CHAPTER 11
Exercise
The Most Powerful Longevity Drug
I never won a fight in the ring; I always won in preparation.
—Muhammad Ali
Several years ago, my friend John Griffin pinged me with a question about how he should be exercising: Should he be doing more cardio or more weights? What did I think?
“I’m really confused by all the contradictory stuff I’m seeing out there,” he wrote.
Behind his seemingly simple question, I heard a plea for help. John is a smart guy with an incisive mind, and yet even he was frustrated by all the conflicting advice from “experts” touting this or that workout as the sure path to perfect health. He couldn’t figure out what he needed to be doing in the gym or why.
This was before I had gotten back into the full-time practice of medicine. At the time, I was immersed in the world of nutrition research, which if anything is even more confounding than exercise science, rife with contradictory findings and passionately held dogmas backed by flimsy data. Are eggs bad or good? What about coffee? It was driving me nuts too.
I started typing out a reply and kept on writing. By the time I hit SEND, I had written close to two thousand words, way more than he asked for. The poor guy just wanted a quick answer, not a memo. I didn’t stop there either. I later expanded that email into a ten-thousand-word manifesto on longevity, which eventually grew into the book you are holding in your hands.[*1]
Clearly, something about John’s question triggered me. It’s not that I was a passionate devotee of strength training over endurance, or vice versa; I’d done plenty of both. I was reacting to the binary nature of his question. In case you haven’t figured it out by now, I’m not fond of the way we reduce these complex, nuanced, vitally important questions down to simple either-ors. Cardio or weights? Low-carb or plant-based? Olive oil or beef tallow?
I don’t know. Must we really take sides?
The problem, and we will see this again in the nutrition chapters, is that we have this need to turn everything into a kind of religious war over which is the One True Church. Some experts insist that strength training is superior to cardio, while an equal number assert the opposite. The debate is as endless as it is pointless, sacrificing science on the altar of advocacy. The problem is that we are looking at these hugely important domains of life—exercise, but also nutrition—through a far too narrow lens. It’s not about which side of the gym you prefer. It’s so much more essential than that.
More than any other tactical domain we discuss in this book, exercise has the greatest power to determine how you will live out the rest of your life. There are reams of data supporting the notion that even a fairly minimal amount of exercise can lengthen your life by several years. It delays the onset of chronic diseases, pretty much across the board, but it is also amazingly effective at extending and improving healthspan. Not only does it reverse physical decline, which I suppose is somewhat obvious, but it can slow or reverse cognitive decline as well. (It also has benefits in terms of emotional health, although those are harder to quantify.)
So if you adopt only one new set of habits based on reading this book, it must be in the realm of exercise. If you currently exercise, you will likely want to rethink and modify your program. And if exercise is not a part of your life at the moment, you are not alone—77 percent of the US population is like you. Now is the time to change that. Right now. Even a little bit of daily activity is much better than nothing. Going from zero weekly exercise to just ninety minutes per week can reduce your risk of dying from all causes by 14 percent. It’s very hard to find a drug that can do that.
Thus, my answer to questions like the one my friend John Griffin asked me is yes and yes. Yes, you should be doing more cardio. And yes, you should be lifting more weights.
At the other end of the spectrum, if you’re someone like me who has been exercising since kindergarten, I promise you these chapters will offer you insights about how to better structure your program—not to achieve a faster marathon time or bragging rights at your gym, but to live a longer and better life, and most important, a life in which you can continue enjoying physical activity well into your later years.
It’s obviously not a revelation that exercise is good for you; so is chicken soup if you have a sore throat. But not many people realize how profound its effects really are. Study after study has found that regular exercisers live as much as a decade longer than sedentary people. Not only do habitual runners and cyclists tend to live longer, but they stay in better health, with less morbidity from causes related to metabolic dysfunction. For those who are not habitual exercisers (yet), you’re in luck: The benefits of exercise begin with any amount of activity north of zero—even brisk walking—and go up from there. Just as almost any diet represents a vast improvement over eating only fast food, almost any exercise is better than remaining sedentary.
Although my medical school classmates and I learned almost zilch about exercise, let alone how to “prescribe” it to patients, Medicine 2.0 does at least recognize its value. Unfortunately, the advice rarely goes beyond generic recommendations to move more and sit less. The US government’s physical activity guidelines suggest that “active adults” engage in at least 30 minutes of “moderate-intensity aerobic activity,” five times per week (or 150 minutes in total). This is to be supplemented with two days of strength training, targeting “all major muscle groups.”
