CHAPTER 3
Objective, Strategy, Tactics
A Road Map for Reading This Book
Strategy without tactics is the slowest route to victory. Tactics without strategy is the noise before defeat.
—Sun Tzu
Several years ago, I flew to San Francisco to attend the funeral of the mother of a good friend from college, whom I’ll call Becky. Because Becky’s parents lived near Palo Alto, where I went to medical school, they invited me to dinner many times. We often ate in their garden, which had been beautifully planned and meticulously maintained by Becky’s mother, whose name was Sophie.
I remembered Sophie as a vibrant, athletic woman who had seemed ageless. But I hadn’t seen her since my wedding nearly fifteen years earlier. Becky filled me in on what I had missed. Beginning in her early seventies, Sophie had undergone a steep physical decline that began when she slipped and fell while gardening, tearing a muscle in her shoulder. That soon escalated into back and neck pain so severe that she could no longer work in the garden or play golf at all, her two primary passions in retirement. She simply sat around the house, feeling depressed. This was followed by a descent into dementia in the last couple of years of her life, before she died of a respiratory infection at age eighty-three.
At her memorial service, everyone agreed that it was a “blessing” that Sophie hadn’t had to linger in that demented state for very long, but as I sat in the pew, I reflected on the fact that she had spent the last decade of her life being unable to participate in any of the activities that had given her pleasure. Instead, she had been in considerable pain. Nobody mentioned that. We were gathered to mourn Sophie’s biological death, but it saddened me even more deeply that she had been robbed of the joy of her final years.
I often talk about Sophie with my patients, not because her tale is unusual but because it is so sadly typical. We have all watched our parents, grandparents, spouses, or friends undergo similar ordeals. The sad thing is that we almost expect this to happen to our elders; and even with this knowledge, relatively few of us take measures that might help ourselves avoid that fate. Even for Becky, who had cared for her mother during her difficult final years, the idea that she might end up in the same condition was probably the furthest thing from her mind. The future, for most of us, remains a hazy abstraction.
I tell Sophie’s story to help illustrate a fundamental concept in my approach to longevity, which is the need to think about and plan for the later decades of our lives—our seventies, eighties, nineties, or beyond. For many people, like Sophie, the last ten years of life are not a particularly happy time. They typically suffer from one or more of the Horsemen diseases and the effects of the requisite treatments. Their cognitive and physical abilities may be weakening or gone. Generally, they are unable to participate in the activities they once loved, whether that means gardening, or playing chess, or riding a bicycle, or whatever else in their life gave them joy. I call this the Marginal Decade, and for many, if not most, it is a period of diminishment and limitation.
I ask all my patients to sketch out an alternative future for themselves. What do you want to be doing in your later decades? What is your plan for the rest of your life?
Everyone has a slightly different answer—they might want to travel, or continue playing golf or hiking in nature, or simply be able to play with their grandkids and great-grandkids (top of my own list). The point of this exercise is twofold. First, it forces people to focus on their own endgame, which most of us might prefer to avoid thinking about. Economists call this “hyperbolic discounting,” the natural tendency for people to choose immediate gratification over potential future gains, especially if those gains entail hard work. Second, it drives home the importance of healthspan. If Becky wants to enjoy a healthy, rewarding life in her later years, and not repeat her mother’s fate, she will have to maintain and hopefully improve her physical and cognitive function every decade between now and then. Otherwise, the gravitational pull of aging will do its thing, and she will decline, just as her mother did.
Because I am a math guy, I like to visualize lifespan and healthspan in terms of a mathematical function, as in figure 2 on the following page—one of many graphs that I draw for my patients. The horizontal or x-axis of the graph represents your lifespan, how long you will live, while the vertical or y-axis represents a kind of sum total of your physical and cognitive function, the two age-dependent dimensions of healthspan. (Obviously, healthspan is not really quantifiable, but bear with my oversimplification.)
