
Self psychology developed from Heinz Kohut's study of narcissistically disturbed patients who sought analysis (Kohut, 1971, 1977, 1984). Kohut's adult patients were characterized by having a highly vulnerable self-esteem that made them feel easily slighted by friends, colleagues, and romantic partners. He did not view them as suffering from intrapsychic or neurotic conflict. Kohut suggested that these individuals lacked developmentally appropriate empathy by their mothers, creating a deficit situation. Individuals with this deficit then go through life attempting to get responses from others that make up for the missing functions within themselves. Kohut called these selfobject functions, in that others must perform functions for the patient's self rather than being allowed to behave autonomously.
The selfobject functions tend to fall into three categories, which Kohut viewed as the three kinds of selfobject transferences. The mirror transference is an attempt to capture the ‘gleam in the mother's eye’ in response to phase-appropriate displays of exhibitionism that hearken back to childhood, when the child felt that empathic responses were not forthcoming from the mother. These approving or mirroring responses were viewed by Kohut as essential for the child's development of a cohesive sense of self.
The second form of selfobject transference is the idealizing transference, where the patient maintains his or her self-esteem by being in the shadow of an idealized therapist. Basking in the reflected glory of the therapist makes the patient feel whole and worthy.
The third transference is called the twinship or alter-ego transference. This aspect of the self appears as a need to be just like the therapist. The developmental origin is a wish for merger that is gradually transformed into imitative behavior.
Inherent in the self psychological view is the notion that the development and maintenance of self-esteem is equally as important as sexuality and aggression as a motivating factor in human interaction. Moreover, Kohut (1984) felt that separation is a myth that does not reflect our actual need for affirming, empathic responses from others to feel a sense of wholeness throughout life. Eventually, Kohut viewed the self-selfobject connection as responsible for all forms of psychopathology. He viewed oedipal conflicts involving sexuality and aggression as mere ‘breakdown products’ of developmentally earlier failures involving lack of self or object responses.
Kohut was not clear on a developmental timetable for the difficulties in the sector of the self. However, he suggested that the self begins as fragmented nuclei and only achieves cohesiveness in response to empathic responses from parents. In the absence of those empathic responses, fragmentation of the self occurs, and the child tries to capture the sense of self through seeking out selfobject responses from others.
The self psychological perspective is consonant with the infant observation work of Daniel Stern (1985, 1989). The mothering figure's affirming and validating responses appear to be crucial to the developing infant's sense of self. The child has a sense of self-with-other in response to the caregiver's attunement from very early in infancy. Stern described five discrete senses of self, beginning with the development of a predominantly body self from birth to 2 months of age. A core sense of self emerges between 2 and 6 months. Between 7 and 9 months, the infant starts to have a greater sense of subjective self as intrapsychic states between infant and mother begin to be matched. When the child is approaching the middle of the second year of life, he or she has the capacity to think symbolically and to communicate verbally so a categorical or verbal sense of self emerges finally. A self with historical continuity, the narrative sense of self, arrives between 3 and 5 years of age.
John Bowlby was responsible for the development of attachment theory, largely in opposition to the existing psychoanalytic theories of his day. Nevertheless, in recent years attachment theory has begun to become integrated with the pluralistic edifice of psychoanalysis. Bowlby (1988) repeatedly emphasized the child's real experience and the importance of the external world in the child's healthy development. Borrowing from ethology, attachment behaviors were viewed by Bowlby as not reducible to another drive. An entire system of behaviors on the part of the child serve to optimize proximity to the mother or caregiver (Fonagy, 2001). In contrast to object relations thinking, the motivation of the child is not object seeking. Rather, the goal of the child is to achieve a psychophysiological state related to being in close proximity with the mother or caretaker. Holmes (2001) suggests that the same is true of adults, who, when stressed or threatened, may, if insecurely attached, resort to ‘pathological secure base phenomena,’ such as substance abuse, deliberate self-harm, or binge eating. These behaviors may re-create a shortcut to the physiological state of the secure base without its relational or psychological components.
The work of Ainsworth et al. (1978) was critically important in refining the attachment concept by studying the infant's response to what was called the Strange Situation. In this 20-minute laboratory test, a child is exposed to brief separations from the child's mother. The reaction to these separations led to a classification of children as securely attached, anxious-avoidantly attached, anxious-ambivalent or resistant in the attachment style, or disorganized/disoriented.