Imagine if doctors were this vague about cancer treatment:
DOCTOR: Ms. Smith, I’m sorry to have to tell you this, but you have colon cancer.
MS. SMITH: That’s terrible news, Doctor. What should I do?
DOCTOR: You need chemotherapy treatment.
MS. SMITH: What kind of chemotherapy? What dose? How often? For how long? What about the side effects?
DOCTOR: ¯\_(ツ)_/¯
We need more specific guidance to help us achieve our goals, and to do so in a way that is efficient but also safe. But first, I want to spend some time exploring why exercise is so important, because I find the data around it to be so persuasive. When I share these data with my patients, they are rarely surprised by the fact that high aerobic fitness and strength are associated with longer lifespan and healthspan—but they are always amazed by the magnitude of the benefit. The data on exercise tell us, with great clarity, that the more we do, the better off we will be.
Let’s start with cardiorespiratory or aerobic fitness. This means how efficiently your body can deliver oxygen to your muscles, and how efficiently your muscles can extract that oxygen, enabling you to run (or walk) or cycle or swim long distances. It also comes into play in daily life, manifesting as physical stamina. The more aerobically fit you are, the more energy you will have for whatever you enjoy doing—even if your favorite activity is shopping.
It turns out that peak aerobic cardiorespiratory fitness, measured in terms of VO2 max, is perhaps the single most powerful marker for longevity. VO2 max represents the maximum rate at which a person can utilize oxygen. This is measured, naturally, while a person is exercising at essentially their upper limit of effort. (If you’ve ever had this test done, you will know just how unpleasant it is.) The more oxygen your body is able to use, the higher your VO2 max.
Our human body has an amazing ability to respond to the demands placed on it. Let’s say I’m just sitting on the couch, watching a movie. At rest, someone my size might require about 300 ml of oxygen per minute in order to generate enough ATP, the chemical “fuel” that powers our cells, to perform all the physiological functions necessary to stay alive and watch the movie. This is a pretty low level of energy demand, but if I go outside and jog around my neighborhood, the energy demands ramp up. My breathing quickens, and my heart rate accelerates to help me extract and utilize ever more oxygen from the air I breathe, in order to keep my muscles working. At this level of intensity, someone my size might require 2,500 to 3,000 ml of oxygen per minute, an eight- to tenfold increase from when I was sitting on the couch. Now, if I start running up a hill as fast as I can, my body’s oxygen demand will increase from there: 4,000 ml, 4,500 ml, even 5,000 ml or more depending on the pace and my fitness level. The fitter I am, the more oxygen I can consume to make ATP, and the faster I can run up that hill.
Eventually, I will reach the point at which I just can’t produce any more energy via oxygen-dependent pathways, and I’ll be forced to switch over to less efficient, less sustainable ways of producing power, such as those used in sprinting. The amount of oxygen that I am using at this level of effort represents my VO2 max. (And not long after that, I will “fail,” meaning I am no longer able to continue running up the hill at that pace.) VO2 max is typically expressed in terms of the volume of oxygen a person can use, per kilogram of body weight, per minute. An average forty-five-year-old man will have a VO2 max around 40 ml/kg/min, while an elite endurance athlete will likely score in the high 60s and above. An unfit person in their thirties or forties, on the other hand, might score only in the high 20s on a VO2 max test, according to Mike Joyner, an exercise physiologist and researcher at the Mayo Clinic. They simply won’t be able to run up that hill at all.[*2] The higher someone’s VO2 max, the more oxygen they can consume to make ATP, and the faster they can ride or run—in short, the more they can do.
This number is not just relevant to athletes; it turns out to be highly correlated with longevity. A 2018 study in JAMA that followed more than 120,000 people found that higher VO2 max (measured via a treadmill test) was associated with lower mortality across the board. The fittest people had the lowest mortality rates—by a surprising margin. Consider this: A person who smokes has a 40 percent greater risk of all-cause mortality (that is, risk of dying at any moment) than someone who does not smoke, representing a hazard ratio or (HR) of 1.40. This study found that someone of below-average VO2 max for their age and sex (that is, between the 25th and 50th percentiles) is at double the risk of all-cause mortality compared to someone in the top quartile (75th to 97.6th percentiles). Thus, poor cardiorespiratory fitness carries a greater relative risk of death than smoking.
