CHAPTER 7
The Ticker
Confronting—and Preventing—Heart Disease, the Deadliest Killer on the Planet
There is some risk involved in action, there always is. But there is far more risk in failure to act.
—Harry S. Truman
One downside of my profession is that too much knowledge can become its own kind of curse. As I delved back into the practice of medicine, after my hiatus in the business world, it dawned on me that I already know how I am likely to die: I seem destined to die from heart disease.
I wonder what took me so long to get the hint. When I was five, my father’s older brother Francis—his favorite of eight siblings—died of a sudden heart attack at forty-six. When my own brother Paul was born two days later, my grief-stricken father chose Francis as his middle name. Just as certain names run in families, a propensity for early cardiovascular disease seems to run in mine. Another uncle suffered a fatal heart attack at forty-two, while a third made it to age sixty-nine before his heart killed him, which is perhaps more typical but still way too young.
My dad is lucky, because he has lived to the ripe old age of eighty-five (so far). But even he has a stent in one of his coronary arteries, a souvenir of his own minor event in his midsixties. He felt chest pain one day at the limestone quarry where he worked, and ended up in the ER, where it was determined that he had had a recent infarction. The stent, a little sleeve of metal wire, was put in a year or so later. I’m not actually convinced that the stent did anything—he was not experiencing symptoms at the time it was placed—but perhaps it scared him enough to be more diligent with his medications and his diet.
So even though my cholesterol profile is excellent, and I eat sensibly, never smoke, have normal blood pressure, and rarely drink alcohol, I’m still at risk. I feel like I’m trapped in that Charlie Munger anecdote, about the guy who just wants to know where he’s going to die, so he’ll make sure never to go there. Unfortunately, too often heart disease finds you.
When I was in medical school, my first-year pathology professor liked to ask a trick question: What is the most common “presentation” (or symptom) of heart disease? It wasn’t chest pain, left arm pain, or shortness of breath, the most common answers; it was sudden death. You know the patient has heart disease because he or she has just died from it. This is why, he claimed, the only doctors who truly understand cardiovascular disease are pathologists. His point: by the time a pathologist sees your arterial tissue, you are dead.
While mortality rates from those first, surprise heart attacks have dropped significantly, thanks to improvements in basic cardiac life support and time-sensitive interventions such as cardiac catheterization and clot-obliterating drugs that can halt a heart attack almost in its tracks, they are still fatal roughly one-third of the time, according to Ron Krauss, senior scientist and director of atherosclerosis research at Children’s Hospital Oakland Research Institute.
Globally, heart disease and stroke (or cerebrovascular disease), which I lump together under the single heading of atherosclerotic cardiovascular disease, or ASCVD, represent the leading cause of death, killing an estimated 2,300 people every day in the United States, according to the CDC—more than any other cause, including cancer. It’s not just men who are at risk: American women are up to ten times more likely to die from atherosclerotic disease than from breast cancer (not a typo: one in three versus one in thirty). But pink ribbons for breast cancer far outnumber the American Heart Association’s red ribbons for awareness of heart disease among women.
My uncles’ deaths remain a mystery to me. They lived in Egypt, and I have no idea what their blood work looked like or, more importantly, what kind of shape their coronary arteries were in. I’m pretty sure they smoked, but perhaps if they had had access to better medical care they too might have survived their heart attacks, as my father did. Or perhaps their fates were inescapable, tied to their genes. All I know is that forty-two seems really young to keel over from a heart attack.
I’d known about my uncles all my life, but the implication of their stories only really hit me in my midthirties, when I became a father for the first time. All of a sudden, the awareness of my own mortality crashed over my head like a rogue wave, coming out of nowhere on one of my long swims. This book probably wouldn’t have been written if not for that family history.
Like most thirty-six-year-olds, Not-Thin Peter scarcely gave a thought to heart disease. Why should I have? My heart was strong enough to have propelled me across the twenty-one-mile-wide Catalina Channel, working steadily for more than fourteen hours, like a Mercedes diesel engine purring along smoothly inside my chest. I was in great shape, I thought. But I was nevertheless worried, on account of my family history. So I insisted that my doctor order a CT scan of my heart, and it wound up changing my whole outlook on life.
The scan was calibrated to detect calcification in my coronary arteries, a sign of advanced atherosclerosis. The results showed that I had a calcium “score” of 6. That sounds low, and in absolute terms it was; someone with severe disease could return a score well over 1,000. But for someone age thirty-six, it should have been zero. My score of 6 meant that I had more calcium in my coronary arteries than 75 to 90 percent of people my age. As I dug deeper into the pathology of this disease, I was dismayed to learn that it was already fairly late in the game. A calcium score is treated as a predictor of future risk, which it is, but it is also a measure of historical and existing damage. And I was already off the charts. I was only in my midthirties, but I had the arteries of a fifty-five-year-old.
I was upset by this revelation, although knowing what I know now, it’s not at all surprising. At the time, I was overweight and borderline insulin resistant, two huge risk factors that by themselves help create an environment that fosters and accelerates the development of atherosclerotic lesions. Yet because my calcium score was “only” 6, and my all-important LDL (“bad”) cholesterol was “normal,” the medical advice I received was—wait for it—to do nothing. Sound familiar?
Doing nothing is not my style, as you may have gathered by now. I sensed that I was not on a good trajectory, and I needed to figure out how to change it. My curiosity launched me on a years-long quest to truly understand atherosclerosis. The story I uncovered, with the generous help of my mentors Tom Dayspring, Allan Sniderman, and Ron Krauss (among others), all of whom are world-renowned experts in cardiac pathology and/or the study of lipids, was flabbergasting.
While heart disease is the most prevalent age-related condition, it is also more easily prevented than either cancer or Alzheimer’s disease. We know a lot about how and why it begins and the manner in which it progresses. While it can’t exactly be cured or reversed the way type 2 diabetes (sometimes) can, it is relatively easy to delay if you’re smart and you get on the case early. It’s also the rare example of a chronic disease where Medicine 2.0 already does focus on prevention, to some extent. We have a cabinet full of blood pressure–and cholesterol–lowering medications that really do reduce the risk of death for many patients, and we have blood tests and imaging tests (like my calcium scan) that can at least give us a snapshot, however blurry, of someone’s cardiovascular health. It’s a start.