Although there is not a one-to-one correlation necessarily between the categories of child attachment and those of adults, attachment theorists have found it clinically useful to think of adult individuals in four somewhat analogous categories of attachment: (1) secure/autonomous individuals who value attachment relationships; (2) insecure/dismissing individuals who deny, devalue, idealize, or denigrate both current and past attachments; (3) preoccupied adults who are overwhelmed or confused by current and past attachment relationships; and (4) disorganized or unresolved individuals who have often suffered neglect or trauma. Compared with other psychoanalytic schools of thought, there is much more rigorous empirical research behind attachment theory. Some of this research demonstrates that expectant parents' mental models of attachment predict subsequent patterns of attachment between mother and infant (Fonagy, 2001). A key concept in attachment theory is mentalization, the capacity to understand that one's own behavior and that of others is motivated by internal states, such as thoughts and feelings (Fonagy, 1998). In addition, part of mentalization is an understanding that one's perceptions of others are representations rather than the way reality actually is. The mother's or caregiver's capacity to observe the infant's intentional state and internal world appears to influence the development of secure attachment in the child. The child's secure attachment to the caregiver is highly influential in the child's development of the capacity to mentalize.
In recent years a number of theoretical models that emphasize the two-person nature of psychoanalytic treatment have emerged. These various approaches, with labels such as intersubjectivity, relational theory, constructivism, or interpersonal psychoanalysis, all endorse skepticism about any fundamental truth residing in the patient or in the analyst. The truth is co-constructed in the interaction between therapist and patient. They are all postmodernists in outlook in that they doubt the existence of an objective reality ‘out there’ (Holland, 1983; Leary, 1994; Aron, 1996).
Renik (1993), for example, stresses the irreducible subjectivity of the analyst in the way that the analyst approaches listening and formulating interventions. The treatment situation is intersubjective in that the psychoanalytic therapist can never fully transcend his or her own unconscious motivations for attempting to help the patient. In a similar vein, the postmodernist perspective recognizes that the appearance of the patient's pathology is heavily influenced by the culture, gender, and personal biases of the therapist. The constructivist point of view stresses that we should be hesitant about regarding the patient's transference as a ‘distortion,’ in that it may be a plausible construct based on the patient's recognition of real aspects of the analyst's behavior (Hoffman, 1983, 1991).
The principles of technique in psychoanalytic psychotherapy have evolved considerably over the years. The stereotype of the ‘blank screen’ therapist who is aloof and silent while the patient struggles has misled many to assume that passivity is the hallmark of the psychodynamic therapist. We now practice in a postblank-screen era in which the therapist is actively engaged in the process and recognizes the role of countertransference as much as transference.
The principles of technique vary somewhat according to the therapist's school of thought, but certain themes are universal. Psychodynamic therapists allow their patients to try to articulate the nature of their problems and set goals for what they would like to address in the course of the treatment. Then they invite their patients to say whatever comes to mind as they reflect on the problem. Patients inevitably run into difficulties when they attempt to speak freely to their therapist, and hence resistances to the process become the daily bread and butter of the dynamic therapist's work. As long ago as 1912, Freud made the observation that ‘the resistance accompanies the treatment step by step. Every single association, every act of a person under treatment must reckon with the resistance that represents a compromise between the forces that are striving toward recovery and the opposing ones’ (p. 103).
A dynamic therapist does not attempt to overcome resistances by insisting that the patient must say what comes to mind. Rather, they strive to understand the meaning of the patient's falling silent or feeling ashamed. In this exploration, dynamic therapists often discover that particular feelings about the therapist are responsible for the resistance. Indeed, transference fantasies about the therapist are a major source of resistance. Patients may wonder if their therapist will be critical of them if they speak their mind. They may also worry that they might hurt the therapist's feelings by saying something negative about the therapy. They may shut down because of concerns that the therapist's motives are other than pure—what if the therapist secretly wants to ridicule them for their foibles? As time goes on in the therapy, more and more of these unconscious concerns are made conscious with the therapist's help, who points out observations of which the patient may not be aware.
The way that the patient resists the process reveals a great deal about the patient's inner world. In 1914, Freud noted that the patient repeats in action what he or she cannot remember and verbalize. Hence the way the patient relates to the therapist—how the patient enters the room, sits in the chair, breaks eye contact with the therapist, and what the patient chooses to call the therapist—all reveal aspects of the patient's internal object relations and unconscious attitudes toward the therapist.
As dynamic therapists begin to understand their patients, they try to enlist them in a collaborative pursuit of common therapeutic goals. This formation of a therapeutic alliance around understanding may be crucial to the success of the therapy. Therapists must help their patients ally themselves with the therapist's task of reflection and understanding. In the optimal situation, patients can observe themselves while also fully participating emotionally in the immediate experience of the therapeutic situation.