That’s only the beginning. Someone in the bottom quartile of VO2 max for their age group (i.e., the least fit 25 percent) is nearly four times likelier to die than someone in the top quartile—and five times likelier to die than a person with elite-level (top 2.3 percent) VO2 max. That’s stunning. These benefits are not limited to the very fittest people either; even just climbing from the bottom 25 percent into the 25th to 50th percentile (e.g., least fit to below average) means you have cut your risk of death nearly in half, according to this study.
These results were confirmed by a much larger and more recent study, published in 2022 in the Journal of the American College of Cardiology, looking at data from 750,000 US veterans ages thirty to ninety-five (see figure 9). This was a completely different population that encompassed both sexes and all races, yet the researchers found a nearly identical result: someone in the least fit 20 percent has a 4.09 times greater risk of dying than a person in the top 2 percent of their age and sex category. Even someone of moderate fitness (40th to 60th percentile) is still at more than double the risk of all-cause mortality than the fittest group, this study found. “Being unfit carried a greater risk than any of the cardiac risk factors examined,” the authors concluded.
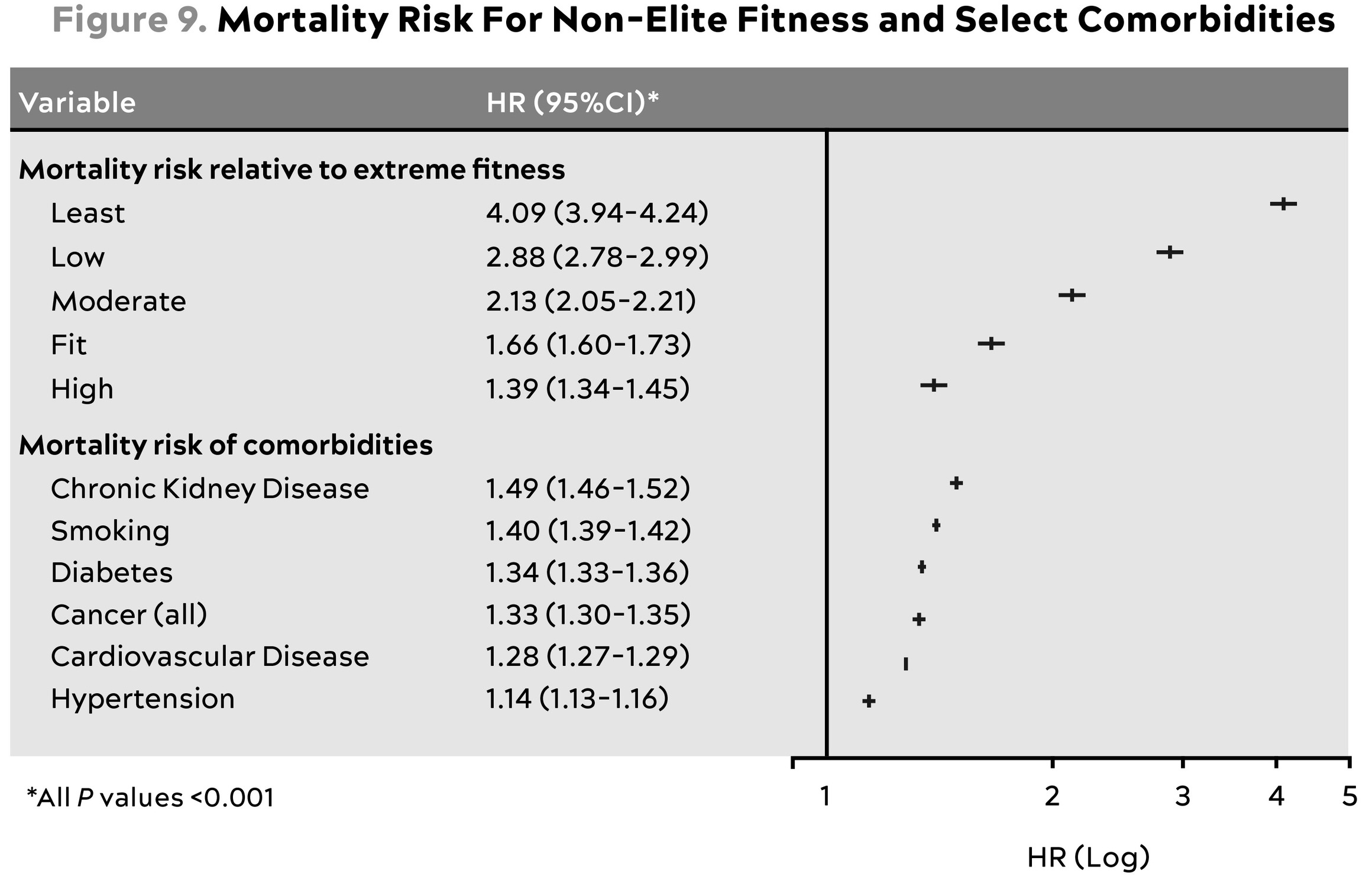
Source: Kokkinos et al. (2022).