In spite of how well we understand atherosclerotic disease and its progression, and how many tools we have to prevent it, it still kills more people than cancer in the United States each year, many of them completely out of the blue. We’re losing the war. I don’t claim to have all the answers, but I think this is at least partly due to the fact that we still have some major blind spots in our understanding of what truly drives our risk for the disease, how it develops, and most of all when we need to act to counter its momentum.
The fundamental problem, I believe, is classic Medicine 2.0: guidelines for managing cardiovascular risk are based on an overly short time horizon, compared to the time line of the disease. We need to begin treating it, and preventing it, much earlier. If we could get it right, the potential payoff would be huge: the high prevalence of male centenarians on the island of Sardinia, for example, has largely been attributed to their ability to avoid or delay circulatory disease. Fewer Sardinian men die from heart disease between the ages of eighty and one hundred than anywhere else in Italy.
But we’re nowhere near that. Heart disease remains our deadliest killer, the worst of the Horsemen. In the next few pages, I hope to convince you that it need not be—that with the right strategy, and attention to the correct risk factors at the correct time, it should be possible to eliminate much of the morbidity and mortality that is still associated with atherosclerotic cardiovascular and cerebrovascular disease.
Bluntly put: this should be the tenth leading cause of death, not the first.
Scientists have been exploring the medical mysteries of the human heart for almost as long as poets have been probing its metaphorical depths. It is a wondrous organ, a tireless muscle that pumps blood around the body every moment of our lives. It pounds hard when we are exercising, slows down when we sleep, and even microadjusts its rate between beats, a hugely important phenomenon called heart rate variability. And when it stops, we stop.
Our vascular network is equally miraculous, a web of veins, arteries, and capillaries that, if stretched out and laid end to end, would wrap around the earth more than twice (about sixty thousand miles, if you’re keeping score). Each individual blood vessel is a marvel of material science and engineering, capable of expanding and contracting dozens of times per minute, allowing vital substances to pass through its membranes, and accommodating huge swings in fluid pressure, with minimal fatigue. No material created by man can even come close to matching this. If one vessel is injured, others regrow to take its place, ensuring continuous blood flow throughout the body.
Incredible as it is, however, our circulatory system is far from perfect—in fact, it is almost perfectly designed to generate atherosclerotic disease, just in the course of daily living. This is in large part because of another important function of our vasculature. In addition to transporting oxygen and nutrients to our tissues and carrying away waste, our blood traffics cholesterol molecules between cells.
It’s practically a dirty word, cholesterol. Your doctor will probably utter it with a frown, because as everyone knows, cholesterol is evil stuff. Well, some of it is—you know, the LDL or “bad” cholesterol, which is inevitably counterpoised against the HDL, or “good” cholesterol. I practically need to be restrained when I hear these terms, because they’re so meaningless. And your “total cholesterol,” the first number that people offer up when we’re talking about heart disease, is only slightly more relevant to your cardiovascular risk than the color of your eyes. So let’s hit rewind and look at what cholesterol really is, what it does, and how it contributes to heart disease.
Cholesterol is essential to life. It is required to produce some of the most important structures in the body, including cell membranes; hormones such as testosterone, progesterone, estrogen, and cortisol; and bile acids, which are necessary for digesting food. All cells can synthesize their own cholesterol, but some 20 percent of our body’s (large) supply is found in the liver, which acts as a sort of cholesterol repository, shipping it out to cells that need it and receiving it back via the circulation.
Because cholesterol belongs to the lipid family (that is, fats), it is not water soluble and thus cannot dissolve in our plasma like glucose or sodium and travel freely through our circulation. So it must be carted around in tiny spherical particles called lipoproteins—the final “L” in LDL and HDL—which act like little cargo submarines. As their name suggests, these lipoproteins are part lipid (inside) and part protein (outside); the protein is essentially the vessel that allows them to travel in our plasma while carrying their water-insoluble cargo of lipids, including cholesterol, triglycerides, and phospholipids, plus vitamins and other proteins that need to be distributed to our distant tissues.
The reason they’re called high- and low-density lipoproteins (HDL and LDL, respectively) has to do with the amount of fat relative to protein that each one carries. LDLs carry more lipids, while HDLs carry more protein in relation to fat, and are therefore more dense. Also, these particles (and other lipoproteins) frequently exchange cargo with one another, which is part of what drives me crazy about labeling them “good” and “bad.” When an HDL transfers its “good cholesterol” to an LDL particle, does that cholesterol suddenly become “bad”?
The answer is no—because it’s not the cholesterol per se that causes problems but the nature of the particle in which it’s transported. Each lipoprotein particle is enwrapped by one or more large molecules, called apolipoproteins, that provide structure, stability, and, most importantly solubility to the particle. HDL particles are wrapped in a type of molecule called apolipoprotein A (or apoA), while LDL is encased in apolipoprotein B (or apoB). This distinction may seem trivial, but it goes to the very root cause of atherosclerotic disease: every single lipoprotein that contributes to atherosclerosis—not only LDL but several others[*1]—carries this apoB protein signature.
Another major misconception about heart disease is that it is somehow caused by the cholesterol that we eat in our diet. According to this dated and simplistic view, eating cholesterol-rich foods causes the so-called bad cholesterol to accumulate in our blood and then build up on our artery walls, as if you poured bacon grease down the kitchen drain every time you made breakfast. Sooner or later, your sink will back up.
The humble egg, in particular, was singled out in a 1968 proclamation by the American Heart Association, accused of causing heart disease because of its high cholesterol content. It has remained in nutritional purgatory for decades, even after reams of research papers showing that dietary cholesterol (and particularly egg consumption) may not have much to do with heart disease at all. Eating lots of saturated fat can increase levels of atherosclerosis-causing lipoproteins in blood, but most of the actual cholesterol that we consume in our food ends up being excreted out our backsides. The vast majority of the cholesterol in our circulation is actually produced by our own cells. Nevertheless, US dietary guidelines warned Americans away from consuming foods high in cholesterol for decades, and nutrition labels still inform American consumers about how much cholesterol is contained in each serving of packaged foods.
