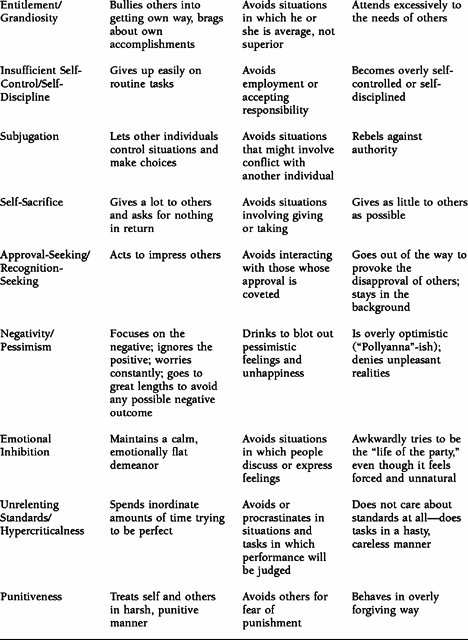
TABLE 1.1. Examples of Maladaptive Coping Responses
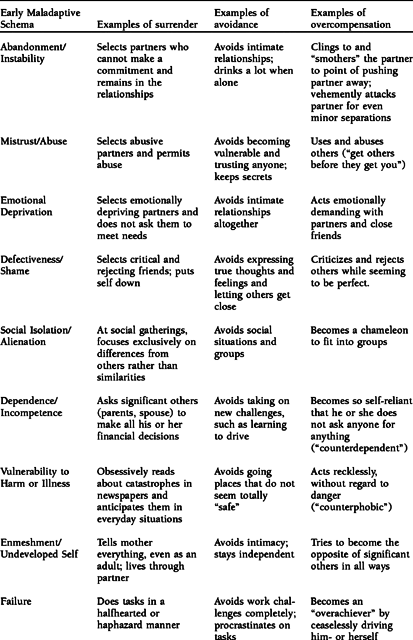
The concept of a schema mode is probably the most difficult part of schema theory to explain, because it encompasses many elements. Schema modes are the moment-to-moment emotional states and coping responses—adaptive and maladaptive—that we all experience. Often our schema modes are triggered by life situations to which we are oversensitive (our “emotional buttons”). Unlike most other schema constructs, we are actively interested in working with both adaptive and maladaptive modes. In fact, we try to help patients flip from a dysfunctional mode to a healthy mode as part of the schema healing process.
At any given point in time, some of our schemas or schema operations (including our coping responses) are inactive, or dormant, while others have become activated by life events and predominate in our current moods and behavior. The predominant state that we are in at a given point in time is called our “schema mode.” We use the term “flip” to refer to the switching of modes. As we have said, this state may be adaptive or maladaptive. All of us flip from mode to mode over time. A mode, therefore, answers the question, “At this moment in time, what set of schemas or schema operations is the patient manifesting?”
Our revised definition of a schema mode is: “those schemas or schema operations—adaptive or maladaptive—that are currently active for an individual.” A dysfunctional schema mode is activated when specific maladaptive schemas or coping responses have erupted into distressing emotions, avoidance responses, or self-defeating behaviors that take over and control an individual’s functioning. An individual may shift from one dysfunctional schema mode into another; as that shift occurs, different schemas or coping responses, previously dormant, become active.
TABLE 1.1. Examples of Maladaptive Coping Responses
Viewed in a different way, a dysfunctional schema mode is a facet of the self involving specific schemas or schema operations that has not been fully integrated with other facets. According to this perspective, schema modes can be characterized by the degree to which a particular schema-driven state has become dissociated, or cut off, from an individual’s other modes. A dysfunctional schema mode, therefore, is a part of the self that is cut off to some degree from other aspects of the self.
A dysfunctional schema mode can be described in terms of the point on a spectrum of dissociation at which this particular mode lies. To the degree that an individual is simultaneously able to experience or blend more than one mode, the level of dissociation is lower. We typically refer to this mild form of a schema mode as a normal mood shift, such as a lonely mood or an angry mood. At the highest level of dissociation is a patient with dissociative identity disorder (or multiple personality disorder). In these instances, a patient in one mode may not even know that another mode exists; and, in extreme cases, a patient with dissociative identity disorder (DID) may even have a different name for each mode. We discuss this concept of modes as dissociative states in more depth later.
