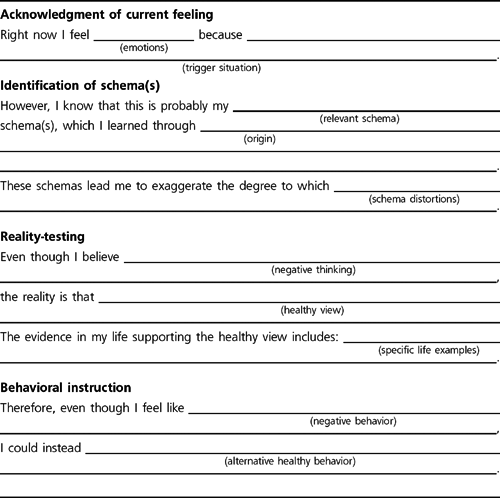
FIGURE 3.1 Schema Therapy Flash Card.
Cognitive techniques in schema therapy include the following:
Testing the validity of a schema
Reframing the evidence supporting a schema
Evaluating the advantages and disadvantages of the patient’s coping styles
Conducting dialogues between the “schema side” and the “healthy side”
Constructing schema flash cards
Filling out Schema Diary forms
The therapist typically goes through the cognitive techniques with patients in the order we have listed them here, as the techniques build on one another.
The therapist and patient test the validity of a schema by examining the objective evidence for and against the schema. This process is similar to testing the validity of automatic thoughts in cognitive therapy, except that the therapist uses the patient’s whole life as empirical data and not just the present circumstances. The schema is the hypothesis to be tested.
The therapist and patient make a list of evidence from the past and present supporting the schema; then they make a list of evidence refuting the schema. Patients usually find it remarkably easy to compose the first list, evidence supporting the schema, because they already believe this evidence. They have been rehearsing it all their lives. Generating evidence that supports the schema feels natural and familiar to them. In contrast, patients usually find it extremely difficult to compose the second list, evidence refuting the schema, and frequently require a good deal of input from the therapist, because they do not believe the evidence against the schema. They have spent their lives ignoring or downplaying this evidence. They do not have ready access to this evidence as a result of schema perpetuation, which has continuously induced them to accentuate information confirming the schema and negate information contradicting the schema. The discrepancy between the patient’s ease at playing the schema side and difficulty playing the healthy side often proves highly instructive to the patient. The patient observes firsthand how the schema works to preserve itself.
To illustrate this technique, we examine one patient’s evidence regarding her Defectiveness schema. Shari is 28 years old, married with two children, and works as a psychiatric nurse. Her Defectiveness schema originated in her childhood with her alcoholic mother. (Her father divorced her mother and left the family when Shari was 4 years old. Although he provided money, Shari rarely saw him after that.) Throughout her childhood, her mother frequently humiliated her by appearing intoxicated in public places. She once came drunk to one of Shari’s school plays and disrupted the performance. Shari avoided bringing friends home out of fear of what her mother might do. Her home life was barren and chaotic.
Here is Shari’s list of evidence that she is defective:
I’m not like everyone else. I’m different and always have been.
My family was different from other families.
My family was shameful.
No one ever loved me or cared for me when I was a child. I never belonged to anyone. My own father didn’t care to see me.
I’m awkward, stilted, obsessive, afraid, and self-conscious with other people.
I’m inappropriate with other people. I don’t know the rules.
I’m fawning and pandering with other people. I need acceptance and approval too much.
I get too angry inside.
It is important to mention that, despite Shari’s critical appraisal of her social ability, she is actually highly socially skilled. Her problem is one of social anxiety, not one of social skills.
Not surprisingly, Shari found it extremely difficult to compose the second list, evidence refuting the schema. When it came to this part of the exercise, she could not think of anything to write down at all. She sat there bewildered and silent. Even though she is both personally and professionally successful and has a multitude of commendable traits, she could not think of a single positive quality to ascribe to herself. The therapist had to suggest every one.