This table expresses all-cause mortality risk for different fitness levels compared to individuals in the top 2% of VO2 max for their age and sex (“extreme fitness”) [TOP] and for various comorbidities—that is, people with versus without each illness. [BOTTOM] Fitness groups are divided by percentile: Least (<20th percentile); Low (21st to 40th percentile); Moderate (41st to 60th percentile); Fit (61st to 80th percentile); High (81st to 97th percentile).
Of course, there are almost certainly confounders here, just as with all observational study, including that of nutrition. But at least five factors[*3] increase my confidence in at least the partial causality of this relationship. First, the magnitude of the effect size is very large. Second, the data are consistent and reproducible across many studies of disparate populations. Third, there is a dose-dependent response (the fitter you are, the longer you live). Fourth, there is great biologic plausibility to this effect, via the known mechanisms of action of exercise on lifespan and healthspan. And fifth, virtually all experimental data on exercise in humans suggest that it supports improved health.
As the authors of the JAMA study concluded, “Cardiorespiratory fitness is inversely associated with long-term mortality with no observed upper limit of benefit [emphasis mine]. Extremely high aerobic fitness was associated with the greatest survival.”
I can’t tell you, from these data, that simply having a high VO2 max will offset your high blood pressure or your smoking habit, as much as these hazard ratios suggest it might. Without a randomized controlled trial, we can’t know for sure, but I kind of doubt it. But I can say with a very high degree of certainty that having a higher VO2 max is better for your overall health and longevity than having a lower VO2 max. Period.
Even better news, for our purposes, is that VO2 max can be increased via training. We can move the needle a lot on this measure of fitness, as we’ll see.
The strong association between cardiorespiratory fitness and longevity has long been known. It might surprise you, as it did me, to learn that muscle may be almost as powerfully correlated with living longer. A ten-year observational study of roughly 4,500 subjects ages fifty and older found that those with low muscle mass were at 40 to 50 percent greater risk of mortality than controls, over the study period. Further analysis revealed that it’s not the mere muscle mass that matters but the strength of those muscles, their ability to generate force. It’s not enough to build up big pecs or biceps in the gym—those muscles also have to be strong. They have to be capable of creating force. Subjects with low muscle strength were at double the risk of death, while those with low muscle mass and/or low muscle strength, plus metabolic syndrome, had a 3 to 3.33 times greater risk of all-cause mortality.
Strength may even trump cardiorespiratory fitness, at least one study suggests. Researchers following a group of approximately 1,500 men over forty with hypertension, for an average of about eighteen years, found that even if a man was in the bottom half of cardiorespiratory fitness, his risk of all-cause mortality was still almost 48 percent lower if he was in the top third of the group in terms of strength versus the bottom third.[*4]
It’s pretty much the same story we saw with VO2 max: The fitter you are, the lower your risk of death. Again, there is no other intervention, drug or otherwise, that can rival this magnitude of benefit. Exercise is so effective against diseases of aging—the Horsemen—that it has often been compared to medicine.
John Ioannidis, a Stanford scientist with a penchant for asking provocative questions, decided to test this metaphor literally, running a side-by-side comparison of exercise studies versus drug studies. He found that in numerous randomized clinical trials, exercise-based interventions performed as well as or better than multiple classes of pharmaceutical drugs at reducing mortality from coronary heart disease,[*5] prediabetes or diabetes, and stroke.
Even better: You don’t need a doctor to prescribe exercise for you.