We have currently identified 10 schema modes, although more modes will undoubtedly be identified in the future. The modes are grouped into four general categories: Child modes, Dysfunctional Coping modes, Dysfunctional Parent modes, and the Healthy Adult mode. Some modes are healthy for an individual, whereas others are maladaptive. We elaborate further on these 10 modes in a subsequent section.
One important goal of schema therapy is to teach patients how to strengthen their Healthy Adult modes, so that they can learn to navigate, negotiate with, nurture, or neutralize dysfunctional modes.
The concept of schema modes originated from our work with patients with borderline personality disorder (BPD), although now we apply it to many other diagnostic categories as well. One of the problems we were having applying the schema model to patients with BPD was that the number of schemas and coping responses they had was overwhelming for both the patient and the therapist to deal with all at one time. For example, we find that, when we give patients with BPD the Young Schema Questionnaire, it is not unusual for them to score high on almost all of the 16 schemas assessed. We found that we needed a different unit of analysis, one that would group schemas together and make them more manageable.
Patients with BPD were also problematic for the original schema model because they continually shift from one extreme affective state or coping response to another: One moment they are angry; the next they may be sad, detached, avoidant, robotic, terrified, impulsive, or filled with self-hatred. Our original model, because it focused primarily on trait constructs—a schema or a coping style—did not seem sufficient to account for the phenomenon of shifting states.
Let us elaborate further on this state-trait distinction as it relates to schema theory. When we say that an individual has a schema, we are not saying that at every moment the schema is activated. Rather, the schema is a trait that may or may not be activated at a given moment. Similarly, individuals have characteristic coping styles, which they may or may not be utilizing at a given moment. Thus our original trait model tells us about the functioning of the patient over time, but it does not tell us about the patient’s current state. Because patients with BPD are so labile, we decided to move away from a trait model and toward a state model in treating them, with the schema mode as the primary conceptual construct.
When we look carefully at individual patients, we observe that their schemas and coping responses tend to group together into parts of the self. Certain clusters of schemas or coping responses are triggered together. For example, in the Vulnerable Child mode, the affect is that of a helpless child—fragile, frightened, and sad. When a patient is in this mode, schemas of Emotional Deprivation, Abandonment, and Vulnerability may be simultaneously activated. The Angry Child mode often presents with the affect of an enraged child having a temper tantrum. The Detached Protector mode is characterized by the absence of emotion, combined with high levels of avoidance. Thus some of the modes are composed primarily of schemas, whereas others primarily represent coping responses.
Each individual patient exhibits certain characteristic schema modes, by which we mean characteristic groupings of schemas or coping responses. Similarly, some Axis II diagnoses can be described in terms of their typical modes. For example, the patient with BPD usually exhibits four schema modes and shifts rapidly from one to the other. One moment the patient is in the Abandoned Child mode, experiencing the pain of her schemas; the next moment she may flip into the Angry Child mode, expressing rage; she may then shift into the Punitive Parent mode, punishing the Abandoned Child; and finally she may retreat into the Detached Protector, blocking her emotions and detaching from people to protect herself.
We mentioned briefly that our concept of a schema mode relates to a spectrum of dissociation. Although we realize that the diagnosis has become controversial, we view the different personalities of patients with DID as extreme forms of dysfunctional modes. Different parts of the self have split off into separate personalities that are often unaware of each other and that may have different names, ages, genders, personality traits, memories, and functions. The dissociative identities of these patients usually consist of either a child at a specific age who has experienced severe trauma; an internalized parent tormenting, criticizing, or persecuting the child; or an adult-like coping mode that in some way protects or blocks out the child modes. We believe that the dissociative identities in DID differ from the modes of patients with BPD mainly in degree and number. Both multiple personalities and borderline modes are parts of the self that have been split off, but the borderline modes have not been split off to nearly the same degree. Furthermore, patients with DID usually have more modes than patients with BPD because they frequently have more than one mode of each type (e.g., three Vulnerable Child modes, each a different age).