The therapist asks leading questions designed to draw from the patient the evidence against the schema. For example, if a patient has a Defectiveness schema such as Shari does, the therapist might ask, “Has anyone ever loved you or liked you?” “Do you try to be a good person?” “Is there anything at all good about you?” “Is there anyone you care about?” “What have other people told you is good about you?” Such questions—often worded in an extreme manner—spur the patient to generate positive information. The therapist and patient gradually develop a list of the patient’s good qualities. Later the patient can use this list to counter the schema.
Here is the list Shari compiled with the help of her therapist.
My husband and children love me.
My husband’s family loves me. (My sister-in-law asked me to take her children if she and my brother-in-law died.)
My friends Jeanette and Anne Marie love me.
My patients like and respect me. I get really good feedback from them pretty much all the time.
Most of the staff at the hospital likes me and respects me. I get good evaluations.
I’m sensitive to other people’s feelings.
I loved my mother, even if she cared about drinking more than she cared about me. I was the one who was there for her until the end.
I try to be good and do the right thing. When I get angry, it’s for good reason.
It is important for the therapist to write down the evidence against the schema, because patients tend to quickly dismiss or forget it.
Shari is fortunate, because there is an abundance of evidence against her Defectiveness schema. Not all patients have such good fortune. If there is not much evidence to contradict the schema, the therapist acknowledges it, but says, “It doesn’t have to be this way.” For example, a male patient with a Defectiveness schema might actually have very few loving people in his life. Through surrendering to the schema (choosing significant others who are rejecting and critical), avoiding the schema (staying out of close relationships), or overcompensating for the schema (treating others arrogantly and pushing them away), the patient might look back on a whole life without love. The therapist says,
“I agree you haven’t developed loving relationships in your life, but it’s for a good reason. It’s because of what happened to you as a child that it’s been so hard for you. Because you learned very young to expect criticism and rejection, you stopped reaching out to people. But we can change this pattern. We can work together to help you choose people who are warm and accepting and let them become part of your life. You can work on gradually getting close to some of these people and letting them gradually get close to you. You could try to stop denigrating yourself and others. If you take these steps, things could be different for you. This is what we’ll work on in therapy.”
As therapy progresses and the patient develops a greater ability to form close relationships, the therapist and patient can add new information to the list of evidence against the schema.
As another step in this process of examining the evidence, patients look at how they discount the evidence against the schema. They write down how they negate evidence. For example, Shari listed the ways she discounts the evidence against her Defectiveness schema.
I tell myself that I’m fooling my husband and children, and that’s why they love me. They don’t know the real me.
I do more for my family and friends than they do for me, and then I feel like that’s the only reason they care about me.
When people give me good feedback, I don’t believe them. I think that there’s some other reason they’re saying it.
I tell myself that I’m only sensitive to people’s feelings out of weakness. I’m afraid to assert myself.
I get down on myself for getting angry and resentful while I was taking care of my mother.
After writing down how they negate evidence, patients “reclaim” the evidence against the schema. The therapist shows how invalidating the evidence against the schema is simply another form of schema perpetuation.
The next step is to take the list of evidence supporting the schema and to generate alternative explanations for what happened. The therapist takes events the patient views as proving the schema and reattributes them to other causes. The goal is to discredit the evidence supporting the schema.
The therapist discounts early childhood experiences as reflecting pathological family dynamics, including poor parenting, rather than the truth of the schema. The therapist points out any activities that occurred within the family that would not have been acceptable in healthy families. In addition, the therapist and patient consider the psychological health and character of the parents (and other family members) one by one. Did the parent truly have the patient’s best interests at heart? What role did the parent assign to the patient? The therapist points out that parents often assign roles to children that do not serve the children’s needs but the needs of the parents. These roles do not reflect inherent flaws in the children, but instead reflect flaws in the parents. Did the parent use the patient in any selfish way? The therapist goes on exploring in this fashion until patients shift to a more realistic perspective of their family history. They stop viewing their early childhood experiences as proof of their schemas.