Many of the same principles that apply to the patient's optimal attitude also apply to the therapist. Just as patients have transference feelings that are a mixture of the real relationship with the therapist and old relationships from the past, therapists experience countertransference involving the same combination. The narrow, or Freudian, view of countertransference was that the analyst's unconscious conflicts about figures in the past are displaced on to the patient in the present. This view has now been superceded by a broader understanding of countertransference. Dynamic psychotherapists think of themselves as containers receiving a variety of projections from the patient. The patient induces certain feelings in the therapist that reflect the patient's internalized relationships. By studying how they feel in response to the patient's projections, therapists start to gain an understanding of how other people feel in relationships with the patient. Therapists must allow themselves to be sufficiently flexible so that they can experience the patient's effort to draw them in to familiar patterns of object relationships. In so doing they are privy to a firsthand experience of the patient's characteristic difficulties with others and can help the patient understand how they are repeating in the present characteristic patterns from the past that are also typical of current relationships.
Terms such as neutrality, abstinence, and anonymity may be misleading in that they can be misconstrued as promoting an aloofness or coldness. These principles of technique have undergone considerable transformation, and all three should now be applied only in a relative sense. In other words, therapists are neutral to the extent that they try to remain nonjudgmental about the patient's feelings, wishes, and behaviors in the service of understanding them. Therapists are abstinent in the sense that they do not gratify the patient's every transference wish because they wish to understand it rather than simply indulge it. Therapists certainly provide a good deal of gratification in their warmth and humanity, their laughter in response to a joke, their creation of a holding environment, and their empathic listening (Gabbard, 2000a,b).
Anonymity, especially, has undergone transformation in the way that modern psychodynamic psychotherapists construe the term. Therapists are revealing things about themselves all the time—by the way their office is set up, the way they react to what the patient says, through nonverbal communications such as facial expressions, and by their choice of when to speak versus when to remain silent. They may also self-disclose certain countertransference feelings they are noting within the session in the service of helping patients to understand what they evoke in the therapist and others. Anonymity today is best understood as a form of restraint based on the asymmetry of the therapeutic relationship. Therapists do not talk about their personal problems or their private lives with their families because they are paid a fee or a salary to focus on the patient's issues. Too much personal disclosure can burden the patient. The traditional view of anonymity was that the therapist should be like a ‘blank screen’ so that the therapist's real characteristics would not ‘contaminate’ the patient's transference. Whatever the therapist does has a continuing impact on the patient's transference so that it is impossible for the therapist to avoid influencing the patient's transference. A spontaneous, natural, warm approach to the patient is much more likely to facilitate a good therapeutic alliance than a remote, silent, aloof posture. We also know that the patient's internal object relations and intrapsychic conflicts will emerge to some degree, regardless of the therapist's behavior.
Spontaneity is certainly a key factor in the therapist's optimal attitude. Psychodynamic therapists allow themselves to be ‘sucked in’ to the patient's internal world by engaging in the ‘dance’ that the patient evokes in the consulting room. An example will illustrate one variation of this phenomenon.
A 30-year-old man came to see his therapist for the first time, and he began by asking him how many patients he had treated. The therapist responded that he did not know the exact number but was curious why the patient asked. In response to this comment, the patient said, ‘Oh, I see, you're one of those therapists who turns questions around to the patient so that you never answer anything.’ The therapist responded, ‘Well, I wouldn't go that far. I do sometimes answer questions if I think it will be useful.’ The patient then commented, ‘You sound like you're getting defensive now.’ The therapist replied, ‘No, I don't think I'm being defensive. I'm simply trying to clarify my position.’
At this point the therapist found himself getting irritated by the way he was being challenged by the patient and recognized that he had been drawn in to a particular dance that was typical of this patient, who complained that many of his friends and colleagues found him to be irritating.
In this example the therapist does not hold himself aloof from the patient's influence but rather serves as a container so that he can fully experience what the patient induces in him while also maintaining the capacity to reflect on what is happening between them. As Gabbard and Wilkinson (1994) note: ‘The optimal state of mind for therapists is when they can allow themselves to be “sucked in” to the patient's world while retaining the ability to observe it happening in front of their eyes. In such a state, therapists are truly thinking their own thoughts, even though they are under the patient's influence to some extent’ (p. 82). This process involves engaging in minor countertransference enactments, in which therapists may feel themselves becoming an object or self-representation within the patient's inner world, followed by a process of working back to thinking one's own thoughts and understanding the enactment in the context of the therapeutic situation.
The dynamic therapist also tracks the affects of the patient. Does anxiety or sadness emerge when the patient's father is discussed? Is there a flash of anger when the patient speaks of demands associated with a sibling's illness? A specific intrapsychic conflict may be heralded by the emergence of affect. Dynamic therapists are equally interested in defenses brought to bear to deal with affect states or drive derivatives. When expression of anger, for example, is stifled by a defensive flight from the subject that evoked the anger, therapists may call attention to the patient's conflict and the defensive strategy used to deal with it (Gray, 1990).