Much of this effect, I think, likely has to do with improved mechanics: exercise strengthens the heart and helps maintain the circulatory system. As we’ll see later in this chapter, it also improves the health of the mitochondria, the crucial little organelles that produce energy in our cells (among other things). That, in turn, improves our ability to metabolize both glucose and fat. Having more muscle mass and stronger muscles helps support and protect the body—and also maintains metabolic health, because those muscles consume energy efficiently. The list goes on and on, but simply put, exercise helps the human “machine” perform far better for longer.
At a deeper biochemical level, exercise really does act like a drug. To be more precise, it prompts the body to produce its own, endogenous drug-like chemicals. When we are exercising, our muscles generate molecules known as cytokines that send signals to other parts of our bodies, helping to strengthen our immune system and stimulate the growth of new muscle and stronger bones. Endurance exercise such as running or cycling helps generate another potent molecule called brain-derived neurotrophic factor, or BDNF, that improves the health and function of the hippocampus, a part of the brain that plays an essential role in memory. Exercise helps keep the brain vasculature healthy, and it may also help preserve brain volume. This is why I view exercise as a particularly important part of the tool kit for patients at risk of developing Alzheimer’s disease—such as Stephanie, the woman with the high-risk Alzheimer’s genes whom we met in chapter 9.
The data demonstrating the effectiveness of exercise on lifespan are as close to irrefutable as one can find in all human biology. Yet if anything, I think exercise is even more effective at preserving healthspan than extending lifespan. There is less hard evidence here, but I believe that this is where exercise really works its magic when applied correctly. I tell my patients that even if exercise shortened your life by a year (which it clearly does not), it would still be worthwhile purely for the healthspan benefits, especially in middle age and beyond.
One of the prime hallmarks of aging is that our physical capacity erodes. Our cardiorespiratory fitness declines for various reasons that begin with lower cardiac output, primarily due to reduced maximum heart rate. We lose strength and muscle mass with each passing decade, our bones grow fragile and our joints stiffen, and our balance falters, a fact that many men and women discover the hard way, by falling off a ladder or while stepping off a curb.
To paraphrase Hemingway, this process happens in two ways: gradually, and then suddenly. The reality of the situation is that old age can be really tough on our bodies. Longitudinal and cross-sectional studies find that fat-free mass (meaning mostly muscle mass) and activity levels remain relatively consistent as people age from their twenties and thirties into middle age. But both physical activity levels and muscle mass decline steeply after about age sixty-five, and then even more steeply after about seventy-five. It’s as if people just fall off a cliff sometime in their mid-seventies.
By age eighty, the average person will have lost eight kilograms of muscle, or about eighteen pounds, from their peak. But people who maintain higher activity levels lose much less muscle, more like three to four kilograms on average. While it’s not clear which direction the causation flows here, I suspect it’s probably both ways: people are less active because they are weaker, and they are weaker because they are less active.
Continued muscle loss and inactivity literally puts our lives at risk. Seniors with the least muscle mass (also known as lean mass) are at the greatest risk of dying from all causes. One Chilean study looked at about one thousand men and four hundred women, with an average age of seventy-four at enrollment. The researchers divided the subjects into quartiles, based on their appendicular lean mass index (technically, the muscle mass of their extremities, arms and legs, normalized to height), and followed them over time. After twelve years, approximately 50 percent of those in the lowest quartile were dead, compared to only 20 percent of those in the highest quartile for lean mass. While we can’t establish causality here, the strength and reproducibility of findings like this suggest this is more than just a correlation. Muscle helps us survive old age.
This is another area where lifespan and healthspan overlap to a great extent. That is, I suspect that having more muscle mass delays death precisely because it also preserves healthspan. This is why I place so much emphasis on maintaining our musculoskeletal structure—which I call the “exoskeleton,” à la Terminator, for lack of a better term.
Your exoskeleton (muscle) is what keeps your actual skeleton (bones) upright and intact. Having more muscle mass on your exoskeleton appears to protect you from all kinds of trouble, even adverse outcomes following surgery—but most important, it is highly correlated with a lower risk of falling, a leading but oft-ignored cause of death and disability in the elderly. As figure 10 reveals, falls are by far the leading cause of accidental deaths in those ages sixty-five and older—and this is without even counting the people who die three or six or twelve months after their nonfatal but still serious fall pushed them into a long and painful decline. Eight hundred thousand older people are hospitalized for falls each year, according to the CDC.