For example, one item on Marika’s list of evidence supporting her Defectiveness schema was, “My father didn’t love me or pay attention to me.” Marika attributed her father’s lack of love to her inherent unlovability: He did not love her because she was unworthy of love. In her view, she was too needy. The therapist spent time exploring the patterns in Marika’s family of origin. Then the therapist suggested an alternative explanation: Her father was incapable of loving his children. In fact, he did not love her brother, either. Her father did not show love for her because of his own psychological limitations, not because she was unlovable. Marika’s father was narcissistic and incapable of genuine love. He did not have the ability to be a good father. A good father would have loved her. She was an affectionate child who wanted a close relationship with her father, but he could not have this kind of relationship.
The therapist discounts experiences since childhood that support the schema by attributing them to schema perpetuation. The coping styles patients learned in childhood have carried their schemas forward into their adult lives. The therapist notes that, because of their schema-driven behaviors, patients have never given their schemas a fair test. For example, another item on Marika’s list of evidence supporting her Defectiveness schema was, “All the men in my life have treated me badly.” She reported that she had had three boyfriends. One of them abused her, one left her, and one frequently slept with other women.
Marika believes that her boyfriends treated her badly because she is undeserving of respect and love, and they knew it. The therapist suggests an alternative explanation: Since she started dating as an adolescent and continuing until the present day, her Defectiveness schema has caused her to keep choosing partners who were critical and rejecting and who would thus treat her badly. (Partner selection is frequently an important aspect of schema perpetuation.)
THERAPIST: Well, let’s look at the type of people you chose. Did you choose partners who at the beginning you had reason to believe would be caring to you—loyal, committed, honest, loving people?
MARIKA: Well, no. Joel from the beginning was trouble. He was sleeping around.
THERAPIST: And how about Mark?
MARIKA: No, he had beaten up his previous girlfriend.
In sum, the therapist takes evidence supporting the schema and reframes it. If it is evidence from childhood, the therapist reframes it as a problem with the parents or family system. If it is evidence from the patient’s life since childhood, the therapist reframes it as schema perpetuation, which has turned the schema into a self-fulfilling prophecy in the patient’s life.
The therapist and patient study each schema and coping response individually and list its advantages and disadvantages. (The therapist and patient have already identified the patient’s coping styles in the Assessment and Education Phase.) The goal is for patients to recognize the self-defeating nature of their coping styles and to discern that, if they were to replace these coping styles with healthier behaviors, they could increase the chances for happiness in their lives. The therapist also points out that their coping styles were adaptive as children but are maladaptive as adults in the wider world outside their families or adolescent peer group.
For example, a young female patient named Kim has an Abandonment schema. She copes with her schema by using an avoidant coping style. She stays away from men by turning down most requests for dates and spending her free time alone or with her girlfriends. On the rare occasions that she goes out with men whom she likes, she ends the relationship abruptly after a few dates:
THERAPIST: So, would it be OK with you if we list the advantages and disadvantages of your coping style—of all the ways you avoid getting close to men and your history of ending promising relationships?
KIM: Yes. That sounds OK.
THERAPIST: So, what are the advantages, do you think? What do you gain by avoiding men and ending relationships prematurely?
KIM: That’s easy. I don’t have to go through the pain of being left. I leave them so they can’t leave me.
The advantage of Kim’s avoidant coping style is that it provides her with an immediate sense of control over what happens in her relationships with men. In the short run, she feels less anxious. The disadvantage, however, is significant: In the long run, she is alone. (As usual, attempts at schema avoidance result in schema perpetuation.)
THERAPIST: What are the disadvantages of avoiding men and breaking up with them when things are going well? What are the disadvantages of your coping style?
KIM: Well, one disadvantage is that I lose a lot of good relationships.
