CHAPTER 12
Training 101
How to Prepare for the Centenarian Decathlon
It is impossible to produce superior performance unless you do something different from the majority.
—Sir John Templeton
Most treatments of exercise are either very specific (e.g., how to train for your first marathon) or overly vague (e.g., “Just keep moving!”). Or they emphasize “cardio” over “weights,” or vice versa. In this chapter, we are seeking to optimize our exercise regimen around the principle of longevity. What combination of modalities will help us delay the onset of chronic disease and death, while simultaneously maintaining healthspan for as long as possible?
This question turns out to be more complicated than how to lower your risk of cardiovascular disease, because there are more variables, and more choices within each variable. It is not a one-dimensional problem but more of a three-dimensional one. The three dimensions in which we want to optimize our fitness are aerobic endurance and efficiency (aka cardio), strength, and stability. All three of these are key to maintaining your health and strength as you age. (And as we’ve seen, they also extend lifespan.) But both cardio and strength are far more nuanced than most people realize—and stability may be the least understood component of all.
When we say “cardio,” we are talking about not one thing, but a physiologic continuum, ranging from an easy walk to an all-out sprint. The various levels of intensity all count as cardio but are fueled by multiple different energy systems. For our purposes, we are interested in two particular regions of this continuum: long, steady endurance work, such as jogging or cycling or swimming, where we are training in what physiologists call zone 2, and maximal aerobic efforts, where VO2 max comes into play.
The strength side of the equation seems simpler, at first: if you use your muscles to counter some resistance, in the form of weights or other forces (e.g., gravity, or elastic bands), they will adapt and grow stronger. That’s how muscle works, and it’s really quite wonderful. There are a few specific movements that I consider to be foundational, but here our most important goal is not only to build strength and muscle mass. It’s equally important that we avoid injury in the process.
This is where stability comes in. We will talk about it in much more detail in the next chapter, but I consider stability to be just as important as aerobic fitness and strength. It’s a bit hard to define, but I think of stability as the solid foundation that enables us to do everything else that we do, without getting injured. Stability makes us bulletproof. Sophie was relatively fit for her age, but she likely lacked stability, making her vulnerable to injury. Many people are in the same boat without even realizing it—even me, in my twenties. It almost doesn’t matter how fit you are; you can still be at risk. This is why our approach to exercise must increase not only our conventional measures of fitness, such as our VO2 max and our muscular strength, but above all our resistance to injury.
In the sections to follow, we will be building a framework around each of these, to help you craft your training program for your own Centenarian Decathlon.
Aerobic Efficiency: Zone 2
Notice that one word has been missing in our discussion of exercise thus far: calories. Most people think that one of the primary benefits of exercise, if not the primary benefit, is that it “burns calories.” And it does, but we are more interested in a finer distinction—not calories, but fuels. How we utilize different fuels, glucose and fatty acids, is critical not only to our fitness but also to our metabolic and overall health. Aerobic exercise, done in a very specific way, improves our ability to utilize glucose and especially fat as fuel.
The key here are the mitochondria, those tiny little intracellular organelles that produce much of our energy. These cellular “engines” can burn both glucose and fat, and thus they are fundamental to our metabolic health. Healthy mitochondria are also important to maintaining the health of our brain, and to controlling potential bad actors like oxidative stress and inflammation. I am convinced that it is impossible to be healthy without also having healthy mitochondria, which is why I place a great deal of emphasis on long, steady endurance training in zone 2.
Zone 2 is one of five levels of intensity used by coaches and trainers in endurance sports to structure their athletes’ training programs. It can get confusing, because some coaches define training zones in terms of heart rate, while others focus on different levels of power output; adding to the confusion, some models have five zones, but others have six or seven. Typically, zone 1 is a walk in the park and zone 5 (or 6, or 7) is an all-out sprint. Zone 2 is more or less the same in all training models: going at a speed slow enough that one can still maintain a conversation but fast enough that the conversation might be a little strained. It translates to aerobic activity at a pace somewhere between easy and moderate.
I had done plenty of zone 2 workouts in my cycling days; this type of training is foundational for any endurance sport. But I had never fully grasped the importance of zone 2 training to our overall health until I happened to meet a very bright exercise scientist named Iñigo San Millán in 2018. I had flown to the United Arab Emirates for a meeting, and shortly after landing, at 11 p.m. on a cool December evening, I was introduced to San Millán, an assistant professor at the University of Colorado School of Medicine who had recently been hired as director of performance for the UAE Team Emirates professional cycling team. He was there to do preseason testing of some of the UAE team riders, and when he found out I was a former cyclist, he put me on a stationary bike right then and there, in the middle of the night, to do a VO2 max test. My kind of guy.
A native of Spain and a former professional cyclist himself, San Millán has worked with all kinds of athletes and coaches in many sports, including hundreds of top professional cyclists. He is also the personal coach of 2020 and 2021 Tour de France champion (and 2022 runner-up) Tadej Pogačar. Despite his impressive sports résumé, San Millán’s true passion is studying the relationship between exercise, mitochondrial health, and diseases such as cancer and type 2 diabetes. As he explained, he hopes to use his insights into the fittest people on the planet, professional cyclists and other elite endurance athletes, in order to help the very least fit people—the one-third to one-half of the population with metabolic diseases or derangements.
In San Millán’s view, healthy mitochondria are key to both athletic performance and metabolic health. Our mitochondria can convert both glucose and fatty acids to energy—but while glucose can be metabolized in multiple different ways, fatty acids can be converted to energy only in the mitochondria. Typically, someone working at a lower relative intensity will be burning more fat, while at higher intensities they would rely more on glucose. The healthier and more efficient your mitochondria, the greater your ability to utilize fat, which is by far the body’s most efficient and abundant fuel source. This ability to use both fuels, fat and glucose, is called “metabolic flexibility,” and it is what we want: in chapters 6 and 7, we saw how the relentless accumulation and spillover of fat drives conditions such as diabetes and cardiovascular disease. Healthy mitochondria (fostered by zone 2 training) help us keep this fat accumulation in check.
A few years ago, San Millán and his colleague George Brooks published a fascinating study that helps illustrate this point. They compared three groups of subjects: professional cyclists, moderately active healthy males, and sedentary men who met the criteria for the metabolic syndrome, meaning essentially that they were insulin resistant. They had each group ride a stationary bicycle at a given level of intensity relative to their fitness (about 80 percent of their maximum heart rate), while the scientists analyzed the amount of oxygen they consumed and the CO2 they exhaled in order to determine how efficiently they produced power—and what primary fuels they were using. The differences they found were striking. The professional cyclists could zoom along, producing a huge amount of power while still burning primarily fat. But the subjects with metabolic syndrome relied almost entirely on glucose for their fuel source, even from the first pedal stroke. They had virtually zero ability to tap into their fat stores, meaning they were metabolically inflexible: able to use only glucose but not fat.