Source: CDC (2021).
I believe this association likely works both ways: someone with more muscle mass is less likely to fall and injure themselves, while those who are less likely to fall for other reasons (better balance, more body awareness) will also have an easier time maintaining muscle mass. Conversely, muscle atrophy and sarcopenia (age-related muscle loss) increase our risk of falling and possibly requiring surgery—while at the same time worsening our odds of surviving said surgery without complications. Just as with VO2 max, it is important to maintain muscle mass at all costs.
Exercise in all its forms is our most powerful tool for fighting this misery and reducing our risk of death across the board. It slows the decline, not just physically but across all three vectors of healthspan, including cognitive and emotional health. A recent study of older British adults found that those with sarcopenia at baseline were nearly six times likelier to report having a low quality of life a decade later than those who had maintained more muscle mass.
This is what we want to avoid. We can avoid it with the help of this powerful “drug” called exercise that miraculously extends lifespan and improves healthspan. The difference is that it requires much more work and knowledge than simply taking a pill. But the more effort you’re willing to put in now, the more benefit you’ll reap in the future.
This is why I place such an emphasis on weight training—and doing it now, no matter your age. It is never too late to start; my mom did not begin lifting weights until she was sixty-seven, and it has changed her life. There are dozens of studies showing that strength training programs can significantly improve the mobility and physical function of subjects who are obese, or recovering from cancer treatment, even those who are already elderly and frail. Therefore, I will find a way to lift heavy weights in some way, shape, or form four times per week, no matter what else I am doing or where I might be traveling.
But exercise gets little more than lip service from Medicine 2.0. When was the last time your doctor tested your grip strength or asked you a detailed question about your strength training? Does your doctor know your VO2 max? Or have they offered training suggestions for how to improve it? I’m guessing that has happened precisely never—because none of what we’re covering here or in the nutrition chapters is even considered to rise to the level of “healthcare,” at least in our system. Some insurance companies offer discounts or incentives for members to go to the gym, but the kind of focused attention that I think we all need (including me) is well beyond the purview of most physicians.
It’s only after we get injured or become so weak that we are in danger of losing our independence, that we are deemed eligible for physical therapy and rehabilitation. So think of what follows as “prehab”—physical therapy before you need it.
When I talk with my patients about exercise, I often bring them back to the story of Sophie, my friend Becky’s mother, whom we met in chapter 3. She had actually been relatively active, even in retirement. She played golf once or twice a week and worked most days in her garden. It wasn’t a structured “exercise” program; she was just doing the things she loved. But then she injured her shoulder, and then her knee, requiring surgery for both. Even after surgery, she was never able to recover fully. Her activity level dropped off almost to zero. As Becky related to me, her mother mostly sat around the house, feeling depressed. Her cognitive decline fairly quickly ensued.
This made me incredibly sad as I sat there in the pew at her funeral. Yet her story was all too familiar. We have all seen older friends and relatives go through a similar ordeal, slowly (or not slowly) weakening until they can no longer find enjoyment in the things they once loved to do. What could have been done, I wondered, to change Sophie’s fate?
Had she simply needed to “exercise more”? Go to the gym and use the elliptical? Would that have saved her somehow?
It wasn’t clear that the answer was that simple. I had done plenty of exercise in my own life, but by the time of Sophie’s funeral I was nursing a handful of my own pet injuries that I’d accumulated over the years. Fit as I was, it wasn’t clear that I was on a better path than Sophie had been.
For most of my life, I’ve been obsessive with respect to fitness, always focusing on one particular sport—and inevitably taking it to an extreme. After I had burned myself out on boxing, then running, and finally long-distance open-water swimming, I turned to cycling. I went all in: My primary aim in life was to win the local cycling time-trial series, a twenty-kilometer individual race against the clock that almost nobody else cared about. I spent hours analyzing power-meter data and calculating my coefficient of aerodynamic drag, looking to shave precious seconds from my times using dorky models that I built in Excel.
The truth was that I had become pretty useless at everything except pedaling my road bike as fast as possible for twenty kilometers. I possessed a high VO2 max and I could produce a lot of power through the pedals, but I was not truly strong or flexible, and I did not have great balance or stability. I was a one-dimensional athlete, and if I had kept it up, I might have ended up with my spine fused into my time-trial tuck, still able to ride my bike but unable to do anything else useful, especially with my upper body. I eventually quit competitive cycling because it became clear that at a certain point this obsessive approach becomes unsustainable in virtually any activity. How many old marathon runners do you know who are still racing? Probably not many.