A basic principle of psychoanalytic therapy is working through. Calling attention to affect states, defenses, and resistances and understanding their meaning all take time. Freud (1914) noted, ‘One must allow the patient time to become more conversant with this resistance with which he has now become acquainted, to work through it, to overcome it, by continuing, in defiance of it, the analytic work…’ (p. 155). The therapist must be prepared to address the same conflicts, the same resistances, and the same transferences as they surface in a variety of different situations, both within the therapeutic relationship and outside the consulting room. Only through repetitive interpretation, observation, and confrontation will the patient finally gain a sense of mastery over a host of haunting internal conflicts and the ‘ghosts’ responsible for them. Freud (1914) stressed that this working-through process is what distinguishes the psychoanalytic approach from therapies based on suggestion. It also is one of the reasons that dynamic therapy is usually long term or open ended. A significant exception is brief dynamic therapy, but that modality is covered elsewhere in this volume.
Psychodynamic psychotherapy occurs in the context of a frame that assures ethical behavior on the part of the therapist. By adhering to the frame, the enactments occur in an attenuated way that does not threaten harm or exploit the patient. The frame is constituted by a set of professional boundaries that define the limits of a professional relationship and differentiates it from a friendship, a romantic relationship, or a parent–child relationship. Included in these boundaries are the therapist's office, the time frame of 45 or 50 minutes, professional dress and demeanor, limited self-disclosure on the part of the therapist, the acceptance of a fee for a service (or a salary, if publicly funded), confidentiality, and no physical contact. The central point of this asymmetrical relationship is that the therapist's entire focus is on helping the patient with the problems the patient brings to therapy.
Boundaries should not be construed rigidly. Many variations on boundary transgressions occur, some of them benign and even helpful. If a patient falls down entering the office, a therapist may help the patient up. In some cases, therapists may answer personal questions or extend the session. These minor transgressions are referred to as boundary crossings (Gutheil and Gabbard, 1998) because they occur in isolation, are attenuated in such a way that no harm is done, and are often explored in the therapy itself. The more egregious boundary transgressions, such as sexual misconduct, are referred to as boundary violations because they are exploitative of the patient's vulnerability, may harm the patient, and destroy the viability of the therapy.
Psychodynamic psychotherapy is often referred to as expressive-supportive psychotherapy. This designation reflects the fact that with any one patient, the therapist may be more expressive or exploratory at some times while shifting to a more supportive or suppressive style at another, depending on the patient's needs. Dynamic psychotherapy that is predominantly exploratory or expressive is oriented to analyzing defenses, transference, and intrapsychic conflicts and to making more of the patient's unconscious available to conscious awareness. Supportive or suppressive psychotherapy aims to bolster or strengthen defenses and suppress unconscious conflict. Although psychodynamic psychotherapy as a treatment generally connotes an expressive or exploratory emphasis, supportive interventions are used regularly in such treatments.
The types of interventions that predominate in highly expressive dynamic therapy are interpretation, observation, and confrontation. Interpretations are statements made by the therapist that attempt to explain the patient's thoughts, feelings, behaviors, or symptoms. They link these phenomena to unconscious fantasies, meanings, or childhood origins. An experience that occurs in the therapy that relates to the therapist may be linked to parallel situations outside the consulting room and past situations from long ago. A therapist might use the following transference interpretation to help a patient make unconscious motivations consciously available: ‘I wonder if you find it necessary to disagree with any observation I make as a way of defeating the therapy and by implication, triumphing over your dad as well.’ Wishes and defenses against those wishes are often the subject of interpretation, and these conflicts can be interpreted as they appear in the transference, childhood memories, and current relationships (Malan, 1976; Gabbard, 2000a).
Observation calls attention to a behavior, the sequence of a comment, a flash of emotion, a pattern within the therapy, or similar phenomena (Gabbard, 2004). Unlike interpretation, observation does not attempt to explain or identify motives. The therapist hopes the observation will lead to a collaborative exploration of meanings. A therapist might say, for example, ‘I don't think you're aware of it, but you often grimace when I ask about your mother.’
Confrontation involves an attempt to make the patient face something that he or she is avoiding. While confrontation may have an aggressive connotation, this type of intervention can be delivered gently as well. After a patient's mother died, the therapist noticed that the patient completely avoided the topic of his mother's death. The therapist chose a well-timed moment to point this out: ‘I know it's a difficult subject for you, but I don't think you've spoken about your mother a single time since her funeral.’ Whereas observation generally focuses on nonverbal communications or patterns that are outside the patient's awareness, confrontations generally target behaviors or topics that are conscious but avoided (Gabbard, 2004).