THERAPIST: How do you feel about losing your last boyfriend, Jonathan?
KIM: (pause) Relieved. I feel relieved. I don’t have to worry about it all the time anymore.
THERAPIST: Do you feel anything else about it?
KIM: Yeah, well, of course. I feel sad. I miss him. I feel sad that he’s gone. We were really close for a while.
The exercise helps Kim face the reality of her situation. If she continues with her current method of coping with her Abandonment schema, she will surely end up alone. However, if she is willing to tolerate her anxiety and commit to a promising relationship, then there is a possibility that she might get what she wants most: a relationship with a man who will heal, rather than reinforce, her Abandonment schema.
With the next cognitive technique, patients learn to conduct dialogues between their “schema side” and “healthy side.” Adapting the Gestalt “empty chair” technique, the therapist instructs patients to switch chairs as they play the two sides: In one chair they play the schema side, in the other they play the healthy side.
Because patients normally have little or no experience expressing the healthy side, the therapist first plays the healthy side and the patient plays the schema. The therapist might introduce the technique by saying: “Let’s have a debate between the schema side and the healthy side. I’ll play the healthy side, and you play the schema side. Try as hard as you can to prove that the schema is true, and I’ll try as hard as I can to prove that the schema is false.” Beginning this way gives the therapist the opportunity to model the healthy side for the patient and enables the therapist to come up with answers to whatever arguments the patient raises while playing the schema side.
Eventually the patient takes over the role of the healthy side, with the therapist acting as coach. Either the therapist or patient can play the schema side; when the patient plays both sides, the patient moves back and forth between two different chairs, each chair representing one side of the debate. At first the patient needs a lot of prompting from the therapist to come up with healthy responses. The therapist gradually withdraws into the background, however, as the patient more easily generates healthy answers. The goal is for patients to learn how to play the healthy side on their own, naturally and automatically.
In the following example, Dr. Young helps a patient conduct a dialogue between his Mistrust/Abuse and Defectiveness schemas and his “healthy side.” The patient is a 35-year-old man named Daniel, whom we present in greater detail in the next chapter on experiential strategies. Daniel had a traumatic childhood: His father was alcoholic, and his mother was sexually, physically, and emotionally abusive. At the time of his interview with Dr. Young, Daniel had been in traditional cognitive therapy with another therapist for about 9 months. He had sought therapy for social anxiety and anger-management problems. Daniel’s ultimate goal was to meet a woman and get married, but he both mistrusted women and expected them to reject him. He thus avoided social situations in which he might meet women.
In order to prepare the patient for the dialogue, Dr. Young began the session by helping the patient build a case against the schema. Dr. Young thus provided the patient with some ammunition to use against the schema side. In the following excerpt, Daniel plays both the schema side and the healthy side.
THERAPIST: What I’d like to do now is to have what I call a dialogue between the schema side, which feels women can’t be trusted and they’re not going to find you attractive, and then this healthy side that you’re trying to build up but which is still not as strong. Do you know what I’m saying?
DANIEL: Yes.
THERAPIST: So I’m going to ask you to go back and forth. Maybe you can start as if you’re in a room at a dance about to approach a woman, but you’re feeling avoidant, you want to run. First be the schema side that wants to run out and say what you’re afraid of.
DANIEL: (as the schema side) “I’m in a very nervous state and I’m sort of hoping that the dance will not be a success, and that, contrary to what I’ve heard, that there’s always more women than men at the dances, that the reverse will be true, and that will give me a reason to leave.”
Dr. Young encourages the patient to overcome his desire to escape and stay at the dance despite his anxiety:
THERAPIST: Now imagine that you’re at the dance and you actually see a woman you’re attracted to. Now be the schema side.
DANIEL: (as the schema side) “She looks like a really nice person, but I don’t think she’d go for me. I’m probably not even up to this person, on either an intellectual level or an emotional level. She’s probably way ahead of me maturity-wise. And she’ll probably go for one of these other guys, and they’ll probably ask her before me anyway.”