Even Ancel Keys, the famed nutrition scientist who was one of the founding fathers of the notion that saturated fat causes heart disease, knew this was nonsense. The problem he recognized was that much of the basic research into cholesterol and atherosclerosis had been conducted in rabbits, which have a unique ability to absorb cholesterol into their blood from their food and form atherosclerotic plaques from it; the mistake was to assume that humans also absorb dietary cholesterol as readily. “There’s no connection whatsoever between cholesterol in food and cholesterol in blood,” Keys said in a 1997 interview. “None. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.”
It took nearly two more decades before the advisory committee responsible for the US government dietary guidelines finally conceded (in 2015) that “cholesterol is not a nutrient of concern for overconsumption.” Glad we settled that.
The final myth that we need to confront is the notion that cardiovascular disease primarily strikes “old” people and that therefore we don’t need to worry much about prevention in patients who are in their twenties and thirties and forties. Not true. I’ll never forget the one-question pop quiz that Allan Sniderman dropped on me over dinner at Dulles Airport, back in 2014: “What proportion of heart attacks occur in people younger than age sixty-five?” I guessed high, one in four, but I was way low. Fully half of all major adverse cardiovascular events in men (and a third of those in women), such as heart attack, stroke, or any procedure involving a stent or a graft, occur before the age of sixty-five. In men, one-quarter of all events occur before age fifty-four.
But while the events themselves may have seemed sudden, the problem was likely lurking for years. Atherosclerosis is a slow-moving, sneaky disease, which is why I take such a hard line on it. Our risk of these “events” rises steeply in the second half of our lifespan, but some scientists believe the underlying processes are set into motion in late adolescence, even as early as our teens. The risk builds throughout our lives, and the critical factor is time. Therefore it is critical that we understand how it develops, and progresses, so we can develop a strategy to try to slow or stop it.
Back when I had an office, pre-COVID, I kept a clutter-free desk, but one book in particular was always there: Atlas of Atherosclerosis Progression and Regression, by Herbert C. Stary. It will never be a bestseller, but in the field of cardiovascular pathology it is legendary. It also happens to be a highly effective tool for communicating the seriousness of this disease to my patients, thanks to its lavish and gruesome photographs of arterial lesions as they form, develop, and rupture—all taken of the arteries of dead people, many of them in their twenties and thirties. The story it lays out, in graphic detail, is equal parts fascinating and terrifying. By the time I finished, my patients would often have this kind of harrowed expression on their faces, as if they’d just leafed through a coffee-table book documenting their own death.
This isn’t a perfect analogy, but I think of atherosclerosis as kind of like the scene of a crime—breaking and entering, more or less. Let’s say we have a street, which represents the blood vessel, and the street is lined with houses, representing the arterial wall. The fence in front of each house is analogous to something called the endothelium, a delicate but critical layer of tissue that lines all our arteries and veins, as well as certain other tissues, such as the kidneys. Composed of just a single layer of cells, the endothelium acts as a semipermeable barrier between the vessel lumen (i.e., the street, where the blood flows) and the arterial wall proper, controlling the passage of materials and nutrients and white blood cells into and out of the bloodstream. It also helps maintain our electrolyte and fluid balance; endothelial problems can lead to edema and swelling. Another very important job it does is to dilate and contract to allow increased or decreased blood flow, a process modulated by nitric oxide. Last, the endothelium regulates blood-clotting mechanisms, which can be important if you accidentally cut yourself. It’s a pretty important little structure.
The street is very busy, with a constant flow of blood cells and lipoproteins and plasma and everything else that our circulation carries, all brushing past the endothelium. Inevitably, some of these cholesterol-bearing lipoprotein particles will penetrate the barrier, into an area called the subendothelial space—or in our analogy, the front porch. Normally, this is fine, like guests stopping by for a visit. They enter, and then they leave. This is what HDL particles generally do: particles tagged with apoA (HDL) can cross the endothelial barrier easily in both directions, in and out. LDL particles and other particles with the apoB protein are far more prone to getting stuck inside.
This is what actually makes HDL particles potentially “good” and LDL particles potentially “bad”—not the cholesterol, but the particles that carry it. The trouble starts when LDL particles stick in the arterial wall and subsequently become oxidized, meaning the cholesterol (and phospholipid) molecules they contain come into contact with a highly reactive molecule known as a reactive oxygen species, or ROS, the cause of oxidative stress. It’s the oxidation of the lipids on the LDL that kicks off the entire atherosclerotic cascade.
Now that it is lodged in the subendothelial space and oxidized, rendering it somewhat toxic, the LDL/apoB particle stops behaving like a polite guest, refusing to leave—and inviting its friends, other LDLs, to join the party. Many of these also are retained and oxidized. It is not an accident that the two biggest risk factors for heart disease, smoking and high blood pressure, cause damage to the endothelium. Smoking damages it chemically, while high blood pressure does so mechanically, but the end result is endothelial harm that, in turn, leads to greater retention of LDL. As oxidized LDL accumulates, it causes still more damage to the endothelium.
I’ve been saying LDL, but the key factor here is actually exposure to apoB-tagged particles, over time. The more of these particles that you have in your circulation, not only LDL but VLDL and some others, the greater the risk that some of them will penetrate the endothelium and get stuck. Going back to our street analogy, imagine that we have, say, one ton of cholesterol moving down the street, divided among four pickup trucks. The chance of an accident is fairly small. But if that same total amount of cholesterol is being carried on five hundred of those little rental scooters that swarm around cities like Austin, where I live, we are going to have absolute mayhem[*2] on our hands. So to gauge the true extent of your risk, we have to know how many of these apoB particles are circulating in your bloodstream. That number is much more relevant than the total quantity of cholesterol that these particles are carrying.
If you take a healthy coronary artery and expose it to high enough concentrations of apoB particles, over a long enough time, a certain amount of LDL (and VLDL) will get stuck in that subendothelial space and become oxidized, which then leads to it sticking together in clumps or aggregates. In response to this incursion, the endothelium dials up the biochemical equivalent of 911, summoning specialized immune cells called monocytes to the scene to confront the intruders. Monocytes are large white blood cells that enter the subendothelial space and transform into macrophages, larger and hungrier immune cells that are sometimes compared to Pac-Man. The macrophage, whose name means “big eater,” swallows up the aggregated or oxidized LDL, trying to remove it from the artery wall. But if it consumes too much cholesterol, then it blows up into a foam cell, a term that you may have heard—so named because under a microscope it looks foamy or soapy. When enough foam cells gather together, they form a “fatty streak”—literally a streak of fat that you can see with your naked eye during an autopsy of a splayed-open coronary artery.
