8
Emotional Embodiment and Affect Tolerance
Chapter summary: discusses factors that determine affect tolerance, and discusses how expanding the brain and body physiology to expand emotional experiences in it can quickly contribute to improving a person’s capacity for tolerating them.
The most important assumption in emotional embodiment work is that emotional embodiment—expansion of the emotional experience to as much of the brain and body physiology as possible—brings about greater affect tolerance: the enhanced capacity to bear and stay with a difficult emotional experience over a longer period of time, which is often required for successful resolution of past traumas. In this chapter, we explore how that might be possible, especially for unpleasant emotional experiences that our brains are innately programmed to resist. Throughout this chapter, the combined physiology of the brain and body will be referred to simply as the physiology. The terms “body physiology” and “brain physiology” will be used when there is a need to distinguish between them.
The Basic Physiology of Pleasant and Unpleasant Emotional Experiences
As we saw in chapter 5, emotions are assessments of the impact of a situation on a person’s well-being. Pleasant emotional experiences are movements in the direction of improvement in one’s well-being. In essence, pleasant emotions result from increases in states of regulation, or decreases in states of dysregulation, in the physiology. On the other hand, unpleasant emotions are movements in the direction of worsening in one’s well-being. They are, in essence, increases in states of dysregulation and decreases in states of regulation in the physiology. We breathe with greater ease, are less stressed, and feel an increase in our well-being when we are experiencing love in a secure relationship. We breathe with difficulty, are more stressed, and feel a decrease in our well-being when we feel the hurt from the breakup of the same relationship.
Experiences of states of regulation in the physiology are inherently more pleasurable. Experiences of states of dysregulation, on the other hand, are inherently more painful. For this reason, evolution has programmed us to avoid unpleasant emotional states and seek pleasant emotional states to maximize our chances of survival.1 Unpleasant emotional experiences, as states of dysregulation, threaten our survival by compromising our physiology. Conversely, pleasant emotional experiences, as states of regulation, improve our physiology and enhance our survival. One reason—perhaps the most important reason—why we have much difficulty in tolerating and being with unpleasant emotional experiences has to do with the fact that they are inherently painful. It is much easier to be with the pleasure of a wedding engagement than with the pain of a divorce!
A Simple Model of the Physiology of Regulation and Dysregulation
The physiology of regulation and dysregulation, which as we saw in chapter 5 is also the physiology of emotion, is extremely complex. It is the subject of inquiry in a large number of disciplines, including medicine. For our purpose, to understand how expanding the physiology to expand the emotional experience can make the emotional experience more bearable, we need a model of the physiology of regulation and dysregulation. So, let us build a simple one.
The regulation and dysregulation of the physiology can be understood in terms of certain flows that are vital for the physiology’s health and functioning. First is the flow of blood. Blood carries basic nutrients such as oxygen and glucose, regulatory biochemicals such as hormones, immune agents such as white blood cells, information such as blood sugar level, and waste products such as carbon dioxide, from one part of the physiology to another. Second is the flow of information back and forth between the brain and the body through the sensory and motor nerves of the somatic and autonomic nervous systems. This flow is essential for the brain to gather information about the body and to regulate the body based on that information.
The third flow is the interstitial or extracellular flow: the flow of fluid between the cells, through which nutrients such as minerals and messenger molecules such as peptides are carried from one part of the physiology to another.2 The fourth flow is the lymphatic flow, which plays a role in managing fluid levels in tissues, absorbing fat from the intestines, protecting the body from invaders by producing and distributing immune cells such as white blood cells, and removing waste products.3 The fifth flow is the flow of measurable electromagnetic energies from one part of the physiology to another, which are now known to play a role in regulating the physiology.4 The sixth flow is the flow of quantum energies at the subatomic level between one part of the physiology and another that are involved in generating and regulating experiences in the physiology.5,6
Whether the physiology is regulated or dysregulated, overall or in part, depends very much on the state of these six vital flows from one part of the physiology to another. When these flows are relatively unobstructed, we can imagine that the level of regulation and the person’s well-being would be on the high side, with lower levels of stress. On the other hand, if there are significant disruptions in one or more of these vital flows, one can expect dysregulation, disease, and reduction in one’s well-being, with higher levels of stress. Because the physiology is an integral unit wherein every part depends on every other part for its functioning, the level of overall regulation, health, and well-being throughout the physiology could be diminished when these vital flows are hamstrung even in one or a few areas of the physiology. Disruption in the vital flows can also be expected if there is significant damage to one or more parts of the highly interdependent physiology.