After that, I fell into this kind of directionless limbo where I bounced around between different fitness activities. I tried to get back into running. I went to Pilates classes with my wife. I did Barry’s Bootcamp for a time. You name it, I tried it. Then I joined a boutique fitness chain that specializes in high-intensity interval training, or HIIT. I enjoyed the fast-paced workouts they offered, like treadmill sprints and thirty-second Burpee blocks, and it took a fraction of the time that cycling did, so I was happy about that. But I didn’t have a goal other than “exercising.”
All this changed as I sat in the pew of the church at Sophie’s funeral. Officially, she had died from pneumonia, but what had really killed her, I realized, was the slow gravitational pull of aging on her body. That had not begun in the last year or even the last decade of her life. It had been working against her, pulling her down, since before I had met her—for decades. And it was killing the rest of us, too: her daughter, Becky, along with my patients, myself, and everyone reading this book is likely headed for the same steep decline.
That thought saddened me to my core. But then it hit me: the only way that we would be able to fight this was to adopt the philosophy of a decathlete—and apply it to aging.
Of all Olympic athletes, the decathletes are most revered. The male and female winners of the gold medal are declared the “World’s Greatest Athletes.” Yet they are not the best at any of the ten individual events in which they compete; they likely would not even medal. But they are still considered the greatest because they are remarkably good at so many different events. They are true generalists—yet they train like specialists.
We need to adopt a similar approach to aging, I decided: each of us needs to be training for the Centenarian Decathlon.
The Centenarian Decathlon
What in the world is the Centenarian Decathlon?
I’m not talking about an actual competition among hundred-year-olds, although similar events do already exist: the National Senior Games, held every other year, brings together remarkable older athletes, some of them in their nineties and beyond. The record for the hundred-meter dash for women ages one hundred and up is about forty-one seconds.
The Centenarian Decathlon is a framework I use to organize my patients’ physical aspirations for the later decades of their lives, especially their Marginal Decade. I know, it’s a somewhat morbid topic, thinking about our own physical decline. But not thinking about it won’t make it any less inevitable.
Think of the Centenarian Decathlon as the ten most important physical tasks you will want to be able to do for the rest of your life. Some of the items on the list resemble actual athletic events, while some are closer to activities of daily living, and still others might reflect your own personal interests. I find it useful because it helps us visualize, with great precision, exactly what kind of fitness we need to build and maintain as we get older. It creates a template for our training.
I start by presenting my patients with a long list of physical tasks that might include some of the following:
-
Hike 1.5 miles on a hilly trail.
-
Get up off the floor under your own power, using a maximum of one arm for support.
-
Pick up a young child from the floor.
-
Carry two five-pound bags of groceries for five blocks.
-
Lift a twenty-pound suitcase into the overhead compartment of a plane.
-
Balance on one leg for thirty seconds, eyes open. (Bonus points: eyes closed, fifteen seconds.)
-
Have sex.
-
Climb four flights of stairs in three minutes.
-
Open a jar.
-
Do thirty consecutive jump-rope skips.
The full list is much longer, with more than fifty different items, but you get the idea. Once they’ve read it I ask them to please select which of these tasks they want to be able to perform in their ninth, or better yet tenth, decade. Which ones do they choose?
All of them, typically. They want to be able to hike a mile and a half, or carry their own groceries, or pick up a great-grandchild, or get up if they fall down. Or play eighteen holes of golf, or open a jar, or fly somewhere on a plane. Of course they do.
That’s great, I say. You’ll make that kid’s day when you pick her up like that. But now let’s do a little math. Let’s say the kid weighs twenty-five or thirty pounds. That’s basically the same as doing a squat while holding a thirty-pound dumbbell in front of you (i.e., a goblet squat). Can you do that now, at age forty? Most likely. But now let’s look into the future. Over the next thirty or forty years, your muscle strength will decline by about 8 to 17 percent per decade—accelerating as time goes on. So if you want to pick up that thirty-pound grandkid or great-grandkid when you’re eighty, you’re going to have to be able to lift about fifty to fifty-five pounds now. Without hurting yourself. Can you do that?