Obviously, these two groups—professional athletes and sedentary, unhealthy people—were as dissimilar as could be. San Millán’s insight was that the sedentary subjects needed to be training in a manner similar to the Tour de France–bound cyclists he worked with. A professional cyclist might spend thirty to thirty-five hours a week training on his or her bike, and 80 percent of that time in zone 2. For an athlete, this builds a foundation for all their other, more intense training. (The catch is that a professional rider’s zone 2 output feels like zone 5 for most people.)
As fundamental as zone 2 training is for professional cyclists, however, San Millán believes that it’s even more important for nonathletes, for two reasons. First, it builds a base of endurance for anything else you do in life, whether that is riding your bike in a one-hundred-mile century ride or playing with your kids or grandkids. The other reason is that he believes it plays a crucial role in preventing chronic disease by improving the health and efficiency of your mitochondria, which is why training aerobic endurance and efficiency (i.e., zone 2 work) is the first element of my Centenarian Decathlon training program.
When we are exercising in zone 2, most of the work is being done by our type 1, or “slow-twitch,” muscle fibers. These are extremely dense with mitochondria and thus well-suited for slow-paced, efficient endurance work. We can go for a long time without feeling fatigued. If we pick up the pace, we begin to recruit more type 2 (“fast-twitch”) muscle fibers, which are less efficient but more forceful. They also generate more lactate in the process, because of the way they create ATP. Lactate itself is not bad; trained athletes are able to recycle it as a type of fuel. The problem is that lactate becomes lactic acid when paired with hydrogen ions, which is what causes that acute burning you feel in your muscles[*1] during a hard effort.
In technical terms, San Millán describes zone 2 as the maximum level of effort that we can maintain without accumulating lactate. We still produce it, but we’re able to match production with clearance. The more efficient our mitochondrial “engine,” the more rapidly we can clear lactate, and the greater effort we can sustain while remaining in zone 2. If we are “feeling the burn” in this type of workout, then we are likely going too hard, creating more lactate than we can eliminate.
Because I am a numbers guy and I love biomarkers and feedback, I often test my own lactate while I am working out this way, using a small handheld lactate monitor, to make sure my pacing is correct. The goal is to keep lactate levels constant, ideally between 1.7 and 2.0 millimoles. This is the zone 2 threshold for most people. If I’m working too hard, lactate levels will rise, so I’ll slow down. (It’s sometimes tempting to go too hard in zone 2, because the workout feels relatively “easy” on good days.) I make a point of this because lactate is literally what defines zone 2. It’s all about keeping lactate levels steady in this range, and the effort sustainable.
If you don’t happen to have a portable lactate meter on hand, like most people, there are other ways to estimate your zone 2 range that are reasonably accurate. If you know your maximum heart rate—not estimated, but your actual maximum, the highest number you’ve ever seen on a heart rate monitor—your zone 2 will correspond to between approximately 70 and 85 percent of that peak number, depending on your fitness levels. That’s a big range, so when starting people out, I prefer they rely on their rate of perceived exertion, or RPE, also known as the “talk test.” How hard are you working? How easy is it to speak? If you’re at the top of zone 2, you should be able to talk but not particularly interested in holding a conversation. If you can’t speak in complete sentences at all, you’re likely into zone 3, which means you’re going too hard, but if you can comfortably converse, you’re likely in zone 1, which is too easy.
Zone 2 output is highly variable, depending on one’s fitness. In San Millán and Brooks’s study, the professional cyclists produced about three hundred watts of power in zone 2, while the sedentary, metabolically unhealthy subjects could generate only about one hundred watts at the same relative level of intensity. That’s a huge difference. If we express this output in terms of watts per kilogram of body weight, the difference becomes even more stark: The seventy-kilogram cyclists put out more than four watts per kilogram of body weight, while the one-hundred-plus kilogram sedentary subjects could only manage about one watt per kilogram.
This pronounced difference comes back to the fact that the unhealthy subjects’ mitochondria—their engine(s)—were much less efficient than those of the athletes, so they very quickly switched over from aerobic respiration, burning fat and glucose in the mitochondria with oxygen, to the much less efficient glycolysis, an energy-producing pathway that consumes only glucose and produces loads of lactate (similar to the way cancer cells produce energy, via the Warburg effect). Once we start producing energy this way, lactate accumulates and our effort quickly becomes unsustainable. There are other (fortunately rare) genetic diseases that target the mitochondria and produce far more severe sequelae, but in terms of mass-acquired chronic conditions, type 2 diabetes does a real number on the mitochondria, and San Millán’s data very elegantly demonstrate the disability that it creates.
Even when we are at rest, our lactate levels tell us much about our metabolic health. People with obesity or other metabolic problems will tend to have much higher resting lactate levels, a clear sign that their mitochondria are not functioning optimally, because they are already working too hard just to maintain baseline energy levels. This means that they are relying almost totally on glucose (or glycogen) for all their energy needs—and that they are totally unable to access their fat stores. It seems unjust, but the people who most need to burn their fat, the people with the most of it, are unable to unlock virtually any of that fat to use as energy, while the lean, well-trained professional athletes are able to do so easily because they possess greater metabolic flexibility (and healthier mitochondria).[*2]
Mitochondrial health becomes especially important as we grow older, because one of the most significant hallmarks of aging is a decline in the number and quality of our mitochondria. But the decline is not necessarily a one-way street. Mitochondria are incredibly plastic, and when we do aerobic exercise, it stimulates the creation of many new and more efficient mitochondria through a process called mitochondrial biogenesis, while eliminating ones that have become dysfunctional via a recycling process called mitophagy (which is like autophagy, touched on in chapter 5, but for mitochondria). A person who exercises frequently in zone 2 is improving their mitochondria with every run, swim, or bike ride. But if you don’t use them, you lose them.
This is another reason why zone 2 is such a powerful mediator of metabolic health and glucose homeostasis. Muscle is the largest glycogen storage sink in the body, and as we create more mitochondria, we greatly increase our capacity for disposing of that stored fuel, rather than having it end up as fat or remaining in our plasma. Chronic blood glucose elevations damage organs from our heart to our brain to our kidneys and nearly everything in between—even contributing to erectile dysfunction in men. Studies have found that while we are exercising, our overall glucose uptake increases as much as one-hundred-fold compared to when we are at rest. What’s interesting is that this glucose uptake occurs via multiple pathways. There is the usual, insulin-signaled way that we’re familiar with, but exercise also activates other pathways, including one called non-insulin-mediated glucose uptake, or NIMGU, where glucose is transported directly across the cell membrane without insulin being involved at all.