Through the lens of this simple model of regulation and dysregulation, unpleasant emotional experiences, because they are states of dysregulation and high stress, can be expected to involve disruptions in one or more of the six vital flows in one or more parts of the physiology. Pleasant emotional experiences, because they are states of greater regulation with lower levels of stress, can be expected to involve less disruption in these vital flows among different areas of the physiology.
One might wonder if unpleasant emotional experiences always involve disruption in one or more of the six vital flows that have been identified as having to do with regulation and dysregulation in the physiology. After all, we saw in chapter 5 that emotional experiences can be generated in the brain alone through neurotransmitter action or through recall of prior emotional experiences. Even in such instances, disruptions of the vital flows can occur. Unpleasant emotional experiences generated in the brain might elicit physiological defenses against them in the brain physiology itself, which can lead to disruption in the essential flows within the brain physiology and between the brain and the body physiology. The emotional experiences generated in the brain physiology can also elicit defenses against emotions in the body physiology, such as reduction in one’s breathing to decrease oxygen to the brain, to ease the emotional intensity there.
As brain-generated unpleasant emotional experiences extend to the body (which they often do), it is hard to imagine situations in which physiological defenses against emotions activated in the body would not lead to disruption of the vital flows in the body physiology. One might also think of the possibility that unpleasant emotional experiences could be created without involving any disruption in the vital flows in another way. For example, painful experiences could theoretically be generated through the stimulation of pain receptors that are distributed all over the body, without any disruption. However, physiological defenses such as constriction and numbing almost always occur in response to pain and do disrupt the vital flows of information and substances from one part of the physiology to the other.
The Effects of Physiological Defenses against Emotions on the Physiology of Regulation
As we saw in chapter 7, when we are coping with a situation with everything we have, our emotional experiences could become too much for us to handle, and they could start to compromise our ability to continue coping with the situation. This might happen because the dysregulation in our physiology could become so extreme as to threaten our very survival, as when our heart rate might go so high as to risk a heart attack; or our brain might be unable to bear the emotional experience because its threshold or limit for tolerating suffering is exceeded, as when the pain in the heart from a breakup is simply too much. The disruption caused by the threat to one’s survival in the first instance, and the distraction from the unbearable suffering in the second, could interfere with and compromise our cognitive and behavioral processes involved in coping with the current situation.
We saw in chapter 7 that in order to prevent overwhelming emotional experiences from compromising our ability to cope with a situation, nature has provided us with a number of physiological defenses to manage them. For example, endogenous opioids, secreted as a defense against overwhelming emotions such as debilitating terror and helplessness in an extremely dangerous situation, can make a person feel paradoxically calm and collected so they can plot their escape cognitively and behaviorally. Such physiological defenses against extreme emotional experiences in the course of coping with difficult situations throughout our lives are indeed adaptive. They can be seen as additional coping mechanisms to make sure our emotional experience (our assessment of the impact of a situation on our well-being) does not in itself become disruptive of our ability to continue to cope with the situation through cognition and behavior.
However, physiological defenses against emotions come with a price. They tend to disrupt the vital flows and therefore dysregulate the physiology. For example, constriction dynamics can inhibit blood, lymph, and interstitial flows. Inhibition of respiratory and cardiovascular functions can also disrupt these three flows. Biochemical dynamics such as numbing can disrupt the flow of information through the nerves—information that needs to go between the brain and the body for the brain to sense and regulate what is happening in the body. However, these dynamics save the day in that they help prevent unbearable emotional experiences from overwhelming our cognition and behavior. Given the alternative—threats to our physiological and psychological survival—it is a small price to pay in the short run. However, physiological defenses against emotions can cause physiological and psychological dysfunction if they persist over the long term.
Not all physiological defenses against emotions might disrupt the vital regulatory flows. For example, arousal or charge as a defense against depression cannot be thought of as inhibitory of any of the vital flows, even though prolonged use of it can stress the physiology, create unpleasantness, trigger inhibitory defenses such as constriction and numbing, and in turn disrupt the vital flows. Most physiological defenses against emotions, such constriction of tissue and movement, and inhibition of various biological functions, tend to be inhibitory and are therefore disruptive of vital regulatory flows.