At the more supportive end of the continuum, therapists may give specific advice to patients on how they should live their lives, how they should decide to behave in a specific situation, or whether they should leave a relationship in which they are involved. Advice giving is unusual in exploratory therapy and sharply distinguishes supportive from expressive therapy. Praise is also used in supportive or suppressive therapy to reinforce certain behaviors or thoughts by approving them. Affirmation is another intervention associated with therapies that are predominantly supportive. In such treatments, therapists make comments such as, ‘I don't blame you a bit for feeling the way you do,’ or ‘you are absolutely right to be angry.’ Defenses may be bolstered by such comments as: ‘I think you should continue to act kindly to your mother even though you are secretly angry at her.’ In this example the therapist reinforced the patient's reaction formation because the patient had a history of getting out of control when expressing anger.
In between the more expressive and supportive interventions are a number of therapist's comments that are used in all dynamic therapies. Empathic validation, particularly associated with self psychological therapists, involves placing oneself in the patient's shoes and attuning oneself to the patient's internal state. This empathic immersion in the patient's inner world helps one to understand feelings, thoughts, or behaviors from the patient's perspective. An example of a comment that is empathically validating is the following: ‘I can certainly appreciate why you would feel hurt by your boss's behavior toward you because you had worked hard on the project and expected some recognition.’
Much of psychotherapy involves facilitating the patient's exploration of a particular subject. Hence therapists probably use encouragement to elaborate more than any other intervention. Examples include, ‘Please tell me more about that; I'm very interested in it.’ Other comments may be more specific: ‘At what point in your adolescence did you feel that you really had to leave home?’ Sometimes encouragement to elaborate is needed because the patient's communication is confusing: ‘Could you please explain to me why you and your previous therapist decided you couldn't work together anymore?’
Clarification is a third intervention that resides in the middle of the expressive-supportive continuum and may take a variety of forms. In dynamic psychotherapy a clarification is often designed to repackage something the patient has said as a way of summarizing key points that the patient is making (Gabbard, 2000a). Clarification may be a way of checking out with the patient if the therapist's understanding is correct. It may also be a way of helping the patient recognize patterns: ‘The more I hear you talk, the more I realize that you're basically mad at your mother, your sister, and your girlfriend.’ It may also be a way of helping the patient get in touch with specific feelings that are being avoided: ‘When you talk about the loss of your boyfriend, I can see that you miss him and are saddened by it even though you'd like to mainly focus on the anger.’
Frequency and transference focus are also a function of the expressive-supportive continuum. Patients who are suited for highly expressive treatment may make greater progress with more than one session per week and more emphasis on transference issues. Patients needing a supportive approach may benefit from sessions less than once per week and avoidance of addressing transference themes.
The goals of psychodynamic psychotherapy are multiple. One basic goal is to expand the patient's awareness of unconscious conflicts, feelings, wishes, fantasies, and motivations. Psychodynamic therapists look for patterns in work or school and in relationships. How do past patterns of relatedness get repeated in the present, both with the therapist and in life outside the consulting room? What recurrent conflicts inhabit the patient in work or school settings? The therapist seeks to formulate interpretations of these unconscious patterns. Another goal is to increase the patient's awareness of problematic attachment patterns so new and different modes of attaching to others are possible.
One of the overall goals of dynamic psychotherapy is to help patients ‘live in their own skin’ (Gabbard, 1996). Therapists try to help patients understand how they lie to themselves, hide from themselves, and try to project their own conflicts and feelings on to others. From a Kleinian and object relations perspective, therapists interpret how certain aspects of the self have been disavowed and projected on to others so the patient can ultimately take back what has been externalized. Self psychological psychotherapists try to strengthen the patient's self-esteem so that these patients are able to endure slights and narcissistic injuries with greater equanimity.
While most of these goals are more geared to the expressive end of the continuum, patients who have greater deficits may require more supportive strategies with more limited goals. Patients with borderline personality disorder, for example, may need supportive and validating comments to tolerate interpretation (Gabbard, 2000a). They may also need explicit support from the therapist to improve certain ego deficits, such as the capacity for judgment. Therapists may systematically help such patients think through the consequences of their actions to avoid making poor judgments. They may also help them delay impulsive actions by pointing out feelings that trigger the actions. Another goal may be to help the patient deal with internal deficits by providing active soothing or comforting to replace what is missing in the patient's internal world.