This in turn explains why exercise, especially in zone 2, can be so effective in managing both type 1 and type 2 diabetes: It enables the body to essentially bypass insulin resistance in the muscles to draw down blood glucose levels. I have one patient with type 1 diabetes, meaning he produces zero insulin, who keeps his glucose in check almost entirely by walking briskly for six to ten miles every day, and sometimes more. As he walks, his muscle cells are vacuuming glucose out of his bloodstream via NIMGU. He still needs to inject himself with insulin, but only a tiny fraction of the amount that he would otherwise require.
One other plus of zone 2 is that it is very easy to do, even for someone who has been sedentary. For some people, a brisk walk might get them into zone 2; for those in better condition, zone 2 means walking uphill. There are many different ways to do it: you can ride a stationary bicycle at the gym, or walk or jog or run around the track at the local high school, or swim some laps in the pool. The key is to find an activity that fits into your lifestyle, that you enjoy doing, and that enables you to work at a steady pace that meets the zone 2 test: You’re able to talk in full sentences, but just barely.
How much zone 2 training you need depends on who you are. Someone who is just being introduced to this type of training will derive enormous benefit from even two 30-minute sessions per week to start with. Based on multiple discussions with San Millán and other exercise physiologists, it seems that about three hours per week of zone 2, or four 45-minute sessions, is the minimum required for most people to derive a benefit and make improvements, once you get over the initial hump of trying it for the first time. (People who are training for major endurance events, such as running a marathon, obviously need to do more than this.) I am so persuaded of the benefits of zone 2 that it has become a cornerstone of my training plan. Four times a week, I will spend about an hour riding my stationary bike at my zone 2 threshold.
One way to track your progression in zone 2 is to measure your output in watts at this level of intensity. (Many stationary bikes can measure your wattage as you ride.) You take your average wattage output for a zone 2 session and divide it by your weight to get your watts per kilogram, which is the number we care about. So if you weigh 60 kilos (about 132 pounds) and can generate 125 watts in zone 2, that works out to a bit more than 2 watts/kg, which is about what one would expect from a reasonably fit person. These are rough benchmarks, but someone who is very fit will be able to produce 3 watts/kg, while professional cyclists put out 4 watts/kg and up. It’s not the number that matters, but how much you are improving over time. (If you’re a runner or a walker, the same principle applies: As you improve, your zone 2 pace will get faster.)
Zone 2 can be a bit boring on its own, so I typically use the time to listen to podcasts or audiobooks, or just think about issues that I’m working on—a side benefit of zone 2 is that it also helps with cognition, by increasing cerebral blood flow and by stimulating the production of BDNF, brain-derived neurotrophic factor, which we touched on earlier. This is another reason why zone 2 is such an important part of our Alzheimer’s disease prevention program.
I think of zone 2 as akin to building a foundation for a house. Most people will never see it, but it is nevertheless important work that helps support virtually everything else we do, in our exercise regimen and in our lives.
Maximum Aerobic Output: VO2 Max
If zone 2 represents a steady state, where you are kind of cruising along at a sustainable pace, VO2 max efforts are almost the opposite. This is a much higher level of intensity—a hard, minutes-long effort, but still well short of an all-out sprint. At VO2 max, we are using a combination of aerobic and anaerobic pathways to produce energy, but we are at our maximum rate of oxygen consumption. Oxygen consumption is the key.
Besides improving mitochondrial health and glucose uptake and metabolic flexibility, and all those other good things, zone 2 training also increases your VO2 max somewhat. But if you really want to raise your VO2 max, you need to train this zone more specifically. Typically, for patients who are new to exercising, we introduce VO2 max training after about five or six months of steady zone 2 work.
One reason why I emphasize this so much is that this measure of peak aerobic capacity is powerfully correlated with longevity, as we saw in chapter 11. I have all my patients undergo VO2 max testing and then train to improve their score. Even if you are not competing in high-level endurance sports, your VO2 max is an important number that you can and should know.
Testing is widely available, even from some of the larger fitness chains. The bad news is that the VO2 max test is an unpleasant affair that entails riding an exercise bike or running on a treadmill at ever greater intensity, while wearing a mask designed to measure oxygen consumption and CO2 production. The peak amount of oxygen you consume, typically close to the point at which you “fail,” meaning the point where you just can’t keep going, yields your VO2 max. We have all our patients do the test at least annually, and they almost all hate it. We then compare their results, normalized by weight, to the population of their age and sex.
Why is this important? Because our VO2 max is a pretty good proxy measure of our physical capability. It tells us what we can do—and what we cannot do. Take a look at figure 11, which charts low, average, and high VO2 max levels by age. Two things stand out. First, there’s a huge gap in fitness between the top and bottom 5 percent of each age group (the upper vs. lower lines). Second, it’s striking how steeply VO2 max declines with age, and how this decline corresponds to diminished functional capacity. The lower it goes, the less you can do.
For example, a thirty-five-year-old man with average fitness for his age—a VO2 max in the mid-30s—should be able to run at a ten-minute mile pace (6 mph). But by age seventy, only the very fittest 5 percent of people will still be able to manage this. Similarly, an average forty-five- to fifty-year-old will be able to climb stairs briskly (VO2 max = 32), but at seventy-five, such a feat demands that a person be in the top tier of their age group. Activities that are easy when we are young or middle-aged become difficult if not impossible as we get older. This explains why so many people are miserable in their Marginal Decade. They simply can’t do much of anything.