We use the physiological and psychological defenses at our disposal to cope with unbearable experiences. Inhibitory physiological defenses against emotional experiences, such as constriction and numbing, are often biologically expensive because, as we have seen, they tend to disrupt the vital flows that regulate our physiology. Psychological defenses against emotional experiences that use our cognition and behavior to protect us might be less expensive. We can at times cognitively convince ourselves that our abusive partner is not really all that bad, so as to help ourselves feel less bad. Or we might just use work as a behavioral defense to feel good and avoid feeling how lousy our relationship is making us feel. However, we cannot continue to cope with an ongoing difficult situation such as a bad marriage in the long run only cognitively and behaviorally without physiological consequences.
We are less capable of using cognitive and behavioral defenses when we are children than when we are adults. For this reason, when children encounter traumatic situations, they are more likely than adults are to freeze and dissociate, as opposed to fighting, fleeing, or reasoning their way out of it. Children who have not had the necessary support and opportunity to work through their childhood traumas emotionally are also more likely to become adults who are prone to psychophysiological symptoms.
Our focus here is on how physiological defenses affect the physiology of regulation in terms of the vital flows that govern it. Our physiological defenses against overwhelming experiences in the middle of a crisis can unfortunately persist beyond the event, increasing the level of dysregulation in the physiology. They can kick in automatically if similar situations trigger unresolved emotions stemming from the original event. For example, a child can develop asthma from shutting down the respiratory physiology to manage the overwhelming experience of separation from their mother.7 Just to be clear, please note that a child can develop asthma for many reasons, including allergies. And not all children separated from their mothers develop asthma as a psychophysiological symptom. Still, the child who develops asthma from the stress of separation from their mother might continue to have asthma attacks as an adult whenever there is a threat of a loss in relationship, if the adult has not worked through the trauma of the original separation.
The patterns of defense engaged during the loss can also become generalized and form automatic defensive reaction patterns to any event that causes significant stress, in relationships or other contexts. The constriction pattern on the right side of my cranium—resulting from my birth, in which I nearly died, along with my mother—continues to kick in and cause discomfort and dysfunction when I am stressed beyond a certain point, no matter the source of stress. In the field of pre- and perinatal psychology, the twisting constriction of the structures of the spine in the womb into a dysfunctional scoliosis pattern is believed to be a defense mechanism instinctually employed to manage overwhelming unpleasant emotional experiences, such as existential terror and fragmentation. In all these ways, physiological defenses against emotions can persist—like the emergency brake engaged in a dangerous road condition staying on after the danger has passed—and can thus contribute to psychological and psychophysiological symptoms, until there is no longer a reason for them to be triggered to defend against unbearable experiences.
How does one ensure that physiological or psychological defenses against overwhelming emotions used in difficult situations do not cause pathologies? A standard answer in psychology is that we have to resolve the emotions involved by working with the situations they arise in. To complete an emotional experience such as a heartbreak, so that we are not constantly defending against it by shutting our heart down as soon as it rears its ugly head from the unconscious, we need to get ahold of that experience and process it to the point that we have a sense that we can bear it. At that point we can get to a sense that we can live through it or we have lived through it, it is behind us, and we could live through it again if it were to happen again. Also, when we can tolerate the experience, it becomes possible to stay with the experience without shutting the brain and body physiology down. That way we can process the experience more optimally, not only emotionally but also cognitively and behaviorally. As we saw in chapter 6 on cognition, emotion, and behavior, the more unencumbered the physiology of the brain and body, the more functional all three can be.
How Undoing of Physiological Defenses against Emotions and Expanding the Emotional Experience in the Physiology Make It Easier to Process Unresolved Emotional Experiences
The primary reason we use psychological and physiological defenses against emotions is because they are painful. Even when we are defending against pleasant emotions such as love and power, as well as unacceptable cognitions and behaviors, we do so because of emotional consequences that we expect to be unpleasant. Emotional experiences are painful because of the levels of physiological dysregulation and stress that define them. To work with unresolved emotions contributing to our symptoms in therapy, we often need to make them conscious to begin with. That usually involves looking at the details of the situations in which they arise, working to undo the psychological and physiological defenses in their way, and providing the necessary external understanding, validation, and support to experience them for as long as might be necessary.