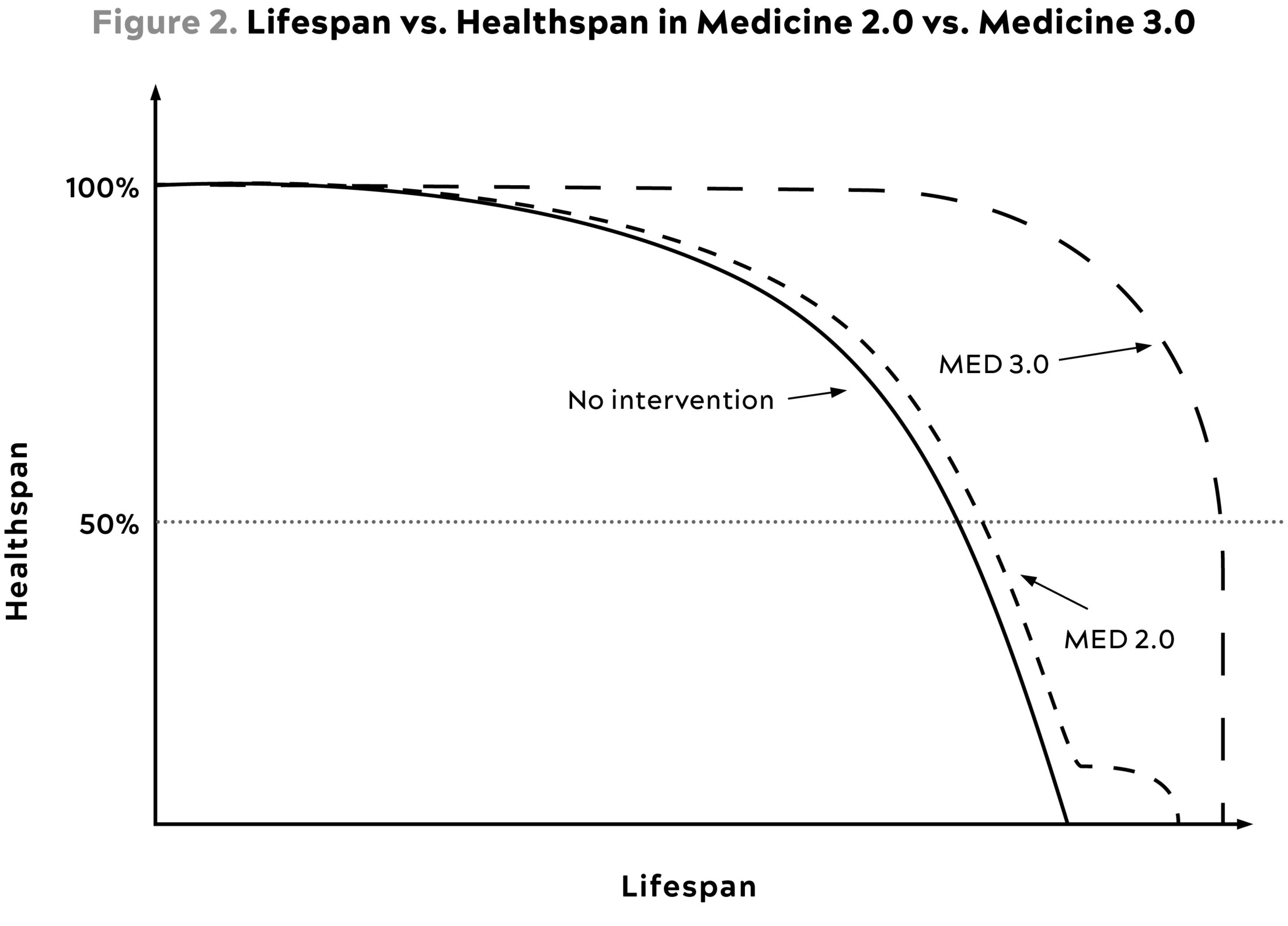
The black line represents the natural trajectory of your life: You are born at time zero, and for purposes of our diagram, we’ll say your physical and cognitive health start out at 100 percent. You remain relatively robust until about the fifth decade of life, at which point your cognitive and physical health will likely begin a gradual but steady decline, until you die (healthspan = zero) sometime in your sixties or early seventies. This would have been a not untypical lifespan for someone born into a hunter-gatherer or primitive agrarian tribe, provided they managed to avoid early death thanks to infectious disease or another calamity.
Now look at the typical modern life course, represented by the short-dashed line on the graph, marked “Med 2.0.” You will live a bit longer, thanks to the relative comfort and safety of our lives. But in midlife, you will gradually begin to feel some changes. You will lose a bit of your youthful strength and stamina. You might notice that you occasionally forget passwords, or the names of people you meet, or the names of actors in movies you watched long ago. Your friends and peers will begin to be diagnosed with cancer, cardiovascular disease and related conditions like high blood pressure, and diabetes or prediabetes. You will attend memorial services for friends from school.