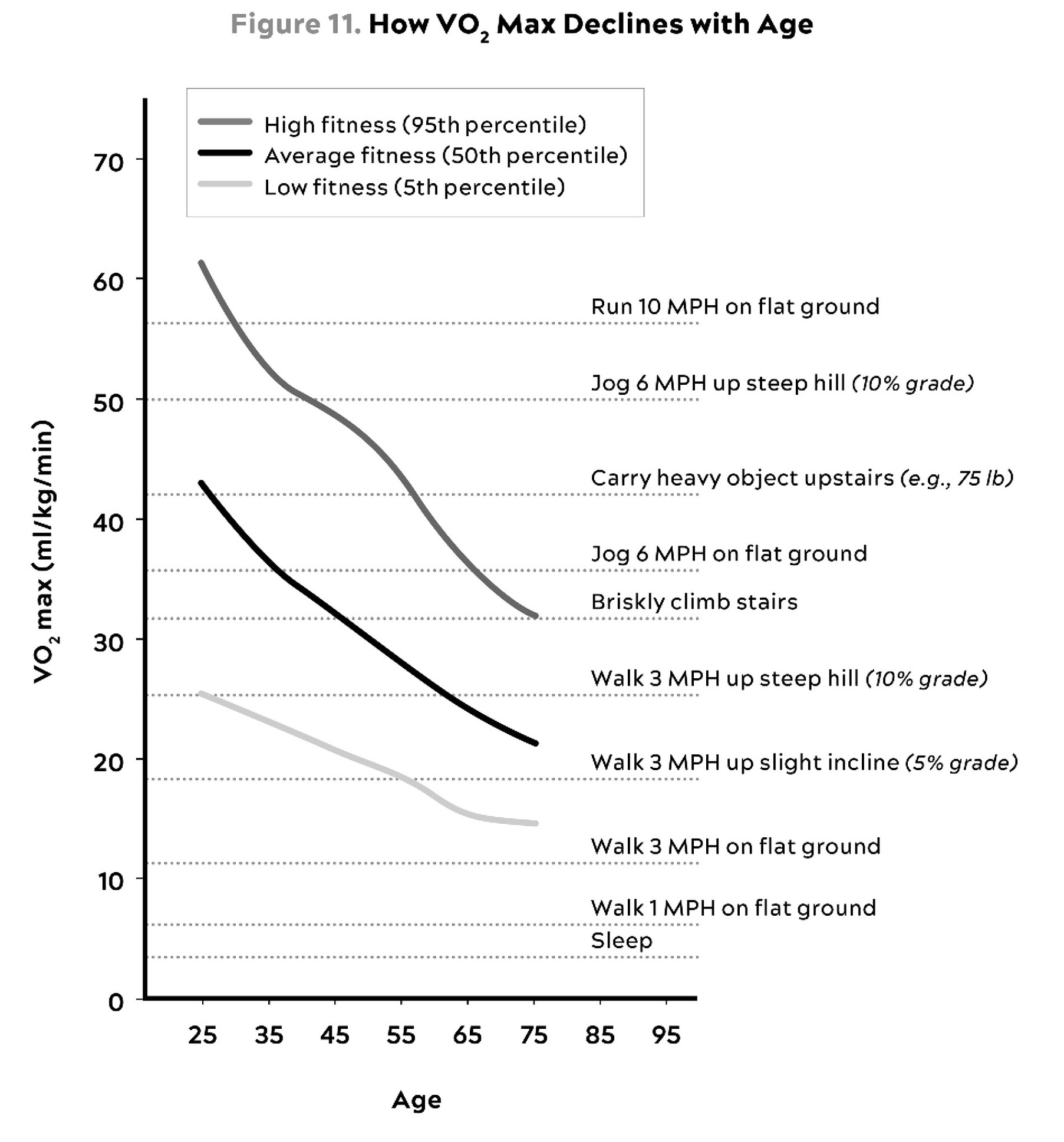
Source: Graph by Jayson Gifford, Brigham Young University, based on data from Ligouri (2020).
I push my patients to train for as high a VO2 max as possible, so that they can maintain a high level of physical function as they age. Ideally, I want them to target the “elite” range for their age and sex (roughly the top 2 percent). If they achieve that level, I say good job—now let’s reach for the elite level for your sex, but two decades younger. This may seem like an extreme goal, but I like to aim high, in case you haven’t noticed.
There is a logic to it. Let’s say you are a fifty-year-old woman, and you enjoy hiking in the mountains; that’s how you want to spend your retirement. That kind of activity would require a VO2 max of about 30, give or take. Let’s also assume, for the sake of argument, that you’re in the 50th percentile for your age; that puts you at about 32 ml/kg/min. You can do that hike now!
That seems like good news—but it’s really the bad news. Studies suggest that your VO2 max will decline by roughly 10 percent per decade—and up to 15 percent per decade after the age of fifty. So simply having average or even above-average VO2 max now just won’t cut it. We are planning for you to live for another thirty years, or forty. If you are only starting at 32 ml/kg/min now, at fifty, you can expect to be closer to 21 ml/kg/min at age eighty. These are not abstract numbers; they represent a profound decline in function. It’s the difference between walking easily up a flight of stairs versus struggling to even walk on an inclined surface. It’s a far cry from hiking in the Dolomites. To arrive in her ninth decade with a sufficient level of fitness to achieve her goal, our fifty-year-old would need to have a VO2 max of about 45 to 49 right now. This is the top tier for her sex, but two decades younger.
It is important that your goals reflect your own priorities—the activities that you enjoy, and what you want to be able to accomplish in your later decades. The more active you want or plan to be as you age, the more you need to train for it now.
Keep in mind, increasing your VO2 max by any amount is going to improve your life, not only in terms of how long you live but also how well you live, today and in the future. Improving your VO2 max from the very bottom quartile to the quartile above (i.e., below average) is associated with almost a 50 percent reduction in all-cause mortality, as we saw earlier. I believe that almost anyone is capable of achieving this—and they should, because the alternative is so unacceptable. Once maximal oxygen consumption or VO2 max drops below a certain level (typically about 18 ml/kg/min in men, and 15 in women), it begins to threaten your ability to live on your own. Your engine is beginning to fail.
This is why it’s so essential to train VO2 max in addition to zone 2. It’s a key to maintaining a fulfilling, independent life as you age. But it takes hard work over a long period of time to build it up and keep it up.
How trainable is VO2 max? The conventional wisdom, reflecting the bulk of the literature, suggests that it’s possible to improve elderly subjects’ aerobic capacity by about 13 percent over eight to ten weeks of training, and by 17 percent after twenty-four to fifty-two weeks, according to one review. That’s a good start, but I think it represents only the beginning of what is possible; as usual with Medicine 2.0, these studies are almost always too short. We are talking about a lifelong training program, not one that lasts only eight weeks. Everyone is different, in terms of their fitness potential and their response to training, but Mike Joyner believes that longer and more focused training can yield much larger gains over extended periods of time—periods measured in years, not weeks. I tell my patients that this is not a two-month project; it’s a two-year project.
It is not clear how much upside it is possible to achieve, but the literature suggests that sustained, diligent training can pay off. A small study of nine well-trained octogenarian endurance athletes (cross-country skiers) found that their average VO2 max was 38, versus 21 for a control group of untrained octogenarian men, a difference of more than 80 percent. That’s huge. The athletes had the aerobic capacity of people decades younger than them,[*3] while the men in the control group had declined so far that they were on the verge of losing their ability to live independently. True, the study subjects were lifelong athletes—but that’s also part of the point here. Our goal is to become elite athletes of aging.