A psychologically healthy individual still has recognizable modes, but the sense of a unified identify remains intact. A healthy individual might shift into a detached, angry, or sad mood in response to changing circumstances, but these modes will differ from borderline modes in several important respects. First, as we have said, normal modes are less dissociated than borderline modes. Healthy individuals can experience more than one mode simultaneously. For example, they can be both sad and happy about an event, thus producing the sensation of “bittersweet.” In contrast, when we talk about a borderline mode, we are referring to one part of the self that is split off from the other parts in a pure and intense form. The individual is overwhelmingly frightened or completely enraged. Second, normal modes are less rigid and more flexible and open to change than the modes of patients with serious characterological problems. In Piagetian terms, they are more open to accommodation in response to reality (Piaget, 1962).
To summarize, modes vary from one individual to another along several dimensions:
Dissociated ↔ Integrated
Unacknowledged ↔ Acknowledged
Maladaptive ↔ Adaptive
Extreme ↔ Mild
Rigid ↔ Flexible
Pure ↔ Blended
Another difference between healthy and more impaired individuals lies in the strength and effectiveness of the Healthy Adult mode. Although we all have a Healthy Adult mode, the mode is stronger and more frequently activated in psychologically healthy people. The Healthy Adult mode can moderate and heal dysfunctional modes. For example, when psychologically healthy people become angry, they have a Healthy Adult mode that can usually keep angry emotions and behaviors from going out of control. In contrast, patients with BPD typically have a very weak Healthy Adult mode, so that when the Angry Child mode is triggered, there is no strong counterbalancing force. The anger almost completely takes over the patient’s personality.
We have identified 10 schema modes that can be grouped into four broad categories: Child modes, Dysfunctional Coping modes, Dysfunctional Parent modes, and the Healthy Adult mode.
We believe that the Child modes are innate and universal. All children are born with the potential to manifest them. We have identified four: the Vulnerable Child, the Angry Child, the Impulsive/Undisciplined Child, and the Happy Child modes. (These labels are general terms. In actual therapy we individualize the names of modes collaboratively with patients. For example, we might refer to the Vulnerable Child mode as Little Ann, or Abandoned Carol.)
The Vulnerable Child is the mode that usually experiences most of the core schemas: It is the Abandoned Child, the Abused Child, the Deprived Child, or the Rejected Child. The Angry Child is the part that is enraged about unmet emotional needs and that acts in anger without regard to consequences. The Impulsive/Undisciplined Child expresses emotions, acts on desires, and follows natural inclinations from moment to moment in a reckless manner, without regard to possible consequences for the self or others. The Happy Child is one whose core emotional needs are currently met.
We have identified three dysfunctional coping modes: the Compliant Surrenderer, the Detached Protector, and the Overcompensator. These three modes correspond to the three coping styles of surrender, avoidance, and overcompensation. (Again, we tailor the name of the mode so that it fits the feelings and behaviors of the individual patient.) The Compliant Surrenderer submits to the schema, becoming once again the passive, helpless child who must give in to others. The Detached Protector withdraws psychologically from the pain of the schema by emotionally detaching, abusing substances, self-stimulating, avoiding people, or utilizing other forms of escape. The Overcompensator fights back either by mistreating others or by behaving in extreme ways in an attempt to disprove the schema in a manner that ultimately proves dysfunctional (see the previous discussion of overcompensation for examples). All three maladaptive coping modes ultimately perpetuate schemas.
We have identified two dysfunctional parent modes thus far: the Punitive Parent and the Demanding Parent. In these modes, the patient becomes like the parent who has been internalized. The Punitive Parent punishes one of the child modes for being “bad,” and the Demanding Parent continually pushes and pressures the child to meet excessively high standards.
The 10th mode, as described earlier, is the Healthy Adult. This is the mode we try to strengthen in therapy by teaching the patient to moderate, nurture, or heal the other modes.