At a certain point, the decline begins to steepen. Eventually, sometime around age seventy or seventy-five, give or take, your cognitive and physical capacities will diminish to roughly their halfway point (represented by the horizontal dotted line), which I sort of arbitrarily define as the point below which you are no longer able to do the things that you want to do with ease. You’re constrained, and bad stuff starts to happen more frequently and with greater consequence. It’s one thing to break your femur in a skiing accident when you’re forty and still strong and resilient; it’s quite another to break it falling off a curb when you’re seventy-five and functioning at 25 percent of your capacity. At the same time, your own risk of chronic disease is rising exponentially.
This is where Medicine 2.0 steps in. We treat your heart disease, or cancer, or whatever else afflicts you, prolonging your life by a few months, or years if you’re lucky. This is when the lifespan/healthspan curve flattens out horizontally to the right, representing this postponement of death. But now look at where this occurs: when your healthspan is already compromised. This means that we have delayed your death without significantly improving your quality of life—something at which Medicine 2.0 is quite adept. This is the Marginal Decade that most of us can expect, in our current system.
Now look at the long-dashed line on the graph. This represents your ideal trajectory. This is what you want. Instead of beginning a slow decline in midlife, your overall healthspan stays the same or even improves into your fifties and beyond. You will be fitter and healthier at fifty-five and even sixty-five than you were at forty-five and will remain physically fit and cognitively sharp well into your seventies and eighties, and possibly beyond. You will seem like someone a decade younger than the age on your passport, or possibly two. There is much more space under this curve, and all that space represents your longer, better life: more time being with your family, pursuing your passions, traveling, or continuing to do meaningful work. Moreover, when you do begin to decline, the descent is steep but relatively brief. This is called squaring the longevity curve.
In this scenario, we live longer, and we live better for longer. We outlive our life expectancy, and we also exceed society’s expectations of what our later life is supposed to look like. Instead of a lousy Marginal Decade, we get to enjoy what feels more like a “Bonus Decade”—or decades—when we are thriving in every dimension. This is our objective: to delay death, and to get the most out of our extra years. The rest of our lives becomes a time to relish rather than to dread.
The next obvious question is: How do we accomplish this? How do we lengthen our lifespan while simultaneously extending our healthspan? How do we stave off death via the Horsemen while slowing or even reversing physical, cognitive, and emotional decline?
What’s our plan?
This is where most people make a wrong turn. They want to take a shortcut, right to the tactics: this is what to eat (and not eat), that is how you should exercise, these are the supplements or medications you need, and so on. There are warehouses full of books that purport to have the answers, but the one you are reading now is not one of them. Instead, I believe this is exactly where we need to hit pause and take a step back, lest we skip the most important step in the process: the strategy.
Take another look at the Sun Tzu quote that opens this chapter: “Tactics without strategy is the noise before defeat.” He was talking about war, but it applies here as well. To achieve our objectives, we first need to have a strategy: an overall approach, a conceptual scaffolding or mental model that is informed by science, is tailored to our goals, and gives us options. Our specific tactics flow from our strategy, and the strategy derives from our objective. We know what the objective is by now, but the strategy is the key to victory.
The big mistake people often make is to conflate strategy and tactics, thinking they are the same. They are not. I like to explain this distinction using one of the more memorable boxing matches of all time: Muhammad Ali versus George Foreman, the famed “Rumble in the Jungle” that took place in Kinshasa, Zaire, in 1974. Ali’s objective, obviously, was to win the match against Foreman and regain his heavyweight title. The problem Ali faced was that Foreman was younger, stronger, meaner, and favored to win in devastating fashion. It’s hard to reconcile with the jovial guy who sells countertop grills now, but back in the day George Foreman was considered the meanest SOB who ever laced on boxing gloves. He was viewed as literally invincible. The pundits all agreed that colorful and beloved as he was, Ali didn’t stand a chance—which is why he needed a strategy.
Ali knew he had certain slight advantages over Foreman in that he was faster, more experienced, and mentally tougher. He also knew that Foreman was hotheaded and prone to anger. Rather than try to counter Foreman punch for punch, Ali decided that he would attempt to induce the younger, less seasoned fighter to wear himself out, leaving him frustrated and tired, and thus vulnerable. If he could accomplish that, he knew it would be a more even match. This was his strategy: make Foreman angry, and then let him flail away until he had exhausted himself and Ali could mount an offensive.