The fatty streak is a precursor of an atherosclerotic plaque, and if you are reading this and are older than fifteen or so, there is a good chance you already have some of these lurking in your arteries. Yes, I said “fifteen” and not “fifty”—this is a lifelong process and it starts very early. Autopsy data from young people who died from accidents, homicides, or other noncardiovascular causes have revealed that as many as a third of sixteen- to twenty-year-olds already had actual atherosclerotic lesions or plaques in their coronary arteries when they died. As teenagers.
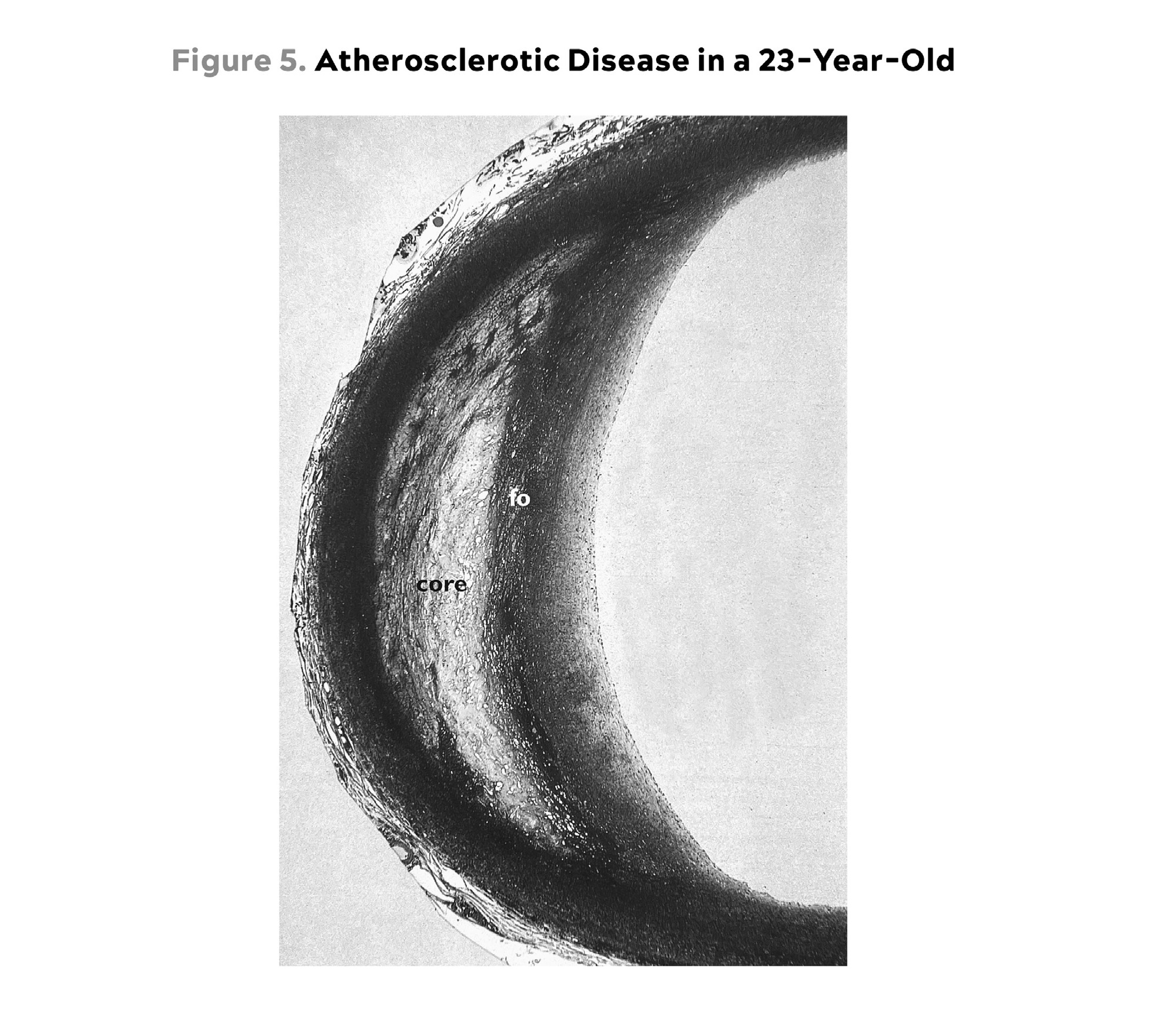
Source: Stary, (2003).
This is a cross-sectional view of the proximal left anterior descending artery, one of the key vessels supplying blood to the heart, from a twenty-three-year-old male homicide victim. Note that he already has extensive atherosclerotic damage in the wall of this artery: a significant core (“core”) of accumulated lipids, and macrophages and foam cells (“fo”) in the subendothelial space, beginning to encroach on the lumen, the passage where blood flows. He would likely not suffer a heart attack anytime soon, but this is very advanced disease nonetheless.
It’s not as if they were about to have heart attacks. The atherosclerotic process moves very slowly. This may be partly because of the action of HDLs. If an HDL particle arrives at our crime scene, with the foam cells and fatty streaks, it can suck the cholesterol back out of the macrophages in a process called delipidation. It then slips back across the endothelial layer and into the bloodstream, to deliver the excess cholesterol back to the liver and other tissues (including fat cells and hormone-producing glands) for reuse.
Its role in this process of “cholesterol efflux” is one reason why HDL is considered “good,” but it does more than that. Newer research suggests that HDL has multiple other atheroprotective functions that include helping maintain the integrity of the endothelium, lowering inflammation, and neutralizing or stopping the oxidation of LDL, like a kind of arterial antioxidant.
The role of HDL is far less well understood than that of LDL. The cholesterol content in your LDL particles, your “bad” cholesterol number (technically expressed as LDL-C),[*3] is actually a decent if imperfect proxy for its biologic impact; lots of studies have shown a strong correlation between LDL-C and event risk. But the all-important “good cholesterol” number on your blood test, your HDL-C, doesn’t actually tell me very much if anything about your overall risk profile. Risk does seem to decline as HDL-C rises to around the 80th percentile. But simply raising HDL cholesterol concentrations by brute force, with specialized drugs, has not been shown to reduce cardiovascular risk at all. The key seems to be to increase the functionality of the particles—but as yet we have no way to do that (or measure it).