THERAPIST: All right, now be the healthy side that we’re trying to build up and have it answer. Talk back to that side.
DANIEL: (as the healthy side) “Don’t be so quick to judge. You have a lot of good parts to yourself that probably would be very appealing to this woman. You have a definite value system, you know boundaries, you can allow her to be her own person, you have a definite sensitivity towards female issues, and she probably would like you a lot.”
Here Daniel is using his prior cognitive work against the schema. Dr. Young elicits more of the schema side:
THERAPIST: Now go back to the schema side.
DANIEL: (as the schema side) “But even so, when it comes down to continuing the conversation to the point of asking her for a date, you know, I don’t think you should, because then you’re going to have to deal with other issues, such as, maybe becoming more intimate and figuring out where to go after the date, whether you should go to bed or whether you shouldn’t go to bed. It’s better that you don’t get involved because of that.”
THERAPIST: Now be the healthy side again.
DANIEL: (as the healthy side) “I don’t think that’s the issue right now, and you wouldn’t have to be worried about it for a long time.”
THERAPIST: Try to answer it, though. Try to answer it even though you’re right, you don’t have to worry about it till later, but try to at least give some hope that there’s an answer to it.
The therapist encourages Daniel to answer every argument posed by the schema.
DANIEL: (as the healthy side) “I think that, when it gets to that point, that I could do very well giving affection and being emotionally supportive and being sensitive when it comes time to being sexually intimate, possibly. (Speaks hesitantly.) I don’t think that’ll be a problem.”
THERAPIST: (coaching the patient as the healthy side) “I have to be sure I trust the woman before I try to do anything sexual.”
The therapist helps Daniel when he falters. Sexual intimacy is an issue he is only beginning to explore in his relationships with women.
DANIEL: (continuing as the healthy side) “I would have to trust. I would just have to learn how to trust the woman and feel safe.”
THERAPIST: Now be the schema side that says, “You’ll never do that, women can’t be trusted.”
The therapist tries to elicit all the counterarguments the schema utilizes to preserve itself.
DANIEL: (as the schema side) “Women can’t be trusted, and they’re very unreasonable and erratic, and it will be very difficult to figure out just what to do. And I don’t think you can do it.”
THERAPIST: OK, now be the other side.
DANIEL: (as the healthy side) “Women are people just like men are, and they can be very reasonable, and they’re very nice to be with.”
The therapist tries to help the patient differentiate his mother, who was the primary cause of his schemas, from other women.
THERAPIST: Try to distinguish your mother from other women in your answer.
DANIEL: (continuing as the healthy side) “And all woman aren’t necessarily like your mother. Each woman is a unique person just like I am, and they have to be treated as individuals. And there are many women who have value systems that are probably even better than mine.”
THERAPIST: Now be the schema side.
DANIEL: (as the schema side) “Well, that’s easier said than done, because your mother really fixed it so no woman could possibly be good to you. The women here are just like all women. Women in general are like your mother, and they’re just concerned about one thing, using you and abusing you. And that’s just about what you’re gonna wind up with. Eventually you’ll be used or abused.”
THERAPIST: Now be the healthy side.
DANIEL: (as the healthy side) “Again, all women are not like my mother, and all women are not abusive. Women are neither totally bad nor totally good. They’re like every other person; they have good parts and bad parts.”
The patient goes back and forth between the chairs. The therapist continues the exercise until the healthy side has the final word.
It takes most patients a long time and a lot of practice before they can play the healthy side with assurance. It takes many months of repeating the exercise to “chip away” at the schema and fortify the healthy side. The therapist asks patients to repeat the dialogues until they can play the healthy side independently. Even though they can speak the words, however, patients still say, “I don’t really believe the healthy side.” The therapist can answer: “Most patients feel the way you do at this point in the therapy: Rationally they understand the healthy side, but emotionally they don’t believe it yet. All I’m asking you to do now is to say what you know to be logically true. Later we’ll work on helping you take in what you’re saying on a more emotional level.”