Psychodynamic therapists carefully assess each patient to determine whether the emphasis should be predominantly expressive, predominantly supportive, or a mixture of both. Several characteristics suggest that the patient will be responsive to more exploratory approaches. Those patients who are strongly motivated to understand themselves because they are suffering are more suited to an exploratory approach. Other ego strengths auger well for expressive treatment: intact reality testing, good impulse control, a high tolerance for frustration, and a general reflectiveness or psychological mindedness that leads the patient to think about internal motivations for behaviors. Meaningful and enduring interpersonal relationships, above-average intelligence, and a capacity to see parallels between situations in different contexts are also indications for dynamic therapy with an expressive emphasis. Patients who lack these characteristics may require more supportive approaches. In general, a person who is in the throes of a severe life crisis will need support even if ordinarily the person might be suited for a more dynamic approach. Brain-based cognitive dysfunction may also prevent a person from being able to use exploratory therapy. Even patients who are significantly disturbed may benefit from highly expressive therapy, however, if the therapist is sufficiently skilled to provide support, when necessary, in the areas of the patient's deficits.
How does psychodynamic therapy work? Where once upon a time the complete focus was on interpretation of unconscious conflict, almost all psychoanalytic therapists now recognize that there are multiple modes of therapeutic action that vary from patient to patient (Gabbard and Westen, 2003). Fostering insight and the therapeutic relationship itself are probably the primary modes by which change is brought about in psychoanalytic therapy.
Historically, one of the ways that insight has been fostered is to encourage free association. By having the patient say whatever comes to mind, the therapist can demonstrate to the patient how ideas are linked unconsciously through the network of associations. Interpretation is another way to make unconscious wishes, fears, or fantasies more consciously available. The dynamic therapist hopes to instill a way of thinking in the patient's mind so that following termination, the patient continues to do ‘self-analytic’ or ‘self-therapeutic’ work to understand anxiety, depression, or conflict as it emerges posttermination period.
Freud (1915) once noted that the analyst pursues a course ‘for which there is no model in real life’ (p. 166). There is undoubtedly a corrective effect of experiencing a new and different kind of relationship for the patient. When therapists behave differently from what patients expect, the patients must come to grips with the way that they have imposed certain internal expectations on external figures.
Over time the patient internalizes the relationship with the therapist. Soon the internalization process modifies representations that have been present since childhood. Our representations of self and other are etched in neural networks based on childhood experiences (Westen and Gabbard, 2002a,b). These representations are potentials that are activated by situations in external reality that are similar in some way to these internalized self- and object representations. For example, a child who grew up beaten by his father will expect an older male therapist to be violent or critical. When that therapist is calm and caring, the neural network associated with the abusive father and the abused son will gradually be modified in its intensity. While the neural network will not completely disappear, it is weakened because it is now being surpassed by a new neural network involving a representation of an understanding and patient object and a self that feels understood. In keeping with the alteration of representations, the patient also internalizes emotional attitudes of the therapist so that the affect linkage between representations may have a different emotional valence.
Blatt and Auerbach (2001) used the Differentiation-Relatedness Scale to study 40 seriously disturbed treatment-resistant young adults and adolescents. These patients were evaluated at the beginning and end of psychoanalytically oriented inpatient treatment that lasted more than 1 year. Over the course of treatment, internal self- and object representations underwent significant changes. Prior to treatment, these representations were dominated by splitting and polarization, while after treatment, in concert with improved clinical functioning, there were more integrated descriptions of self and others, reflecting a move in the direction of the consolidation of object constancy. Hence the developmental level of mental representations changed significantly with intensive psychoanalytic treatment in an inpatient setting.
Yet another way that the therapeutic relationship may catalyze change is through internalization of the therapist's capacity for mentalization as measured by improved reflective functioning (Fonagy and Target, 1996). Patients who lack the capacity for mentalization related to early attachment problems have difficulty understanding the idea that mental states motivate behavior. Similarly, they have difficulty understanding how the minds of others work. Through the psychotherapeutic relationship, patients may ‘find themselves’ in the therapist's mind and improve their ability to distinguish representations from external reality. As a result of this improved capacity, patients can then understand both their own mental states and those of others. This capacity may improve in concert with the increased developmental level of internal representations (Blatt and Auerbach, 2001).
The mode of therapeutic action inherent in the therapeutic relationship should not be misconstrued as a simple matter of conscientiously behaving differently than objects from the past (Gabbard and Westen, 2003). To effect change, patients must perceive their therapist as sufficiently similar to the past objects that the core neural networks are activated. Then patients have the opportunity to work through the old representations and affect states that have been problematic to them. The characteristic self-other patterns must come to life in the relationship with the therapist.