The payoff is that increasing your VO2 max makes you functionally younger. One study found that boosting elderly subjects’ VO2 max by 6 ml/kg/min, or about 25 percent, was equivalent to subtracting twelve years from their age. If you are a man in your sixties and you are starting with a VO2 max of 30, you are more or less average for your age group (see figure 12). (Women typically have a somewhat lower average VO2 max by age, because of various factors, so an “average” woman in her sixties would be at about 25 ml/kg/min.) If you can boost that up to 35 via training, you will be squarely in the top 25 percent of your age group. Nice work. Now, here’s another way to look at it: In your sixties, you will have achieved the aerobic fitness of an average man in his fifties, a decade younger than you. If you can get it still higher, to 38 or 39, you will be the aerobic equivalent of an average thirty-something. This means you will have bought yourself a phase shift, like we talked about with the centenarians: you now have the fitness of someone decades younger than you. So give yourself a pat on the back; you’ve earned it.
The beauty of this is that VO2 max can always be improved by training, no matter how old you are. Don’t believe me? Then let me introduce you to an amazing Frenchman named Robert Marchand, who set an age-group world record in 2012 by cycling 24.25 kilometers in an hour, at the age of 101. Apparently, he wasn’t satisfied with that performance, so he decided he needed to train harder. Following a strict program designed by top coaches and physiologists, he managed to boost his VO2 max from an already-impressive 31 ml/kg/min up to 35 ml/kg/min, which would put him in the elite 2.5 percent of men in their eighties. Two years later, now 103, he came back and broke his own record, riding almost twenty-seven kilometers in an hour. That’s impressive, and it shows that it’s never too late to improve your VO2 max.
Even if we are not out to set world records, the way we train VO2 max is pretty similar to the way elite athletes do it: by supplementing our zone 2 work with one or two VO2 max workouts per week.
Where HIIT intervals are very short, typically measured in seconds, VO2 max intervals are a bit longer, ranging from three to eight minutes—and a notch less intense. I do these workouts on my road bike, mounted to a stationary trainer, or on a rowing machine, but running on a treadmill (or a track) could also work. The tried-and-true formula for these intervals is to go four minutes at the maximum pace you can sustain for this amount of time—not an all-out sprint, but still a very hard effort. Then ride or jog four minutes easy, which should be enough time for your heart rate to come back down to below about one hundred beats per minute. Repeat this four to six times and cool down.[*4]
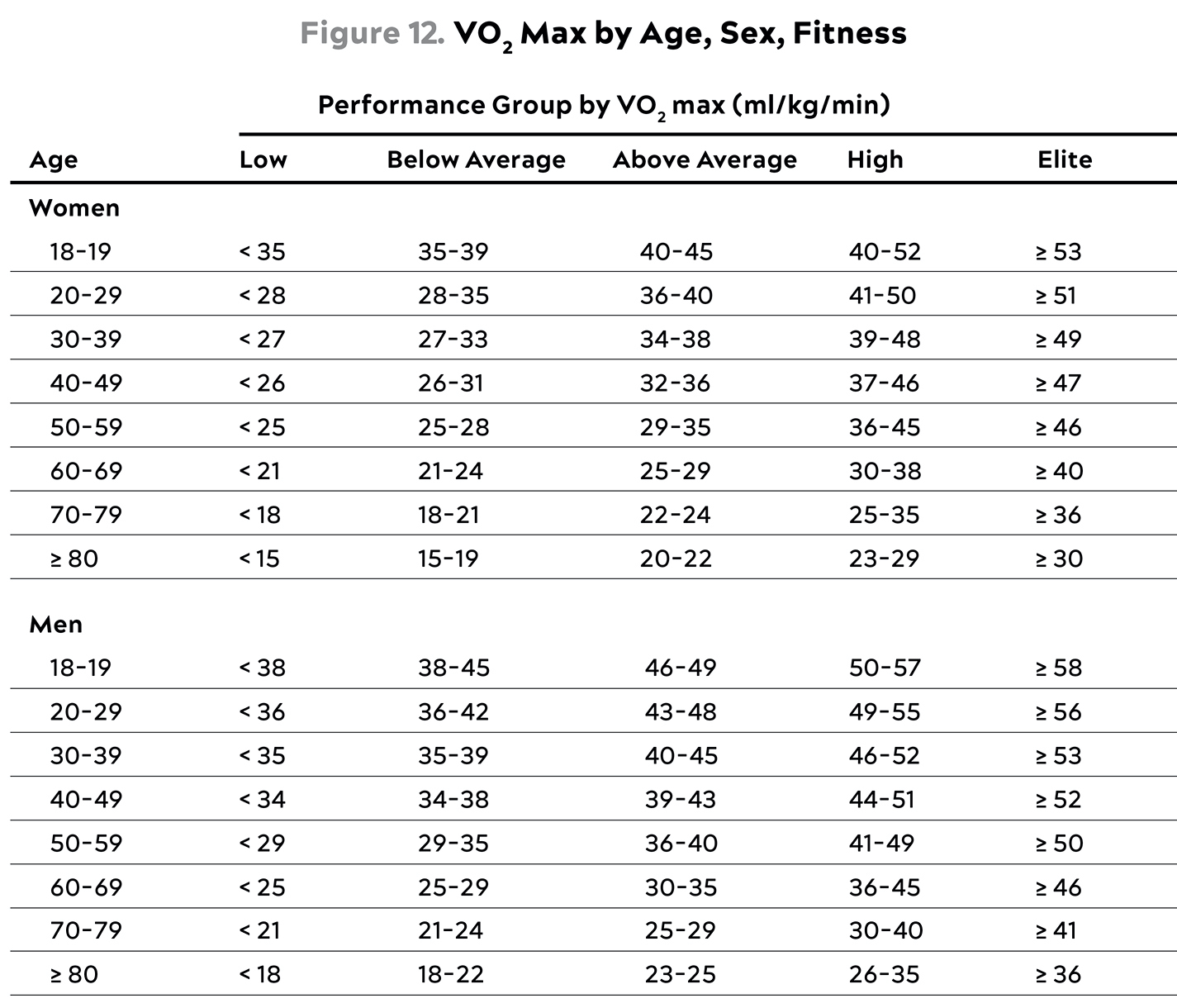
Source: Mandsager et al. (2018).