What we are asking of ourselves and those we are trying to help is to meet the necessary suffering of their unresolved emotions in the short run in order to reduce the unnecessary suffering from their symptoms in the long run. In the short run, that means we are increasing the level of dysregulation, stress, and distress in the physiology that define the unpleasant emotional experience.
No one likes to suffer if they can help it. I can personally vouch for that. So when we work with unresolved emotions that contribute to our symptoms, we are trying to push a boulder uphill. We are trying to increase the level of inherently painful physiological dysregulation, increasing distress in the physiology. We are, in short, asking for trouble. Psychological and physiological defenses can be expected to kick in and push the boulder downhill, countering our efforts to deepen the emotional experience toward its resolution. The physiological defenses that are engaged, to the extent that they inhibit the vital regulatory flows, will also subject the physiology to additional dysregulation, stress, and distress, even if it might appear on the level of conscious experience that there is some relief from the distress resulting from the attempt to reduce the unpleasant emotional experience through the defenses.
When we work to reduce physiological defenses against emotions that are adding to dysregulation in the physiology, and we are at the same time engaged in generating unpleasant emotional experiences in the same physiology, we are in effect reducing one source of dysregulation, discomfort, and distress in a person’s experience. The more places in the physiology we remove the physiological defenses that are disrupting the vital regulatory flows, the less they contribute to the dysregulation, discomfort, and distress in accessing the unpleasant emotional experience, and the greater the person’s ability to tolerate the expansion of the emotional experience in the physiology, even when it is painful.
This is one way in which emotional embodiment work increases affect tolerance (the ability to tolerate an emotional experience over a longer period). It can be likened to the experience of a person whose arms are being pulled in opposite directions. If one side stops pulling, the suffering would immediately be a lot less. We can verify this for ourselves next time we are having a painful physical or emotional experience. If we turn inward, we can find the pain as well as a felt sense of resistance to the pain. By simply saying to ourselves that we accept the pain for what it is, we can surprise ourselves with a drop in the level of suffering compared to just a moment ago. In moments of suffering, I try to remember and practice to the best of my ability (often unsuccessfully!) the wisdom I lavish upon others by reminding myself of the following statement: the resistance is half the suffering.
Another reason why emotional embodiment work increases affect tolerance has to do with the expansion of the emotional experience to as much of the body as possible. Emotion is an assessment of the impact of a situation on the entirety of the brain and body physiology, especially for overwhelming emotional experiences that motivated a person to resort to psychological and physiological defenses against the experiences at some point. Expanding the impact of a situation, even if it originally affected one part of the physiology more than another, distributes the impact’s burden and makes it more bearable.
As an example, a car hit me on the right side of my body barely a week after I started my first doctoral study at Northwestern University. After the accident, while I was walking I would start to feel fear and unease on the right side of my body when it was exposed to the street. That emotional response would get stuck as a result of the left side of my body bracing along with the right side, as it did during the accident, leaving me anxious and uncomfortable for a long time. For the resolution to happen, the defensive reaction of bracing, which involves constriction of tissue and movement, had to ease so that the vital regulatory flows could carry the information of the impact from the right side to the left side. I resolved the issue by managing to get my fear and unease to spread to my left side. To personally verify this dynamic, next time you are in your dentist’s office getting a shot, try to imagine relaxing your body to let the pain disperse, as opposed to constricting your neck and gripping the chair with your hands, and discover for yourself that it is an easier experience.
There is yet another way in which emotional embodiment work might increase affect tolerance: by increasing the ability of different parts of the physiology to help one another by facilitating the vital regulatory flows among them. It is not uncommon for a physiological defense, such as constriction or numbing in one part of the physiology, to interfere with the exchange of regulatory information between that part and the rest of the physiology, disrupting the regulatory processes between the part and the whole and increasing the level of dysregulation, stress, and distress locally as well as globally. From this perspective, undoing physiological defenses against emotions to integrate and coordinate the functioning of different parts of the physiology by improving the regulatory flows among them could improve one’s ability to tolerate the emotional experience. Such integration could be expected to reduce the level of regulation, stress, and distress throughout the physiology, even as one is trying to process an unpleasant emotional experience.