In addition to the primary modes of therapeutic action—the fostering of insight and the therapeutic relationship—a variety of secondary strategies are brought to bear in a typical course of psychodynamic therapy (Gabbard and Westen, 2003). Despite the history of eschewing suggestion by psychoanalytic writers, there is little doubt that explicit or implicit suggestions for change accompany most treatments. Problematic beliefs of the patient may be confronted because they are clearly related to behaviors that are self-defeating in one way or another. In addition, therapists may help patients examine conscious methods of decision making or problem solving that create difficulties for them. Even exposure, which is classically associated with behavior therapy, occurs in psychodynamic treatments to some degree. As Fonagy and Target (2000) have emphasized, helping patients to differentiate belief from fact is a form of exposure in that the therapist acknowledges the patient's psychic reality of fear while simultaneously offering an alternative perspective that suggests safety. Moreover, transference anxieties diminish over time in part because of the exposure inherent in the psychotherapeutic situation. For example, patients ultimately realize that their fears of being humiliated or criticized by the therapist are unrealistic as their exposure to the therapist increases.
Some changes undoubtedly occur outside the realm of planned technical interventions. Specific moments of mutual recognition—a tear in the therapist's eye, a shared belly laugh—that are not symbolically represented may have a powerful therapeutic impact (Stern et al., 1998). These changes may occur in the realm of implicit procedural knowledge involving how to feel, think, or behave in a specific relational context.
Two other secondary strategies are worth noting. In recent years, self-disclosure by the therapist in a limited way has become a common intervention. Judicious self-disclosure may promote increased reflective function by helping the patients see that their representation of the therapist is different from the way the therapist actually feels (Gabbard, 2001). Self-disclosures of here-and-now countertransference feelings may also help patients understand the impact they have on others (Gabbard and Wilkinson, 1994). In addition, an affirmation process goes on in most dynamic therapies where patients feel that their point of view is valued and validated. This empathically validating function of the therapist may serve to mitigate longstanding feelings of being disbelieved or dismissed by earlier figures in one's life.
Psychoanalysts and psychodynamic therapists have historically been far too complacent about demonstrating the efficacy of their treatments. In some respects, the scarcity of efficacy data based on randomized controlled trials is understandable in light of the unique methodological problems associated with studying long-term psychoanalytic treatment (Gabbard et al., 2002). A long-term follow-up study would be prohibitively expensive as the project would have to persist for 10 years or more to accumulate a large enough sample so that statistically valid analyses would be possible. A suitably matched control group would also be difficult to recruit. Self-selection of treatment is considered important to analysts and analytically oriented therapists because of the motivation necessary to engage in psychodynamic exploration. Patients who are not given the treatments they prefer might well drop out of a randomized, controlled study. Indeed, a substantial number of dropouts would create major problems for a long-term study. Finally, over a period of a decade, uncontrolled variables, such as life events, serious illness, medication changes, and the comorbidity with Axis I disorders might well effect the meaningfulness of the results (Gunderson and Gabbard, 1999).
The psychodynamic approach has been given credibility by a substantial body of research on brief psychodynamic therapy. In a recent meta-analysis to assess the efficacy of short-term psychodynamic psychotherapy (STPP), (Leichsenring et al., 2004) included only randomized controlled trials that fulfilled rigorous criteria. They found that STTP yielded large and significant effect sizes for social functioning, general psychiatric symptoms, and target problems, and these improvements tended to increase at follow-up. These effect sizes significantly exceeded those of treatment as usual and waiting list control. They also found that there were no differences between STPP and other forms of psychotherapy.
When we examine psychoanalysis and intensive psychoanalytic therapy, we find a small number of outcome studies with the rigor of a randomized controlled design. In the Boston Psychotherapy Study (Stanton et al., 1984), patients with schizophrenia who received supportive therapy were compared with those who were provided with psychoanalytic therapy at a frequency of two or more times a week by experienced psychoanalytically oriented therapists. While certain outcome measures seemed to improve differentially in each group, overall no significant advantage was conferred on patients who were treated with psychoanalytic therapy (Gunderson et al., 1984).
A study of psychoanalytic therapy (three to four sessions per week) for 11 hospitalized diabetic children had profound and lasting effects on their health compared with a comparable sample of diabetic children who received standard medical treatment (Moran et al., 1991). The treatment lasted only 15 weeks, so the study is relevant to intensive psychoanalytic therapy but not to the study of extended psychoanalytic therapy.
Heinicke and Ramsey-Klee (1986) compared intensive psychoanalytic psychotherapy (four times a week) with once-a-week sessions for children with learning difficulties. This randomized controlled trial involved treatments lasting more than a year. The children who were seen once a week showed a greater rate of improvement than those receiving four times weekly sessions. At the time of follow-up, however, the children who had four times weekly sessions showed much greater improvement.