From this strategy flowed the tactics that are now legendary: first, come at Foreman with a series of lead straight rights, an obvious, even disrespectful punch that was guaranteed to make Foreman mad. Nobody hits the heavyweight champion of the world like that. Ali then let an enraged Foreman chase him around the ring and press him up against the ropes, wasting energy, while he concentrated on trying to minimize the damage he absorbed—the famous “rope-a-dope.”
For the first few rounds, everyone thought Foreman was absolutely crushing Ali, including Foreman. But because Ali’s strategy was to try to outlast Foreman, he had trained himself to endure the abuse. By about the fifth round, you can almost see Foreman realizing, Damn, I’m already gassed. Meanwhile, Ali’s superior physical conditioning meant he had much more left in the tank. He went on to win the match via a knockout in the eighth round.
The point is that the tactics are what you do when you are actually in the ring. The strategy is the harder part, because it requires careful study of one’s opponent, identifying his strengths and weaknesses, and figuring out how to use both to your advantage, well before actually stepping in the ring. In this book, we will apply this three-part approach to longevity: objective → strategy → tactics.
Our Strategy
Going into the fight with Foreman, Ali knew that time was on his side. The longer he could keep his opponent riled up and wasting energy, while avoiding getting knocked out himself, the better his chances of winning in the long run. Unfortunately for us, time is definitely not on our side. Every moment we are alive, our risk of disease and death is tugging at us, the way gravity pulls a long jumper toward earth.
Of course, not every problem you face requires a strategy. In fact, many don’t. You don’t need a strategy if your objective is, say, to avoid getting a sunburn. Your straightforward tactical options are to put on sunblock, long sleeves and pants, and perhaps a big hat, or to stay out of the sun altogether. But we need a strategy in order to live longer and better, because longevity is a far more complex problem than sunburn.[*1]
Living longer means delaying death from all four of the Horsemen. The Horsemen do have one powerful risk factor in common, and that is age. As you grow older, the risk grows exponentially that one or more of these diseases has begun to take hold in your body. Unfortunately, there’s not much we can do about our chronological age—but what do we mean by “aging,” exactly? It’s not merely the passage of time, but what is happening inside us, beneath the surface, in our organs and our cells, as time passes. Entropy is working on us every single day.
“Aging is characterized by a progressive loss of physiological integrity, leading to impaired function and increased vulnerability to death,” wrote the authors of an influential 2013 paper describing what they termed the “hallmarks of aging.” They continued: “This deterioration is the primary risk factor for major human pathologies, including cancer, diabetes, cardiovascular disorders, and neurodegenerative diseases.”
The very process of aging itself is what makes us vulnerable to these diseases, while also affecting our healthspan. Someone who drops dead of a heart attack did not just get sick an hour earlier. The disease was working inside them, silently and invisibly, for decades. As they grew older, their own internal defense mechanisms weakened, and disease gained the upper hand. We saw something similar in the COVID-19 pandemic. The virus infected people across all age groups, but it killed older people in vastly disproportionate numbers, precisely because it exposed and exploited their existing vulnerability to disease and death: their weakened immune systems, their cardiovascular and respiratory issues, and so on. Thus, our strategy must account for the effects of aging, just as Ali took his own advancing years into account as he searched for a way to defeat Foreman. Without the right strategy, Ali would have almost certainly lost the fight.
This is why we can’t just skip ahead to the tactics, where I tell you what to do. If you are tempted, my advice is to pause, take a breath, and settle in. Without an understanding of the strategy, and the science that informs it, our tactics will not mean much, and you’ll forever ride the merry-go-round of fad diets and trendy workouts and miracle supplements. You’ll be stuck in a Medicine 2.0 mentality, seeking a quick fix to your problems. The only way to become an adroit tactician is to shift your mindset to Medicine 3.0, which requires becoming a master strategist first.
In the chapters to come, we will be taking a deep dive into some of the mechanisms underlying the aging process, and we will also be taking a very close look at the inner workings of each of the Horsemen diseases. How and when do they begin? What forces drive them—internal and external? How are they sustained? Most importantly, how can they be delayed or even prevented entirely? As we’ll see in the next chapter, this is how the centenarians achieve their extraordinarily long lifespans: they delay or prevent the onset of chronic disease, by decades compared to the average.
We will also be taking a more detailed look at healthspan—another one of those overused buzzwords that has lost all meaning. The standard definition, as the period of life when we are free from disease and disability, sets far too low of a bar. If we’re not sick and housebound, then we’re “healthy”? I prefer to use more pointed language—so pointed that it often makes my patients uncomfortable.