HDL may or may not explain why centenarians develop heart disease two decades later than average, if at all; remember, three of the most prominent “longevity genes” discovered to date are involved with cholesterol transport and processing (APOE and two others, CETP and APOC3). And it’s not just centenarians: I have patients walking around whose lipoprotein panels read like a death sentence, with sky-high LDL-C and apoB, but by every single measure that we have—calcium score, CT angiogram, you name it—they show no sign of disease. Yet as of now, we cannot give a satisfactory explanation for why. I feel strongly that if we are to make any further progress attacking cardiovascular disease with drugs, we must start by better understanding HDL and hopefully figuring out how to enhance its function.
But I digress. Back at the crime scene, the ever-growing number of foam cells begin to sort of ooze together into a mass of lipids, like the liquefying contents of a pile of trash bags that have been dumped on the front lawn. This is what becomes the core of our atherosclerotic plaque. And this is the point where breaking and entering tilts over into full-scale looting. In an attempt to control the damage, the “smooth muscle” cells in the artery wall then migrate to this toxic waste site and secrete a kind of matrix in an attempt to build a kind of barrier around it, like a scar. This matrix ends up as the fibrous cap on your brand-new arterial plaque.
More bad news: None of what’s gone on so far is easily detectable in the various tests we typically use to assess cardiovascular risk in patients. We might expect to see evidence of inflammation, such as elevated levels of C-reactive protein, a popular (but poor) proxy of arterial inflammation. But it’s still mostly flying below our medical radar. If you look at the coronary arteries with a CT scan at this very early stage, you will likely miss this if you’re looking only for calcium buildup. (You have a better chance of spotting this level of damage if using a more advanced type of CT scan, called a CT angiogram, which I much prefer to a garden-variety calcium scan[*4] because it can also identify the noncalcified or “soft” plaque that precedes calcification.)
As this maladaptive repair or remodeling process continues, the plaque will continue to grow. At first, this expansion is directed toward the outer arterial wall, but as it continues it may encroach on the lumen, the passage through which blood flows—in our analogy, blocking traffic in the street itself. This luminal narrowing, known as stenosis, can also be seen in an angiogram.
At a certain point in this process, the plaque may start to become calcified. This is what (finally) shows up on a regular calcium scan. Calcification is merely another way in which the body is trying to repair the damage, by stabilizing the plaque to protect the all-important arteries. But it’s like pouring concrete on the Chernobyl reactor: you’re glad it’s there, but you know there’s been an awful lot of damage in the area to warrant such an intervention. A positive calcium score is really telling us that there are almost certainly other plaques around that may or may not be stabilized (calcified).
If the plaque does become unstable, eroding or even rupturing, you’ve really got problems. The damaged plaque may ultimately cause the formation of a clot, which can narrow and ultimately block the lumen of the blood vessel—or worse, break free and cause a heart attack or stroke. This is why we worry more about the noncalcified plaques than the calcified ones.
Normally, however, most atherosclerotic plaques are fairly undramatic. They grow silently and invisibly, gradually occluding the blood vessel until one day the obstruction, due to the plaque itself or a plaque-induced clot, becomes a problem. For example, a sedentary person may not notice that she has a partially blocked coronary artery until she goes outside to shovel snow. The sudden demands on her circulatory system can trigger ischemia (decreased blood delivery of oxygen) or infarction (tissue death from no blood flow)—or, in layman’s terms, a heart attack or a stroke.
It may seem sudden, but the danger was lurking all along.
When I finally recognized my own cardiovascular risk, back in my thirties, I had no idea about how any of this complex disease process worked. Looking back, it’s clear that I had quite a few of the major and lesser risk factors already checked off. I didn’t smoke, which is perhaps the most potent environmental risk driver, and my blood pressure was normal, but I had other problems. And as my calcium score revealed, I already had a small, calcified plaque in the upper part of my left anterior descending (LAD) artery, one of the main arteries supplying my heart. There may have been other bad things happening there as well, but because I did not have a CT angiogram at this time, I had no sense of what kind of damage existed elsewhere in my coronary arteries. Anything shy of calcification is not identified by the calcium score.
Clearly, Not-Thin Peter was already on the road to heart disease. My waist size was on track to hit 40 by the time I turned forty, a clear sign of my metabolic dysfunction. Underneath my belt, I was likely accumulating visceral fat. I was also insulin resistant, an enormous risk driver for cardiovascular disease. Though my blood pressure was fine, I suspect it would have deteriorated fairly rapidly as I aged, as hypertension seems rampant in my family. I probably also had high levels of uric acid, which as we saw in the previous chapter is often found in the company of high blood pressure and other signs of metabolic dysfunction. All of these contribute to another necessary (but not sufficient) condition that is required for atherosclerosis to develop, and that is inflammation. The endothelial barrier, in particular, is uniquely vulnerable to damage from inflammation.
But no physician would likely have treated me for any of this. My blood panel did not signal any significant risk. My LDL-C tested at 110 to 120 mg/dL, just slightly higher than normal but not a cause for concern, particularly in a younger person. My triglycerides were on the higher side, slightly north of 150 mg/dL, but that did not set off any alarm bells either. I now know that these numbers almost certainly indicated a high concentration of atherogenic apoB particles—but no one bothered to test my apoB number, either.
Back then, nearly fifteen years ago, the apoB test (simply, measuring the concentration of apoB-tagged particles) was not commonly done. Since then, evidence has piled up pointing to apoB as far more predictive of cardiovascular disease than simply LDL-C, the standard “bad cholesterol” measure. According to an analysis published in JAMA Cardiology in 2021, each standard-deviation increase in apoB raises the risk of myocardial infarction by 38 percent in patients without a history of cardiac events or a diagnosis of cardiovascular disease (i.e., primary prevention). That’s a powerful correlation. Yet even now, the American Heart Association guidelines still favor LDL-C testing instead of apoB. I have all my patients tested for apoB regularly, and you should ask for the same test the next time you see your doctor. (Don’t be waved off by nonsensical arguments about “cost”: It’s about twenty to thirty dollars.)