Group comparisons for VO2 max are Low (bottom 25%), Below Average (26th to 50th percentile), Above Average (51st to 75th percentile), High (75th to 97.6th percentile), and Elite (top 2.3%).
You want to make sure that you get as close to fully recovered as possible before beginning the next set. If you fail to recover sufficiently between sets, you will not be able to reach your peak effort in the working sets and you’ll consequently miss the desired adaptation. Also, be sure to give yourself enough time to warm up and then cool down from this intense effort.
The good news, I suppose, is that you don’t need to spend very much time in the pain cave. Unless you are training to be competitive in elite endurance sports like cycling, swimming, running, triathlon, or cross-country skiing, a single workout per week in this zone will generally suffice. You’ll pretty quickly find that it boosts your performance across the rest of your exercise program as well—and, more importantly, in the rest of your life.
I learned this lesson very vividly not long ago, when my wife and I had a very tight connection at Heathrow Airport in London. Anyone who has connected there knows that getting from Terminal 5 to Terminal 3 is basically a trip within a trip. The only way we were going to catch our connecting flight was to run the equivalent of a mile in less than eight minutes, while each carrying a twenty-pound suitcase. This was not going to be a zone 2 effort; we were going to have to go much harder than that, for eight straight minutes. We needed to be able to produce a burst of power that was much closer to our VO2 max than to zone 2.
In that moment, we were in a situation not all that different from what our hunter-gatherer ancestors frequently faced (apart from the setting, obviously). Besides being much more fun than traveling through airports, hunting requires 95 percent slow and steady effort, and 5 percent all-out intensity. If you were going to have a chance to kill the antelope or mammoth or whatever else you were tracking, you really needed that extra power to close the deal.
My point is that if you really stop to consider the kind of aerobic fitness that most people actually need in the course of their lives, it basically boils down to being really good at going slow for a long time, but also able to go hard and fast when needed. Training and maintaining a high level of aerobic fitness, and doing it now, is essential to preserving this range of function in your later years.
In a way, maximum aerobic output is like guitarist Nigel Tufnel’s special amplifier, in the classic film This Is Spinal Tap: Where most amps only let you turn the volume up to 10, his went up to 11. As he memorably explained, “It’s one higher.”
Every once in a while, it’s nice to have that range. We made our flight with a few seconds to spare.
Strength
Weight training has been a touchstone for me since I was fourteen years old and my best friend John and I, both wannabe prizefighters, first wandered into the gym at the Scarborough campus of the University of Toronto. It was a smelly dungeon two floors underground, inhabited by very sweaty dudes who absolutely lived to lift heavy metal weights. It had no heat, no windows, and no AC, so winters were freezing and summers were so hot it was not uncommon for someone to pass out after a max-effort set. We loved it. It was as mythical to us as Gold’s Gym at Venice Beach.
Back then, I went to the gym to pursue my boxing ambitions. I literally had no thought of what my life would look like after about age twenty-three. Now that I’m a middle-aged guy myself, I finally understand the seriousness with which those older guys approached their training. I am chasing a different dream—the Centenarian Decathlon, in case you forgot—but I suspect that I’m on the same page as them now.
The sad fact is that our muscle mass begins to decline as early as our thirties. An eighty-year-old man will have about 40 percent less muscle tissue (as measured by cross section of the vastus lateralis, aka the “quad” muscle of the thigh) than he did at twenty-five. But muscle mass may be the least important metric here. According to Andy Galpin, a professor of kinesiology at California State University, Fullerton, and one of the foremost authorities on strength and performance, we lose muscle strength about two to three times more quickly than we lose muscle mass. And we lose power (strength x speed) two to three times faster than we lose strength. This is because the biggest single change in the aging muscle is the atrophy of our fast twitch or type 2 muscle fibers. Ergo, our training must be geared towards improving these with heavy resistance training. Daily life and zone 2 endurance work may be enough to prevent atrophy of type 1 fibers—but unless you are working against significant resistance, your type 2 muscle fibers will wither away.
It takes much less time to lose muscle mass and strength than to gain it, particularly if we are sedentary. Even if someone has been training diligently, a short period of inactivity can erase many of those gains. If that inactivity stems from a fall or a broken bone, and lasts longer than a few days, it can often kick off a steep decline from which we may never fully recover, which is pretty much what happened with Sophie. A study of twelve healthy volunteers with an average age of sixty-seven found that after just ten days of bed rest, which is about what a person would experience from a major illness or orthopedic injury, study participants lost an average of 3.3 pounds of lean mass (muscle). That’s substantial, and it shows just how dangerous inactivity can be. If someone is sedentary and consuming excess calories, muscle loss accelerates, because one of the primary destinations of fat spillover is into muscle.
In its most extreme form, this muscle loss is called sarcopenia, as noted in chapter 11. Someone with sarcopenia will have low energy, feelings of weakness, and problems with balance. Sarcopenia is a prime marker for a broader clinical condition called frailty, where a person meets three of these five criteria: unintended weight loss; exhaustion or low energy; low physical activity; slowness in walking; and weak grip strength (about which more soon). It can become difficult to stand or walk, and they are at huge risk of falling and breaking bones.
Regaining that muscle, once we’ve gotten to this state, is no easy task. One study looked at sixty-two frail seniors (average age seventy-eight) who engaged in a program of strength training and found that even after six months of pure strength training, half of the subjects did not gain any muscle mass. They also didn’t lose any muscle mass, likely thanks to the weight training, but the upshot is, it is very difficult to put on muscle mass later in life.
Another metric that we track closely in our patients is their bone density (technically, bone mineral density or BMD). We measure BMD in every patient, every year, looking at both of their hips and their lumbar spine using DEXA. This also measures body fat and lean mass, so it’s a useful tool across all of the body-composition domains that we care about.
These three bone regions are typically used to make a diagnosis of osteopenia or osteoporosis. The standard guidelines only recommend screening in women at age sixty-five or men at age seventy—which is classic Medicine 2.0, waiting until someone may be staring danger in the eye before doing anything. We think it’s important to get a handle on this much earlier, before any problems arise.
The fact is that bone density diminishes on a parallel trajectory to muscle mass, peaking as early as our late twenties before beginning a slow, steady decline. For women, this decline happens much more quickly once they hit menopause, if they are not on HRT (yet another reason we heavily favor HRT), because estrogen is essential for bone strength—in both men and women. Other risk factors for low bone density include genetics (family history), a history of smoking, long use of corticosteroids (e.g., for asthma or autoimmune conditions), drugs that block estrogen (e.g., women taking such drugs for breast cancer), low muscle mass (again), and being undernourished.