Here’s another way to think of it. Lifespan deals with death, which is binary: you’re alive, and then you’re dead. It’s final. But before that happens, sometimes long before, most people suffer through a period of decline that, I would argue, is like dying in slow motion. Certainly, that was the case for Sophie, Becky’s mom. This can happen quickly, such as after a bad accident, but usually it goes so slowly that we barely perceive the change.
I think about healthspan and its deterioration in terms of three categories, or vectors. The first vector of deterioration is cognitive decline. Our processing speed slows down. We can’t solve complex problems with the quickness and ease that we once did. Our memory begins to fade. Our executive function is less reliable. Our personality changes, and if it goes on for long enough, even our sentient self is lost. Fortunately, most people don’t progress all the way to frank dementia, but many people experience some decline in their cognitive capacity as they age. Our objective is to minimize this.
The second vector of deterioration is the decline and eventual loss of function of our physical body. This may precede or follow cognitive decline; there is no predetermined order. But as we grow older, frailty stalks us. We lose muscle mass and strength, along with bone density, stamina, stability, and balance, until it becomes almost impossible to carry a bag of groceries into the house. Chronic pains prevent us from doing things we once did with ease. At the same time, the inexorable progression of atherosclerotic disease might leave us gasping for breath when we walk to the end of the driveway to fetch the newspaper (if newspapers still exist when we are old). Or we could be living a relatively active and healthy life until we fall or suffer some unexpected injury, as Sophie did, that tips us into a downward spiral from which we never recover.
My patients rarely expect this decline to affect them. I ask them to be very specific about their ideal future. What do they want to be doing when they are older? It’s striking how rosy their predictions tend to be. They feel supremely confident that they will still be snowboarding or kickboxing, or whatever else it is they enjoy doing now, when they’re in their seventies and eighties.
Then I stop them and explain: Look, in order to do that, you will need to have a certain level of muscular strength and aerobic fitness at that age. But even right now, at age fifty-two (for example), your strength and your maximum volume of oxygen uptake (VO2 max) are already barely sufficient to do those things, and they are virtually certain to decline from here. So your choices are (a) surrender to the decline, or (b) come up with a plan, starting now.
No matter how ambitious your goals are for your later years, I suggest that you familiarize yourself with something called the “activities of daily living,” a checklist used to assess the health and functionality of elderly people. The list includes such basic tasks as preparing a meal for oneself, walking without assistance, bathing and grooming, using a phone, going to the grocery store, handling personal finances, and so on. Now imagine living your life without the ability to feed or bathe yourself or walk a few blocks to meet friends for coffee. We take these for granted now, but to continue to live actively as we age, retaining even these minimal abilities, requires us to begin building a foundation of fitness and to maintain it diligently.
The third and final category of deterioration, I believe, has to do with emotional health. Unlike the others, this one is largely independent of age; it can afflict outwardly healthy young people in their twenties, or it can creep up on you in middle age, as it did with me. Or it can descend later in life. Surveys show that happiness tends to reach its nadir in our forties (age forty-seven, to be exact), but as I learned through painful experience, middle-aged distress often has its roots much earlier, in adolescence or childhood. And we may not recognize that we are in danger until we reach a crisis point, as I did. How we deal with it has a huge bearing on our physical health, our happiness, and our very survival.
To me, longevity as a concept is really only meaningful to the extent that we are defying or avoiding all these vectors of decline, simultaneously. And none of these individual components of longevity is worth much without all the others. To live to the age of one hundred without our mind and our body intact is not something that anyone would willingly choose. Similarly, to have the greatest quality of life, only to have it cut short at a young age, is also undesirable. And to retain good health as we age, but without love and friendship and purpose, is a purgatory I would not wish on my worst enemy.
The important distinction here is that while actual death is inevitable, this deterioration that we’re talking about is less so. Not everyone who dies in their eighties or nineties passes through the valleys of cognitive, physical, or emotional destruction on the way there. They are preventable—and I believe that they are largely optional, despite their ever-increasing gravitational pull over time. As we will see in later chapters, cognitive, physical, and even emotional deterioration can all be slowed and even reversed in some cases with the application of the proper tactics.
The other key point is that lifespan and healthspan are not independent variables; they are tightly intertwined. If you increase your muscle strength and improve your cardiorespiratory fitness, you have also reduced your risk of dying from all causes by a far greater magnitude than you could achieve by taking any cocktail of medications. The same goes for better cognitive and emotional health. The actions we take to improve our healthspan will almost always result in a longer lifespan. This is why our tactics are largely aimed at improving healthspan first; the lifespan benefits will follow.