In a more recent study, 38 patients with borderline personality disorder were randomly assigned to a psychoanalytically oriented partial hospital treatment or to standard psychiatric care as a control group (Bateman and Fonagy, 1999). The primary treatments in the partial hospital cell consisted of once weekly individual psychoanalytic psychotherapy and three times weekly group psychoanalytic psychotherapy. The control subjects received no psychotherapy. At the end of treatment at 18 months, the patients who received the psychoanalytically oriented treatment showed significantly more improvements in depressive symptoms, social and interpersonal functioning, need for hospitalization, and suicidal and self-mutilating behavior. These differences were maintained during an 18-month posttreatment follow-up period with assessments every 6 months (Bateman and Fonagy, 2001). Moreover, the treatment group continued to improve during the 18-month follow-up period.
Svartberg et al., (2004) randomly assigned 50 patients with cluster C personality disorders to 40 sessions of either dynamic psychotherapy or cognitive therapy. The full sample of patients showed statistically significant improvement on all measures during treatment and during the 2-year follow-up. Patients who received cognitive therapy did not report significant change in symptom distress after treatment, whereas patients who underwent dynamic therapy treatment did. Two years after the treatment, 54% of the dynamic therapy patients and 42% of the cognitive therapy patients had recovered symptomatically. The researchers concluded that improvement continues after treatment with dynamic psychotherapy.
In Sweden the Stockholm Outcome of Psychoanalysis Psychotherapy Project (Sandell et al., 2000) was able to follow up a large number of patients treated with psychoanalysis and psychoanalytic therapy that was subsidized by national health insurance and provided by private practitioners. This study can best be categorized as a large prepost design. Random assignment was attempted but was unsuccessful. Some patients refused to be assigned, and others who agreed to be assigned did not get the treatment they preferred, so they sought it privately. The patient sample included 756 persons who were subsidized for up to 3 years in psychoanalysis or psychotherapy or on the respective waiting lists for subsidization of those treatments. Complete data for three panel waves were obtained from a group of 331 persons in various phases of long-term psychodynamic psychotherapy and from a group of 74 persons in various phases of psychoanalysis. The psychoanalytic treatments were defined as occurring four to five times a week, while psychotherapy consisted of one to two sessions per week. In measurements of symptomatic outcome using the Symptom Checklist 90, improvement during the 3 years after treatment was positively related to treatment frequency and duration, with patients in psychoanalysis doing better than those in psychoanalytic psychotherapy. This finding may be confounded, however, by the possibility that the psychoanalysts doing once or twice weekly psychotherapy were not conducting their preferred modality. Patients in psychoanalysis continued to improve after termination, a finding not generally noted in outcome studies of other psychotherapies.
Another large prepost study of 763 children who were evaluated and given psychoanalytic treatment at the Anna Freud Centre in London, UK, yielded data that suggested which patients were more likely to benefit from analysis (Target and Fonagy, 1994a, b). Children with phobias appeared to benefit significantly from psychoanalysis, while those with depression did not. Children with severe emotional disorders (three or more Axis I diagnoses) did surprisingly well in psychoanalysis, but they did poorly in once or twice a week psychoanalytic psychotherapy. Children with conduct problems did consistently worse than children with emotional difficulties of equal severity. Children younger than 12 years made more impressive gains with intensive treatment at four to five times per week than with nonintensive treatment at one to three times per week. Adolescents, on the other hand, did not appear to benefit from increased frequency, but the duration of the treatment was correlated with better outcomes. This study nicely illustrates how the findings of research are likely to surprise and inform clinical practitioners.
Several prospective follow-along studies using a prepost design have suggested substantial improvements in patients given psychoanalytic therapies for personality disorders (Stevenson and Meares, 1992; Høglend, 1993; Monsen et al., 1995a,b). Additional data (Stevenson and Meares, 1995) from one of these studies suggest that gains from 1 year of dynamic therapy were maintained at 5-year follow-up. Uncontrolled studies, however, particularly those with relatively small sample sizes and clinical populations whose condition is known to fluctuate wildly, cannot yield data of consequence concerning what type of treatment is likely to be effective for whom.
Psychodynamic psychotherapy is probably the most widely practiced and most well-known form of therapy. Based on psychoanalysis, its unique features include an emphasis on unconscious mental life, systematic attention to transference themes and developmental issues, the exploration of countertransference as an important therapeutic tool, and the working through of resistance, defense, and conflict.
The empirical basis of extended psychoanalytic therapy is far from adequate, but preliminary research is encouraging. Because this form of therapy requires a greater investment of time and money than many other therapies, it should probably be used primarily for conditions that are not likely to respond to brief therapy and/or medication. Patients with complex and longstanding difficulties, especially those firmly entrenched in their character, will probably require open-ended psychoanalytic therapy to make significant gains.