After completing the schema restructuring process, the therapist and patient begin to write schema flash cards. Schema flash cards summarize healthy responses to specific schema triggers. Patients carry the flash cards around with them and read them when the relevant schemas are triggered. Ideally, flash cards contain the most powerful evidence and arguments against the schema and provide patients with continual rehearsals of rational responses.
We provide a Schema Therapy Flash Card template (see Figure 3.1) for the therapist to use as a guide (Young, Wattenmaker, & Wattenmaker, 1996). Using the template, the therapist collaborates with the patient in composing flash cards. The therapist plays such an active role because, at this point in therapy, the patient’s healthy side is not strong enough to write a truly convincing answer to the schema. Usually the therapist dictates the flash card while the patient writes it down on an index card.
In the following excerpt, Dr. Young and Daniel create a flash card for him to read in social situations with women in which he feels anxious.
THERAPIST: There are various techniques we can use to try to help you overcome situations you tend to avoid. One is flash cards. A flash card is a card you carry around with you that basically answers a lot of the fears you have and the schemas that come up. In fact, if you want, I could dictate one to you and you could jot it down. How would that be?
DANIEL: That would be wonderful.
THERAPIST: Maybe we’ll pick one based on what we’ve already talked about in here, as if you’re at one of these dances and you’re trying to meet a woman. How would that be?
DANIEL: That sounds good.
THERAPIST: I’ll dictate and you can just jot it down. You can revise it if it doesn’t seem to fit.
THERAPIST: (dictating) “Right now I’m feeling nervous about approaching a woman because I’m worried she won’t find me desirable.” Is “desirable” the right word? Is there a better word?
DANIEL: “Attractive.”
THERAPIST: “Attractive”? OK. And also, I’m trying to get at the deeper part of that, like “I won’t be able to love her enough,” or “I won’t be able to show love to her.”
DANIEL: “Able to be loving.”
THERAPIST: “Able to be loving.” That’s good. “I also am worried that I can’t trust her to be…”?
DANIEL: “Honest and trustworthy.”
Dr. Young tries to use the patient’s own words while constructing the flash card.
THERAPIST: OK. “However, I know that these are my Defectiveness and Mistrust/Abuse schemas being triggered. These are based on my feelings about my mother and have nothing to do with my value or this woman’s trustworthiness. The reality is.…” Now we want to fill in some evidence that you have to the contrary, that you are lovable and desirable and attractive to women in different ways.
DANIEL: “The reality is I am a very affectionate person capable of being warm and loving.”
THERAPIST: Maybe we’ll put in parentheses a person you’ve shown that to.
DANIEL: “I can be an affectionate person with my son.”
THERAPIST: And now, “Furthermore…” Now I want to say something about the woman you are with. That objectively, women are no less trustworthy than men.
DANIEL: “Women can be very reasonable and trustworthy, just as men can be.”
THERAPIST: Good. Now, the end of the card would say something like, “Therefore, I must approach this woman, even though I feel nervous, because it’s the only way to get my emotional needs met.” How’s that seem to you?
DANIEL: It seems very good.
The complete flash card reads as follows:
Right now I’m feeling nervous about approaching a woman because I’m worried that she won’t find me attractive and that I won’t be able to be loving. I also am worried that I can’t trust her to be honest and trustworthy.
However, I know that these are my Defectiveness and Mistrust/Abuse schemas being triggered. These are based on my feelings about my mother and have nothing to do with my value or this woman’s trustworthiness. The reality is that I am a very affectionate person capable of being warm and loving. (For example, I’m an affectionate person with my son.) Furthermore, women can be very reasonable and trustworthy, just as men can be.
Therefore, I must approach this woman, even though I feel nervous, because it’s the only way to get my emotional needs met.