Tactics
The key difference between Medicine 2.0 and Medicine 3.0 has to do with how and when we apply our tactics. Typically, Medicine 2.0 steps in only when something is acutely wrong, like an infection or a broken bone, with short-term fixes for the immediate problem. In Medicine 3.0, our tactics must become interwoven into our daily lives. We eat, breathe, and sleep them—literally.
Medicine 2.0 relies on two types of tactics, broadly speaking: procedures (e.g., surgery) and medications. Our tactics in Medicine 3.0 fall into five broad domains: exercise, nutrition, sleep, emotional health, and exogenous molecules, meaning drugs, hormones, or supplements. I will not be talking much about molecules, because that would make this book twice as long as it already is, but one thing that I will say is that I do not shy away from pharmaceutical drugs because they are not “natural.” I consider many drugs and supplements, including lipid-lowering medications, to be essential items in our longevity tool kit, and I hope that in the not-too-distant future we will have many even more effective tools at our disposal.
Drugs and supplements aside, our first tactical domain is exercise. Like “healthspan,” exercise is another one of those overly broad blanket terms that annoy me, because it can encompass everything from a walk in the park to a hard bike ride up a mountain pass, a set of tennis, or a session in the gym lifting heavy weights. These all count as “exercise,” but they obviously have very different effects (and risks, by the way). So we will break down this thing called exercise into its most important components: strength, stability, aerobic efficiency, and peak aerobic capacity. Increasing your limits in each of these areas is necessary if you are hoping to reach your limit of lifespan and healthspan. Again, my goal is not to tell you how to lose weight fast or improve the aesthetic quality of your midsection. We want to maintain physical strength, stamina, stability across a broad range of movements, while remaining free from pain and disability.
This is another area where my thinking has changed over time. I used to prioritize nutrition over everything else, but I now consider exercise to be the most potent longevity “drug” in our arsenal, in terms of lifespan and healthspan. The data are unambiguous: exercise not only delays actual death but also prevents both cognitive and physical decline, better than any other intervention. We also tend to feel better when we exercise, so it probably has some harder-to-measure effect on emotional health as well. My hope is that you will understand not only the how but the why of various types of exercise, so you will be able to formulate a program that fits your own personal goals.
Our second domain is nutrition. I won’t be telling you to eat this, not that, or prescribing a specific diet that everyone should follow, and I’m definitely not taking sides in the pointless, never-ending diet wars pitting low carb versus paleo versus vegan, and so on. We will avoid such religious discussions in favor of biochemical evidence. The best science out there says that what you eat matters, but the first-order term is how much you eat: how many calories you take into your body.
How you go about achieving the Goldilocks zone here—not too much, not too little, but just right—will vary depending on numerous factors. My goal is to enable you to determine the best eating pattern for yourself. But please keep in mind that none of the tactics we will discuss are set in stone; we seek feedback from as many sources as possible to try to determine what works and what doesn’t. A good strategy allows us to adopt new tactics and discard old ones in service of our objectives.
Next is sleep, which I and many others had ignored for far too long. Fortunately, over the past decade or so sleep has finally received the attention it deserves. Today, we have a far better understanding of its importance, and what goes wrong in the short and long term when our sleep is compromised (spoiler: a lot). There is not much that can compare to the feeling of waking up from a great night of sleep, feeling completely refreshed and totally primed for the day. Good sleep is critical to our innate physiological repair processes, especially in the brain, while poor sleep triggers a cascade of negative downstream consequences, from insulin resistance to cognitive decline, as well as mental health issues. I too used to be one of those people who enjoyed pulling all-nighters and thought sleep was for people who had nothing better to do. Long story short, I found out how wrong I was in very dramatic fashion. I am now convinced that Not-Thin Peter’s biggest problem was less what he ate than how little he slept.
Finally, we will explore the importance of emotional health, which I believe is every bit as important a component of healthspan as the others. This is an area in which I have very little professional expertise but a great deal of personal experience. So while I do not have much hard experimental data and studies to point to, as in the other chapters, I will be sharing my own very long and painful journey to come to terms with things that happened to me in the past and to correct my own behavior and heal the relationships that I have damaged. If nothing else, it may serve as a cautionary tale—and a prod to get you to consider the state of your own emotional house, if warranted.