Why do we care so much? Just as with muscle, it comes down to protection. We want to slow this decline, armoring ourselves against injury and physical frailty. The mortality from a hip or femur fracture is staggering once you hit about the age of sixty-five. It varies by study, but ranges from 15 to 36 percent in one year—meaning that up to one-third of people over sixty-five who fracture their hip are dead within a year. Even if a person does not die from the injury, the setback can be the functional equivalent of death in terms of how much muscle mass and, hence, physical capacity is lost during the period of bed rest (recall how quickly people over sixty-five lose muscle mass when bedridden).
Our goal is to try to spot this issue, if it arises, decades before a potential fracture might occur. When we detect low or rapidly declining BMD in a middle-aged person, we use the following four strategies:
-
Optimize nutrition, focusing on protein and total energy needs (see nutrition chapters).
-
Heavy loading-bearing activity. Strength training, especially with heavy weights, stimulates the growth of bone—more than impact sports such as running (though running is better than swimming/cycling). Bones respond to mechanical tension and estrogen is the key hormone in mediating the mechanical signal (weight bearing) to a chemical one telling the body to lay down more bone.
-
HRT, if indicated.
-
Drugs to increase BMD, if indicated.
Ideally, we can solve the problem with the first two, but are not afraid to use the second two methods where appropriate. The takeaway for readers here is that your BMD is important, demanding at least as much attention as muscle mass, so you should at least check your BMD every few years. (Particularly if your primary sports are nonweight-bearing, like cycling or swimming.)
I think of strength training as a form of retirement saving. Just as we want to retire with enough money saved up to sustain us for the rest of our lives, we want to reach older age with enough of a “reserve” of muscle (and bone density) to protect us from injury and allow us to continue to pursue the activities that we enjoy. It is much better to save and invest and plan ahead, letting your wealth build gradually over decades, than to scramble to try to scrape together an individual retirement account in your late fifties and hope and pray that the stock market gods help you out. Like investing, strength training is also cumulative, its benefits compounding. The more of a reserve you build up, early on, the better off you will be over the long term.
Yet unlike some guys in the gym, I’m less concerned with how big my biceps are or how much I can bench press. Those might matter if you’re a bodybuilder or a powerlifter, but I’d argue they matter less in the Centenarian Decathlon (or in real life). A far more important measure of strength, I’ve concluded, is how much heavy stuff you can carry. I say this on the basis of my intuition but also research into hunter-gatherers and human evolution. Carrying is our superpower as a species. It’s one reason why we have thumbs, as well as long legs (and arms). No other animal is capable of carrying large objects from one place to another with any efficiency. (And the ones that can, like horses and other livestock, do so only because we bred and trained and harnessed them.) This frames how I view strength training in general. It’s largely about improving your ability to carry things.
I’ve always been a fan of carrying heavy objects with my hands. As a teenager working on a construction site over the summers, I always volunteered to haul tools and materials across the site, and today I still incorporate some kind of carrying, typically with dumbbells, kettlebells, or sandbags, into most of my workouts. I’ve also become semiobsessed with an activity called rucking, which basically means hiking or walking at a fast pace with a loaded pack on your back. Three or four days a week, I’ll spend an hour rucking around my neighborhood, up and down hills, typically climbing and descending several hundred feet over the course of three or four miles. The fifty- to sixty-pound pack on my back makes it quite challenging, so I’m strengthening my legs and my trunk while also getting in a solid cardiovascular session. The best part is that I never take my phone on these outings; it’s just me, in nature, or maybe with a friend or a family member or a houseguest (for whom rucking is mandatory; I keep two extra rucksacks in the garage).
I was introduced to this pastime by Michael Easter in his eye-opening book The Comfort Crisis. His intriguing thesis is that because we have removed all discomfort of any kind from modern life, we have lost touch with the fundamental skills (not to mention the frequent suffering) that once defined what it meant to be human. Carrying stuff over long distances is one of these skills; our ancestors likely had to range far and wide to hunt food for their families and then carry their kills back to camp to feed everyone. But it’s so effective that the military has incorporated it into their training.
“Carrying shaped our species,” he says. “Our ancestors carried often. It gave them robust functional strength and endurance that was likely very protective. But we’ve engineered carrying out of our lives, just as we have many other forms of discomfort. Rucking is a practical way to add carrying back into our lives.”
The main difference is that instead of carrying sixty pounds of antelope meat in my pack, I’m typically hauling heavy metal weights, which are admittedly less appetizing. One thing I specifically focus on when rucking is the hills. Going uphill gives me a chance to push my VO2 max energy system; first-time ruckers are amazed at how taxing it is to walk up a 15 percent grade with even twenty pounds on your back—and then walk back down. (A good goal is to be able to carry one-quarter to one-third of your body weight once you develop enough strength and stamina. My daughter and wife routinely carry this much when they join me.)
As great as rucking is, it’s not the only thing I rely on to build my strength. Fundamentally I structure my training around exercises that improve the following:
-
Grip strength, how hard you can grip with your hands, which involves everything from your hands to your lats (the large muscles on your back). Almost all actions begin with the grip.
-
Attention to both concentric and eccentric loading for all movements, meaning when our muscles are shortening (concentric) and when they are lengthening (eccentric). In other words, we need to be able to lift the weight up and put it back down, slowly and with control. Rucking down hills is a great way to work on eccentric strength, because it forces you to put on the “brakes.”
-
Pulling motions, at all angles from overhead to in front of you, which also requires grip strength (e.g., pull-ups and rows).
-
Hip-hinging movements, such as the deadlift and squat, but also step-ups, hip-thrusters, and countless single-leg variants of exercises that strengthen the legs, glutes, and lower back.
I focus on these four foundational elements of strength because they are the most relevant to our Centenarian Decathlon—and also to living a fulfilling and active life in our later decades. If you can grip strongly, you can open a jar with ease. If you can pull, you can carry groceries and lift heavy objects. If you can do a hip-hinge correctly, you can get up out of a chair with no problem. You’re setting yourself up to age well. It’s not about how much weight you can deadlift now, but how well you will function in twenty or thirty or forty years.
I put grip strength first because it’s something that most people don’t really think about. Even I was surprised to discover that there is an enormous body of literature linking better grip strength in midlife and beyond to decreased risk of overall mortality.[*5] The data are as robust as for VO2 max and muscle mass, in fact. Many studies suggest that grip strength—literally, how hard you can squeeze something with one hand—predicts how long you are likely to live, while low grip strength in the elderly is considered to be a symptom of sarcopenia, the age-related muscle atrophy we just discussed. In these studies, grip strength is likely acting as a proxy for overall muscle strength, but it is also a broader indicator of general robustness and the ability to protect yourself if you slip or lose balance. If you have the strength to grab a railing, or a branch, and hold on, you might avoid a fall.