Daniel can take the flash card with him when he goes to social events and read it when he feels anxious. We expect that reading the flash card before going into the situation will help him shift into a more positive point of view, and reading the card during the event when he feels disheartened will help him interact with women in more positive ways. By repeatedly reading the flash card, Daniel can act to weaken his Defectiveness and Mistrust/Abuse schemas and strengthen his healthy side.
Some patients with BPD carry large numbers of flash cards, one for each of many schema triggers. In addition to helping these patients manage affect and behave in healthier ways, the flash cards serve as transitional objects. Patients with BPD often report that carrying flash cards feels as if they are carrying the therapist along with them. The presence of the flash card is comforting.
FIGURE 3.1 Schema Therapy Flash Card.
Copyright 1996, 2002 by Jeffrey Young, PhD, Diane Wattenmaker, RN, and Richard Wattenmaker, PhD. Unauthorized reproduction without written consent of the authors is prohibited. For permission, write to Schema Therapy Institute, 36 West 44th Street, Suite 1007, New York, NY 10036.
The Schema Diary (Young, 1993) is a more advanced technique than the flash card. With the flash card, the therapist and patient construct a healthy response ahead of time for a specific schema trigger, and the patient reads the flash card as needed before and during the event. With the Schema Diary, patients construct their own healthy responses as their schemas are triggered in the course of their daily lives. The therapist therefore introduces the Schema Diary later in treatment, after the patient has become proficient at using flash cards.
The therapist instructs patients to carry copies of the Schema Diary form with them as they go about their lives. When a schema is triggered, patients fill out the form in order to work through the problem and arrive at a healthy solution. The Schema Diary asks the patient to identify trigger events, emotions, thoughts, behaviors, schemas, healthy views, realistic concerns, overreactions, and healthy behaviors.
We provide a case example. Emily is 26 years old. She recently began a job as the project director of a grant for an arts foundation. Her Subjugation schema has made it difficult for her to manage her staff effectively. She has had the greatest difficulty with a domineering and condescending subordinate named Jane. By the time Emily entered therapy, she was allowing her staff to make most of her administrative decisions. When Jane behaved in an angry way toward her, Emily apologized. “It’s like she’s my boss instead of my being her boss,” Emily says.
With schema therapy, Emily identifies her Subjugation schema and explores the origins of her schema in childhood. She observes how her schema stops her from asserting herself, especially with Jane. Emily filled out a Schema Diary form at work (see Figure 3.2), moments after Jane requested a meeting with her later in the day.
FIGURE 3.2. Emily’s Schema Diary.
Trigger: Jane said she wants to meet with me at three o’clock this afternoon.
Emotions: I feel scared and want to hide.
Thoughts: She’ll tell me off and I won’t know what to do. I can’t stand up to her.
Actual Behaviors: I agreed to meet with her. I’m filling out this form so I can figure out what to do.
Schemas: I remember having to be available to my father and my first husband and how I had to be careful not to upset them. When they got angry, look out. Even now, I let my second husband tell me what to do, and he’s nice. My Subjugation schema makes me want to give Jane whatever she wants so she won’t get mad at me.
Healthy View: I don’t know what Jane wants to meet about. Anyway, I don’t have to give her whatever she wants. I deserve respect and can end the meeting if she turns abusive.
Realistic Concerns: Jane is very intimidating with people. She could yell at me. I’m not perfect at this job, but I’m getting better. I know she can find something I did wrong if she really wants to.
Overreactions: I jumped to two conclusions. The first one is that Jane wants to berate me and the second one is that there’s nothing I can do about it. That makes me feel passive and helpless, like the best I can do is just survive the meeting. This attitude paralyzes me.
Healthy Behavior: I can meet with Jane and find out what she wants instead of stewing about this. If she’s rude, I can end the meeting. On the other hand, I might not be attacked, so I won’t prepare to attack back. The bottom line is I have time to prepare and I can find a solution that works for me.