I was still in my thirties, yet I likely already had all three of the major prerequisites for heart disease: significant lipoprotein burden or apoB, LDL oxidation or modification (leading to the plaques that my calcium scan revealed), and a high level of background inflammation. None of these is enough to guarantee that someone will develop heart disease, but all three are necessary to develop it. We are fortunate that many of these conditions can be modulated or nearly eliminated—including apoB, by the way—via lifestyle changes and medications. As we’ll discuss in the final section, I take a very hard line on lowering apoB, the particle that causes all this trouble. (In short: get it as low as possible, as early as possible.)
But before we go there, I want to talk about another deadly but relatively little-known lipoprotein that is likely responsible for graveyards full of sudden cardiac arrest victims, people whose conventional cholesterol panels and risk factor profiles otherwise looked fine. I don’t have this particular issue, thankfully, but a very good friend of mine does, and finding out about it in a timely manner likely saved his life.
I met Anahad O’Connor in 2012 on a junket to France, courtesy of the French-American Foundation and an award we had both won, and we immediately bonded. I think it was because we were the only two guys on the trip who skipped the pain au chocolat and spent our spare time in the gym. Also, he wrote about health and science for The New York Times, so we had plenty to talk about.
Because I am a cholesterol nerd, I badgered Anahad into doing a comprehensive lipoprotein panel when we got back to the United States. He looked at me funny—Why should he do that? He was only in his early thirties, an extremely fit vegetarian with maybe 6 or 7 percent body fat. He should have been fine in the lipid department. But you never know; his father had died of an aneurysm, which may have been a sign of circulatory problems.
As expected, his standard lipid numbers looked great. There was only one thing that seemed off, so I suggested that he should probably also get a calcium scan, as I had done, so we could get a better sense of the state of his arteries. That’s where things got interesting. Recall, my calcium score had come back at 6, placing me at higher risk than 75 to 90 percent of people my age. Anahad’s calcium score was 125—off the charts for someone so young and otherwise healthy. “Can this be real?” he said.
It was. It turned out that the culprit was a little-known but very deadly type of particle called Lp(a) (pronounced “el-pee-little-A”). This hot mess of a lipoprotein is formed when a garden-variety LDL particle is fused with another, rarer type of protein called apolipoprotein(a), or apo(a) for short (not to be confused with apolipoprotein A or apoA, the protein that marks HDL particles). The apo(a) wraps loosely around the LDL particle, with multiple looping amino acid segments called “kringles,” so named because their structure resembles the ring-shaped Danish pastry by that name. The kringles are what make Lp(a) so dangerous: as the LDL particle passes through the bloodstream, they scoop up bits of oxidized lipid molecules and carry them along.
As my lipid guru Tom Dayspring points out, this isn’t entirely bad. There is some evidence that Lp(a) may act as a sort of cleansing agent, like a street-sweeping truck that gathers up unpleasant and potentially harmful lipid junk and delivers it to the liver. But because Lp(a) is a member of the apoB particle family, it also has the potential to penetrate the endothelium and get lodged in an artery wall; because of its structure, Lp(a) may be even more likely than a normal LDL particle to get stuck, with its extra cargo of lipids gone bad. Even worse, once in there, it acts partly as a thrombotic or proclotting factor, which helps to speed the formation of arterial plaques.
Often, the way Lp(a) announces itself is via a sudden, seemingly premature heart attack. This is what happened to Biggest Loser host Bob Harper, who suffered cardiac arrest at a gym in New York in 2017, at age fifty-two. Harper’s life was saved by a bystander who performed CPR until the paramedics arrived. He woke up in the hospital two days later, wondering what had hit him. Turns out, his very high level of Lp(a) was what had hit him. He had no idea that he was at risk.
This is not an atypical scenario: when a patient comes to me and says their father or grandfather or aunt, or all three, died of “premature” heart disease, elevated Lp(a) is the first thing I look for. It is the most prevalent hereditary risk factor for heart disease, and its danger is amplified by the fact that it is still largely flying under the radar of Medicine 2.0, although that is beginning to change.
Most people have relatively small concentrations of this particle, but some individuals can have as much as one hundred times more than others. The variation is largely genetic, and an estimated 20 to 30 percent of the US population has levels high enough that they are at increased risk; also, people of African descent tend to have higher levels of Lp(a), on average, than Caucasians. This is why, if you have a history of premature heart attacks in your family, you should definitely ask for an Lp(a) test. We test every single patient for Lp(a) during their first blood draw. Because elevated Lp(a) is largely genetic, the test need only be done once (and cardiovascular disease guidelines are beginning to advise a once-a-lifetime test for it anyway).
Anahad was fortunate that he found out about his situation when he did. His calcium score meant that he had already suffered significant atherosclerotic damage due to his Lp(a). Beyond the harm it causes to coronary arteries, Lp(a) is particularly destructive to the aortic valve, one of the more important structures in the heart, by promoting the formation of tiny, bony particles in the valve leaflets, which leads to stenosis or narrowing of the aortic outlet.
There was no quick fix for Anahad, or anyone else with elevated Lp(a). It does not seem to respond to behavioral interventions such as exercise and dietary changes the way that, say, LDL-C does. A class of drug called PCSK9 inhibitors, aimed at lowering apoB concentrations, does seem to be able to reduce Lp(a) levels by approximately 30 percent, but as yet there are no data suggesting that they reduce the excess events (heart attacks) attributable to that particle. Thus, the only real treatment for elevated Lp(a) right now is aggressive management of apoB overall. Though we can’t reduce Lp(a) directly, beyond what a PCSK9 inhibitor can do, we can lower the remaining apoB concentration sufficiently that we can reduce a patient’s overall risk.[*5] Because Anahad is relatively young, he also has more time to address his other risk factors.
Luckily, we found the trouble before the trouble found him.
How to Reduce Cardiovascular Risk
In a way, Not-Thin Peter and Anahad O’Connor were like two sides of the same coin. While our stories don’t seem to have much in common, both underscore the insidious, almost sneaky nature of heart disease: my risk should have been obvious, based on my family history, while Anahad’s disease remained all but invisible until he happened to have a calcium scan, which is not normally done on healthy-seeming people in their thirties. We only learned of our risk thanks to dumb luck, because few doctors would have considered screening either of us for heart disease at our ages.