I press the issue. You also want to be able to hike on a hilly trail? To do that comfortably requires a VO2 max of roughly 30 ml/kg/min. Let’s take a look at the results of your latest VO2 max test—and guess what, you only scored a 30. You’re average for your age, but I’m afraid that’s not good enough, because your VO2 max is also going to decline. So we’re going to have to go ahead and cross that hike off your list. You can pull it off now, but you likely won’t be able to do it when you’re older.
On it goes. To lift that twenty-pound suitcase overhead when you are older means doing so with forty or fifty pounds now. To be able to climb four flights of stairs in your eighties means you should be able to pretty much sprint up those same stairs today. In every case, you need to be doing much more now, to armor yourself against the natural and precipitous decline in strength and aerobic capacity that you will undergo as you age.
Eventually, my patients get it. Together, we come up with a list of ten or fifteen events in their personal Centenarian Decathlon, representing their goals for their later decades. This then determines how they should be training.
The beauty of the Centenarian Decathlon is that it is broad yet unique to each individual. Nor is it limited to ten events; for most people it ends up being more, depending on their goals. My version of the Decathlon is tailored to my own particular interests, such as swimming and archery. It’s also fairly aggressive, I admit, reflecting the importance of a high level of fitness in my life. So I would probably add in some of the following events:
-
Swim half a mile in twenty minutes.
-
Walk with a thirty-pound dumbbell in each hand for one minute.
-
Draw back and fire a fifty-pound compound bow.
-
Do five pull-ups.
-
Climb ninety steps in two minutes (VO2 max = 32).
-
Dead-hang for one minute.
-
Drive a race car within 5 to 8 percent of the pace I can do so today.
-
Hike with a twenty-pound backpack for an hour.
-
Carry my own luggage.
-
Walk up a steep hill.
In the end, most people’s Centenarian Decathlons will probably overlap to a degree. Someone who enjoys stand-up paddleboarding, for example, would perhaps choose “events” focused around building core and cross-body strength. But she will likely be training the same muscle groups as I am doing for archery, and maintaining a similar degree of stamina and balance.
The Centenarian Decathlon is ambitious, no question. A ninety-year-old who is even able to board a plane under her own power, let alone hoist a carry-on bag, is doing extremely well. But there is a method to the madness. These individual tasks are not out of reach. There are octogenarians, nonagenarians, and even centenarians right now who are running marathons, racing bicycles, lifting weights, flying airplanes, jumping out of airplanes, skiing the Rocky Mountains, competing in actual decathlons, and doing all sorts of other amazing things. So all these events are within the realm of possibility.
One purpose of the Centenarian Decathlon, in fact, is to help us redefine what is possible in our later years and wipe away the default assumption that most people will be weak and incapable at that point in their lives. We need to abolish that decrepit stereotype and create a new narrative—perhaps modeled after the old-school fitness guru Jack LaLanne, who kept doing his usual rigorous daily workout right up until his death at age ninety-six. Unlike most very long-lived individuals, he didn’t just get there by accident or luck. He built and maintained a high level of fitness throughout his life, beginning in the 1930s, when very few people exercised regularly and “fitness centers” did not yet exist. As he got older, he set out very deliberately to defy the stereotype of aging as a period of misery and decline. He did the work, and he succeeded, giving us a glimpse of what an older person is truly capable of achieving.
If we are to follow in LaLanne’s footsteps, we must stop pointlessly “exercising,” just because we think we are supposed to, banging away on the elliptical trainer at lunch hour. I promise, you can do better. I suggest you join me and start training, with a very specific purpose, which is to be kick-ass one-hundred-year-olds. When my patients say they are more interested in being kick-ass fifty-year-olds than Centenarian Decathletes, I reply that there is no better way to make that happen than to set a trajectory toward being vibrant at one hundred (or ninety, or eighty) just as an archer who trains at 100 yards will be more accurate at 50. By fixing our aim on the Centenarian Decathlon, we can make every decade between now and then better as well.
With the Centenarian Decathlon as my goal, I now work out with the focus that I once directed exclusively toward cycling, swimming, or boxing. It’s not about being great at any one pursuit, but about being pretty good at just about everything. As Centenarian Decathletes, we are no longer training for a specific event, but to become a different sort of athlete altogether: an athlete of life.