Surprisingly, given the extent to which fitness and gym-going have become so commonplace in our culture in the last few decades, American adults actually seem to have far weaker grip strength—and thus less muscle mass—than they did even a generation ago. In 1985, men ages twenty to twenty-four had an average right-handed grip strength of 121 pounds, while in 2015, men of the same age averaged just 101 pounds. This suggests that people now in their thirties are entering midlife with much less strength than their parents, which could lead to problems as they get older.
Grip strength is important at all ages. Every interaction that we have begins with our hands (or feet, as we’ll discuss later). Our grip is our primary point of contact in almost any physical task, from swinging a golf club to chopping wood; it is our interface with the world. If our grip is weak, then everything else is compromised.
Training grip strength is not overly complicated. One of my favorite ways to do it is the classic farmer’s carry, where you walk for a minute or so with a loaded hex bar or a dumbbell or kettlebell in each hand. (Bonus points: Hold the kettlebell up vertically, keeping your wrist perfectly straight and elbow cocked at ninety degrees, as though you were carrying it through a crowded room.) One of the standards we ask of our male patients is that they can carry half their body weight in each hand (so full body weight in total) for at least one minute, and for our female patients we push for 75 percent of that weight. This is, obviously, a lofty goal—please don’t try to do it on your next visit to the gym. Some of our patients need as much as a year of training before they can even attempt this test.
In general, we urge our new patients to begin with far less weight than they have lifted in the past, sometimes even dropping down to body weight exercises at first. As we will see in the next chapter, on stability, it is far more important to learn and practice ideal movement patterns than to be pounding heavy weights all the time. That said, a farmer’s carry is pretty straightforward (weight in each hand, arms at sides, walk). The most important tip is to keep your shoulder blades down and back, not pulled up or hunched forward. If you are new to strength training, start with light weights, even as low as ten to fifteen pounds, and work up from there.
Another way to test your grip is by dead-hanging from a pull-up bar for as long as you can. (This is not an everyday exercise; rather, it’s a once-in-a-while test set.) You grab the bar and just hang there, supporting your body weight. This is a simple but sneakily difficult exercise that also helps strengthen the critically important scapular (shoulder) stabilizer muscles, which we will talk about in the next chapter. Here we like to see men hang for at least two minutes and women for at least ninety seconds at the age of forty. (We reduce the goal slightly for each decade past forty.)
No discussion of strength is complete without mentioning concentric and especially eccentric loading. Again, eccentric loading means loading the muscle as it is lengthening, such as when you lower a bicep curl. It’s more intuitive when lifting something to focus on the concentric phase, such as curling the dumbbell with your biceps. This is the strength of a muscle getting shorter. One of the tests we have our patients perform is stepping onto and off an eighteen-inch block and taking three full seconds to reach the ground (a forward step down, like descending a very tall step). The stepping up part is comparatively easy, but most people initially struggle with a controlled three-second descent. That requires eccentric strength and control. (I’ll talk about step-ups and step-downs in detail at the end of chapter 13.)
In life, especially as we age, eccentric strength is where many people falter. Eccentric strength in the quads is what gives us the control we need when we are moving down an incline or walking down a set of stairs. It’s really important to keep us safe from falls and from orthopedic injuries. When we can eccentrically load our muscles, it also prevents our joints from taking excess stress, especially our knees. Think about creeping slowly down a very steep hill versus running down in an uncontrolled manner. The difference in force transmission to your knees is dramatic (as is the difference in likely outcomes—safe descent versus faceplant and likely knee injury).
Training eccentric strength is relatively simple. Big picture, it means focusing on the “down” phase of lifts ranging from pull-ups or pull-downs to deadlifts to rows; rucking downhill, carrying a weighted pack, is a great way to build both eccentric strength as well as spatial awareness and control, which are important parts of stability training (next chapter). It also helps protect against knee pain. You don’t need to do this for every rep of every set. Sometimes you just want to focus on moving the weight quickly or moving a heavier load, but make sure at some point in each workout that you are taking the time to cue the eccentric phase of your lifts.
Next is pulling, which is closely related to grip strength. Pulling motions are how we exert our will on the world, whether we are hoisting a bag of groceries out of the car trunk or climbing El Capitan. It is an anchor movement. In the gym, it typically takes the form of rows, where you’re pulling the weight toward your body, or pull-ups. A rowing machine, something I love to use for VO2 max training, is another simple and effective way to work on pulling strength.
The final foundational element of strength is hip-hinging, which is what it sounds like: You bend at the hips—not the spine—to harness your body’s largest muscles, the gluteus maximus and the hamstrings. (I repeat: Do not bend your spine.) It is a very powerful move that is essential to life. Whether you are launching off an Olympic ski jump, picking up a lucky penny off the sidewalk, or simply getting up out of a chair, you are hip-hinging.
Hip-hinging under high axial load, as with a heavy deadlift or squat, should be approached with care because of the risk of injury to the spine. This is why we have our patients work up to weighted hip-hinging very slowly, typically beginning with single-leg step-ups (see description below) and split-stance Romanian deadlift, either without weights or with only very light weights held in the hands.
Normally, this would be the section where I would write a lengthy treatise on the finer points of how to do pull-ups and hip-hinges. I’ve come to the conclusion that they can’t actually be done right without dozens of pictures and thousands of words, in a book that is already too long. There are two reasons why I have decided not to give the details. One, I believe that this type of content is best learned in person, from someone who knows how to cue the movements. For example, the “hard” part about teaching a proper hip-hinge is not illustrating the correct position of the spine relative to the femur and lower leg, or the angle of the hips, in a diagram. The hard part is knowing how to eccentrically load the glutes and hamstrings before you hinge, and how to feel your feet pushing into the floor evenly across the full surface of your foot.
If this is hard to follow, you see exactly why I’ve come to the conclusion that the best way to communicate this information to you, in a way that is actionable, is to show you, as opposed to telling you. And the best way I can show you, shy of working out with you, is having you watch me do these exercises over video, with my colleague Beth Lewis cuing me. (I’ve placed a link to these videos, and a brief description, at the end of the next chapter.)
The second reason I’ve opted not to describe all these exercises in detail is that when new patients come to us, we typically have them stop strength training, at least with heavy weights. Our first step is to put them through a series of strength and movement tests designed to assess not only their physical condition but also their degree of stability. So before you do anything in the gym, I would urge you to read the next chapter, to begin to understand the crucial and complex concept of stability.