Together, our stories illustrate three blind spots of Medicine 2.0 when it comes to dealing with atherosclerotic disease: first, an overly simplistic view of lipids that fails to understand the importance of total lipoprotein burden (apoB) and how much one needs to reduce it in order to truly reduce risk; second, a general lack of knowledge about other bad actors such as Lp(a); and third, a failure to fully grasp the lengthy time course of atherosclerotic disease, and the implications this carries if we seek true prevention.
When I look at a patient’s blood panel for the first time, my eyes immediately dart to two numbers: apoB and Lp(a). I look at the other numbers, too, but these two tell me the most when it comes to predicting their risk of ASCVD. ApoB not only tells me the concentration of LDL particles (which, you’ll recall, is more predictive of disease than the concentration of cholesterol found within LDL particles, LDL-C), but it also captures the concentration of VLDL particles, which as members of the apoB family can also contribute to atherosclerosis. Furthermore, even someone whose apoB is low can still have a dangerously elevated Lp(a).[*6]
Once you establish the central importance of apoB, the next question becomes, By how much does one need to lower it (or its proxy LDL-C) to achieve meaningful risk reduction? The various treatment guidelines specify target ranges for LDL-C, typically 100 mg/dL for patients at normal risk, or 70 mg/dL for high-risk individuals. In my view, this is still far too high. Simply put, I think you can’t lower apoB and LDL-C too much, provided there are no side effects from treatment. You want it as low as possible.
As Peter Libby, one of the leading authorities on cardiovascular disease, and colleagues wrote in Nature Reviews in 2019, “Atherosclerosis probably would not occur [emphasis mine] in the absence of LDL-C concentrations in excess of physiological needs (on the order of 10 to 20 mg/dL).” Furthermore, the authors wrote: “If the entire population maintained LDL concentrations akin to those of a neonate (or to those of adults of most other animal species), atherosclerosis might well be an orphan disease.”
Translation: if we all maintained the apoB levels we had when we were babies, there wouldn’t be enough heart disease on the planet for people to know what it was. Kind of like 3-hydroxyisobutyric aciduria. What, you haven’t heard of it? Well, that’s because there have been only thirteen reported cases. Ever. That is an orphan disease. I’m being a bit facetious, but my point is that atherosclerotic disease shouldn’t even be in the top ten causes of death, if we treated it more aggressively. Instead, we have over eighteen million cases of fatal atherosclerotic disease per year globally.
Many doctors, and in fact many of you reading this, might be shocked to see such a low LDL-C target: 10 to 20 mg/dL? Most guidelines consider lowering LDL-C to 70 mg/dL to be “aggressive,” even for secondary prevention in high-risk patients, such as those who have already had a heart attack. It’s also natural to ask whether such extremely low levels of LDL-C and apoB are safe, given the ubiquity and importance of cholesterol in the human body. But consider the following: infants, who presumably require the most cholesterol, in order to meet the enormous demands of their rapidly growing central nervous system, have similarly low levels of circulating cholesterol, without any developmental impairment. Why? Because the total amount of cholesterol contained in all our lipoproteins—not just LDL, but also HDL and VLDL—represents only about 10 to 15 percent of our body’s total pool of cholesterol. So the concern is unwarranted, as demonstrated by scores of studies showing no ill effects from extremely low LDL concentrations.
This is my starting point with any patient, whether they are like Anahad (with one prominent risk factor) or like me (lots of smaller risk factors). Our first order of business is to reduce the burden of apoB particles, primarily LDLs but also VLDLs, which can be dangerous in their own right. And do so dramatically, not marginally or incrementally. We want it as low as possible, sooner rather than later. We must also pay attention to other markers of risk, notably those associated with metabolic health, such as insulin, visceral fat, and homocysteine, an amino acid that in high concentrations[*7] is strongly associated with increased risk of heart attack, stroke, and dementia.
You’ll note that I don’t pay much attention to HDL-C, because while having very low HDL-C is associated with higher risk, it does not appear to be causal. This is why drugs aimed at raising HDL-C have generally failed to reduce risk and events in clinical trials. The reasons why are suggested by two elegant Mendelian randomization studies that examined both sides of the HDL-C question: Does low HDL-C causally increase the risk of myocardial infarction? No. Does raising HDL-C causally lower the risk of myocardial infarction? No.
Why? Probably because whatever benefit HDLs provide in the battle for arterial supremacy, it (again) seems to be driven by their function—which doesn’t seem to be related to their cholesterol content. But we cannot test for HDL functionality, and until we have a better grasp on how HDL actually works, it will likely remain elusive as a target of therapy.
Lipoproteins aren’t the only significant risk factors for cardiovascular disease; as noted earlier, smoking and high blood pressure both damage the endothelium directly. Smoking cessation and blood pressure control are thus non-negotiable first steps in reducing cardiovascular risk.
We’ll talk about nutrition in much more detail, but my first step in controlling my own cardiovascular risk was to begin to change my own diet, so as to lower my triglycerides (a contributor to apoB when they are high, as mine were), but more importantly to manage my insulin levels. I needed to get my metabolic house in order. I should note that my own solution at the time, a ketogenic diet, might not work for everyone, nor is it a diet to which I continue to adhere. In my clinical experience, about a third to half of people who consume high amounts of saturated fats (which sometimes goes hand in hand with a ketogenic diet) will experience a dramatic increase in apoB particles, which we obviously don’t want.[*8] Monounsaturated fats, found in high quantities in extra virgin olive oil, macadamia nuts, and avocados (among other foods), do not have this effect, so I tend to push my patients to consume more of these, up to about 60 percent of total fat intake. The point is not necessarily to limit fat overall but to shift to fats that promote a better lipid profile.
But for many patients, if not for most, lowering apoB to the levels we aim for—the physiologic levels found in children—cannot be accomplished with diet alone, so we need to use nutritional interventions in tandem with drugs. Here we are fortunate because we have more preventive options in our armamentarium than we do for cancer or neurodegenerative disease. Statins are far and away the most prescribed class of drugs for lipid management, but there are several other options that might be right for a given individual, and often we need to combine classes of drugs, so it’s not uncommon for a patient to take two lipid-lowering drugs that operate via distinct mechanisms. These are typically thought of as “cholesterol-lowering” medications, but I think we are better served to think about them in terms of increasing apoB clearance, enhancing the body’s ability to get apoBs out of circulation. That’s really our goal. Mostly this is done by amplifying the activity of LDL receptors (LDLR) in the liver, which absorb cholesterol from the bloodstream.