I will discuss my journey in much more detail in chapter 17, but one phrase from that period has stuck with me, almost like a mantra. It is something that one of my therapists, Esther Perel, said to me early in our work together.
“Isn’t it ironic that your entire professional life is predicated around trying to make people live longer,” she mused, “yet you’re putting no energy into being less miserable, into suffering less emotionally?”
She continued: “Why would you want to live longer if you’re so unhappy?”
Her logic was undeniable, and it changed my whole approach to longevity.
From Evidence Based to Evidence Informed
It’s important, obviously, that our strategy be based on evidence. Unfortunately, the pursuit of longevity is where the most powerful tool of Medicine 2.0, the randomized clinical trial in humans, runs into a brick wall. Randomized controlled trials are used to determine cause and effect in relatively simple, short-term situations. It’s fairly easy, for example, to run a study showing that sunscreen prevents sunburn. But such studies are of limited use in our quest for longevity.
This is where my approach may ruffle some people’s feathers. The purists of evidence-based medicine demand data from randomized controlled trials (RCTs) before doing anything. Those trials are the gold standard of medical evidence, yet they also reinforce some major limitations of Medicine 2.0, beginning with its short time horizon. In general, the types of clinical questions that are best resolved by RCTs are those involving simple interventions such as a vaccine, or a medication to lower cholesterol. We give this treatment over a relatively short period, from six months up to maybe five or six years at the longest and look for its effect on a specified outcome. Does the vaccine reduce the rate of serious illness and death? Does this drug lower cholesterol and prevent cardiac death, or at least heart attacks, in highly susceptible individuals?
This type of study is the foundation of evidence-based medicine. But if our goal is longevity, the situation becomes more complicated. A one-year clinical trial, or even a five-year study, will not tell us everything we need to know about disease processes that take decades to unfold. There will never be a clinical trial to guide a cardiovascular prevention strategy for a healthy forty-year-old. It would simply take too long to do the study. Furthermore, outside of pharmacology, the interventions are very complex, particularly if they involve exercise, nutrition, and sleep. Studying longevity itself in this way is almost impossible—unless we could somehow take a hundred thousand babies, randomize them to four or five different interventions, and follow them throughout their lifetimes. That would (hopefully) yield a rock-solid, evidence-based prescription for maximizing lifespan and healthspan. But the obstacles to doing this are insurmountable, not least because it would require a century to complete.
Option B is to look at the different types of data that we do have and then develop a strategy that triangulates between them. This might not definitively solve the problem, but it can at least point us in the right direction. Our Option B strategy is based on combining insights from five different sources of data that, viewed separately, probably aren’t strong enough to act on. When taken together, however, they can provide a solid foundation for our tactics. But our supporting framework must shift, from exclusively evidence-based to evidence-informed, risk-adjusted precision medicine.
Our first source of data comes from studies of centenarians, people who have lived to the age of one hundred and beyond, often in good health. These are the extreme outliers, the tiny sliver of the population who have outlived our usual life expectancy by two decades or more. By and large, they have delayed or evaded the diseases that kill most of the rest of us, and many of them have remained in fairly good shape. We would like to know how they accomplished this feat. What do centenarians have in common? What genes do they share that might give them an advantage over noncentenarians? What explains their survival and their apparently slower rate of aging? And most of all, what can the rest of us do to emulate their good fortune?
This evidence is made stronger by the fact that centenarians represent our “species of interest”—that is, they are human. Unfortunately, centenarian data are almost entirely observational rather than experimental, so we can’t truly infer cause and effect. Centenarians’ life histories and habits tend to be idiosyncratic, to say the least, and the fact that their numbers are relatively small means that it can be difficult to draw firm conclusions at all. (We will discuss centenarians in more detail in the next chapter.)
Next, we turn to lifespan data from animal “models,” such as laboratory mice. It is obviously much easier, ethically and logistically, to test lifespan-altering tactics in mice, which typically only live about two or three years, than in humans. We have a huge amount of data about how different sorts of interventions, both dietary and in the form of exogenous molecules, affect mouse lifespan. The limitation, obviously, is that mice are not human; many drugs have succeeded in mice only to fail spectacularly in human studies. There are other types of animal models, including a tiny species of nematode worm called C. elegans that is often used in research, as well as fruit flies, dogs, primates, and even lowly yeast cells. All of these have strengths and weaknesses. My rule of thumb is that if a given intervention can be shown to extend lifespan or healthspan in multiple species spanning a billion years of evolution, for example, from worms to monkeys, then I am inclined to take it seriously.
A third and important source of information to support our strategy comes from human studies of the Horsemen: cardiovascular and cerebrovascular disease, cancer, Alzheimer’s disease and related neurodegenerative conditions, and type 2 diabetes and related metabolic dysfunction. How do these diseases begin? How do they progress? What risk factors help to cause them, or fuel them? What underlying factors do they share? What are the cutting-edge treatment modalities for those with “advanced” disease—and what do they tell us about developing a strategy for prevention? We want to know each of these diseases inside and out, understanding their weaknesses and vulnerabilities, just as Ali scrutinized Foreman before their match.
Fourth, we consider the molecular and mechanistic insights derived from the study of aging in both humans and animal models. We have learned an enormous amount about the cellular changes that occur during the aging process and in specific diseases. From this, we also have developed some ideas for how to manipulate these changes, via exogenous molecules (e.g., drugs) or behavioral changes (e.g., exercise).
Our final source of insights is a very clever method of analysis called Mendelian randomization, or MR for short. MR helps bridge the gap between randomized controlled trials, which can establish causality, and pure epidemiology, which often cannot. We’ll talk about epidemiology in more detail later, but while it has proved useful in certain situations, such as determining the link between smoking and lung cancer, it has been less useful in more complex scenarios. Mendelian randomization helps tease out causal relationships between modifiable risk factors (e.g., LDL cholesterol) and an outcome of interest (e.g., cancer) in situations where actual randomized experiments cannot easily be done. It accomplishes this by letting nature do the randomization.[*2] By considering the random variation in relevant genes and comparing them against the observed results, it eliminates many of the biases and confounders that limit the usefulness of pure epidemiology.
For example, some epidemiologic studies have suggested an inverse relationship between LDL cholesterol and cancer risk. That is, people with lower LDL cholesterol appear to have a higher risk of cancer. But is the relationship causal? That’s a tricky but important question. If true, it would imply that lowering LDL cholesterol, such as with statins, increases the risk of cancer, which would obviously be bad news. Epidemiology does not tell us the direction of causality, so we turn to MR.
With MR, we can look at genetic variations that result in low, medium, and high levels of LDL cholesterol. These genes are randomly occurring, so they serve as a proxy for a randomized natural experiment. By examining the relationship between the resulting LDL cholesterol levels and cancer incidence, we can answer the question without the usual confounders that plague traditional epidemiology. And lo and behold, it turns out that low LDL cholesterol does not cause cancer or increase its risk. If we use the same technique to look at the effect of LDL levels on cardiovascular disease (our dependent variable), it turns out that higher LDL cholesterol is causally linked to the development of cardiovascular disease (as we’ll discuss in chapter 7).
An astute reader will notice that one concept has been conspicuously absent from this chapter so far: absolute certainty. This took me a little while to grasp when I transitioned from mathematics to medicine, but in biology we can rarely “prove” anything definitively the way we can in mathematics. Living systems are messy, and confounding, and complex, and our understanding of even fairly simple things is constantly evolving. The best we can hope for is reducing our uncertainty. A good experiment in biology only increases or decreases our confidence in the probability that our hypothesis is true or false. (Although we can feel fairly certain about some things, such as the evidence supporting the idea that your doctor should wash her hands and put on sterile gloves before operating on you.)
In the absence of multiple, repeated, decades-long randomized clinical trials that might answer our questions with certainty, we are forced to think in terms of probabilities and risk. In a sense it’s a bit like charting an investment strategy: we are seeking the tactics that are likeliest, based on what we know now, to deliver a better-than-average return on our capital, while operating within our own individual tolerance for risk. On Wall Street, gaining an advantage like this is called alpha, and we’re going to borrow the idea and apply it to health. I propose that with some unorthodox but very reasonable lifestyle changes, you can minimize the most serious threats to your lifespan and healthspan and achieve your own measure of longevity alpha.
My aim here is to equip you with a set of tools that you can apply to your own specific situation—whether you need to pay attention to your glucose regulation, your weight, your physical condition, your Alzheimer’s disease risk, and so on. Your personal tactics should never be static, but will evolve as needed, as you journey through life with all its uncertainties—and as we learn more about the science of aging and the workings of diseases like cancer. As your own situation changes, your tactics can (and must) change, because as the great philosopher Mike Tyson once put it, “Everyone has a plan until they get punched in the mouth.”
Advice George Foreman could have used.