Different drugs arrive at this effect via different paths. Typically our first line of defense (or attack), statins inhibit cholesterol synthesis, prompting the liver to increase the expression of LDLR, taking more LDL out of circulation. They may have other benefits too, including an apparent anti-inflammatory effect, so while I don’t think statins should be dissolved into the drinking water, as some have suggested, I do think they are very helpful drugs for reducing apoB or LDL concentration in many patients. Not everyone can take statins comfortably; about 5 percent of patients experience deal-breaking side effects, most notably statin-related muscle pain. Also, a smaller but nonzero subset of patients taking statins experience a disruption in glucose homeostasis, which may explain why statins are associated with a small increase in the risk for type 2 diabetes. Another fraction of patients experience an asymptomatic rise in liver enzymes, which is even more common in patients also taking the drug ezetimibe. All these side effects are completely and rapidly reversible when the drug is discontinued. But for those who can tolerate them (i.e., most people), I deploy them early and often. (For more on specific statin and other apoB-lowering medications, see the sidebar on this page.)
This brings us to the final, and perhaps greatest, major blind spot of Medicine 2.0: time.
The process I’ve outlined in this chapter unfolds very slowly—not over two or three or even five years, but over many decades. The fact that younger people have been found to have lesions and plaques, without suffering many events, tells us that there is a considerable period of time when the disease is not harmful. Dying from cardiovascular disease is certainly not inevitable: the centenarians delay it for decades, and many avoid it altogether, their arteries remaining as clean as those of people a generation younger. Somehow, they manage to slow the process down.
Nearly all adults are coping with some degree of vascular damage, no matter how young and vital they may seem, or how pristine their arteries appear on scans. There is always damage, especially in regions of shear stress and elevated local blood pressure, such as curves and splits in the vasculature. Atherosclerosis is with us, in some form, throughout our life course. Yet most doctors consider it “overtreatment” to intervene if a patient’s computed ten-year risk of a major adverse cardiac event (e.g., heart attack or stroke) is below 5 percent, arguing that the benefits are not greater than the risks, or that treatment costs too much. In my opinion, this betrays a broader ignorance about the inexorable, long-term unfolding of heart disease. Ten years is far too short a time horizon. If we want to reduce deaths from cardiovascular disease, we need to begin thinking about prevention in people in their forties and even thirties.
Another way to think of all this is that someone might be considered “low risk” at a given point—but on what time horizon? The standard is ten years. But what if our time horizon is “the rest of your life”?
Then nobody is at low risk.
When I had my first calcium scan in 2009, at the age of thirty-six, my ten-year risk was incalculably low—literally. The dominant mathematical models for risk assessment have a lower limit for age of forty or forty-five. My parameters could not even be entered into the models. So it’s no wonder nobody was alarmed by my findings. Despite my calcium score of 6, my ten-year risk of a heart attack was far less than 5 percent.
In 2016, seven years after my initial calcium scan, I had a CT angiogram (the better, higher-res scan), which showed the same small speck of calcium but no evidence of additional soft plaque elsewhere. In 2022, I went back again for a repeat CT angiogram, and the result was the same. There was no indication whatsoever of soft plaque this time either, and only that tiny speck of calcium remained from 2009.[*9] Thus, at least at the resolution of the sharpest CT scanner commercially available, there is no reason to believe that my atherosclerosis has progressed over thirteen years.
I have no idea if this means I’m free from risk—I frankly doubt it—but I no longer fear dying from cardiovascular disease the way I once did. My long, comprehensive program of prevention seems to have paid off. I feel a lot better now, at age fifty, than I did at age thirty-six, and my risk is a lot lower by any metric other than age. One major reason for this is that I started early, well before Medicine 2.0 would have suggested any intervention.
Yet most physicians and cardiology experts would still insist that one’s thirties are too young to begin to focus on primary prevention of cardiac disease. This viewpoint is directly challenged by a 2018 JAMA Cardiology paper coauthored by Allan Sniderman, comparing ten-year versus thirty-year risk horizons in terms of prevention. Sniderman and colleagues’ analysis found that looking at a thirty-year time frame rather than the standard ten years and taking aggressive precautionary measures early—like beginning statin treatment earlier in certain patients—could prevent hundreds of thousands more cardiac events, and by implication could save many lives.
For context, most studies of statins used in primary prevention (that is, prevention of a first cardiac event) last about five years and typically find a “number needed to treat” (or NNT, the number of patients who need to take a drug in order for it to save one life) of between about 33 and 130, depending on the baseline risk profile of the patients. (Amazingly, the longest statin trials to date have lasted just seven years.) But looking at their risk reduction potential over a thirty-year time frame, as the Sniderman study did, reduces the NNT down to less than 7: For every seven people who are put on a statin at this early stage, we could potentially save one life. The reason for this is simple math: risk is proportional to apoB exposure over time. The sooner we lower apoB exposure, thus lowering risk, the more the benefits compound over time—and the greater our overall risk reduction.
This encapsulates the fundamental difference between Medicine 2.0 and Medicine 3.0 when it comes to cardiovascular disease. The former views prevention largely as a matter of managing relatively short-term risk. Medicine 3.0 takes a much longer view—and more importantly seeks to identify and eliminate the primary causative agent in the disease process: apoB. This changes our approach to treatment completely. For example, a forty-five-year-old with elevated apoB has a lower ten-year risk than a seventy-five-year-old with low apoB. Medicine 2.0 would say to treat the seventy-five-year-old (because of their age), but not the forty-five-year-old. Medicine 3.0 says to disregard the ten-year risk and instead treat the causal agent in both cases—lowering the forty-five-year-old’s apoB as much as possible.
Once you understand that apoB particles—LDL, VLDL, Lp(a)—are causally linked to ASCVD, the game completely changes. The only way to stop the disease is to remove the cause, and the best time to do that is now.
Still struggling with this idea? Consider the following example. We know that smoking is causally linked to lung cancer. Should we tell someone to stop smoking only after their ten-year risk of lung cancer reaches a certain threshold? That is, do we think it’s okay for people to keep smoking until they are sixty-five and then quit? Or should we do everything we can to help young people, who have maybe just picked up the habit, quit altogether?
When viewed this way, the answer is unambiguous. The sooner you cut the head off the snake, the lower the risk that it will bite you.