Energy Psychology’s Take on Why Expanding Emotional Experiences in the Physiology Makes It Easier to Tolerate Them
In energy psychology approaches such as Polarity Therapy, difficulties in accessing and managing psychological experiences such as emotions are theorized to arise from an uneven distribution of quantum or subatomic energies in the brain and body physiology.8 Whether these quantum energies belong to the depths of the physiology or issue from an independent body interacting with it (an assumption in some approaches), all of our experiences, physiological as well as psychological, are believed to arise from these quantum energies stimulating the physiology. When defenses in the quantum energy fields are worked through and the energies are more evenly distributed, there is less dysregulation, stress, and distress throughout the physiology, even when stimulating unpleasant emotional experiences in the physiology. The more even stimulation of the physiology by a more balanced quantum energy pattern distributes the emotional experience more evenly in the physiology, making it more bearable.
Why Unresolved Childhood Experiences Are Harder to Tolerate
A client once sought my help to alleviate her suffering from a constant fear she had had ever since childhood. This fear made her constantly look for a reason for it in her current life and engage in one activity or another to fix it. We used one of the objects of her fear that she identified—that she could die from an illness—to evoke the fear, and then we worked to get her to distribute the fear to more of her physiology until she could tolerate and stay with it. Then she could clearly see that the fear was nothing less than the fear of dying itself. What amazed her was that she could experience it throughout her brain and body physiology and observe that her mind was not spinning to come up with a reason for it or an action to fix it. Given the relative ease with which she could now handle a fear she had suffered from all of her life, she wondered why she had found it hard to fully grasp, let alone to stay with, until then.
After joking that this was because I would not have gotten the credit then, I set about exploring answers to the interesting question: why, every time I succeed in processing an overwhelming childhood emotion, do I find it to be somewhat of an anticlimax?
There is more than one reason for this paradoxical experience of finding that a long-avoided childhood experience is surprisingly not as hard to resolve as one had expected, given a long history of difficulty in resolving it. First, at the time of the experience, the child is less capable of tolerating it because of the child’s immature physiology and psyche, with fewer cognitive and behavioral resources to cope with the experience. The child’s affect tolerance threshold (the intensity of experience they can bear) is rather low, and the defenses that are readily employed are more physiological than psychological. The experience is buried in the unconscious, along with its physiological defenses in tow, to which more psychological defenses get added in later years, and marked as extremely dangerous and intolerable to go anywhere near. So when something now triggers it to the surface of consciousness, the physiological defenses as well as the later psychological defenses tend to engage rather quickly, even before the actual emotional experience is fully out the door. In a way, it is like putting a child in front of a closet door and asking them to open the door, and the child freaks out because they think there is a monster inside the closet. One has to use the adult ego to gently persuade the child ego to open the door and find that the actual experience is not as bad as the child might have imagined it to be.
The second reason why resolution may feel anticlimactic is that what is recalled is not exactly what one might have experienced back then in its original form. For example, no matter how hard I try, I cannot fully recall and reenact in my physiology the awful experiences of nearly dying in my birth and coming close to having cerebral palsy, with my skull crushed and stuck in a birth canal too small for my head, with the umbilical cord wrapped around my head, and with my mother—to whom I was still physiologically connected—on the verge of death herself. It is as though the child ego is expecting and guarding against that original experience, all that terror, fragmentation, and death anxiety, and not the pale symbolic emotional summary of it. So when recalled in the adult physiology in the here and now, it cannot be anywhere as intense, dreadful, or consequential as the child’s original horrible experience, in flesh and blood, on the verge of death. Hence the relief when it is actually finally experienced as a weak version of the original.
The third reason why this type of resolution ends up being not as bad as expected is the predominant use of physiological defenses to guard against primal experiences from childhood, and their activation when we try to access the experience to work with it. They can kick in quickly and cause much disruption to the vital regulatory flows, stirring up a lot of dysregulation, stress, and distress when we actively try to go back to that experience. To use an earlier metaphor, there are more people trying to push the boulder downhill when we are trying to push it uphill. Getting rid of those folks who are well-intentioned but outdated—i.e., getting rid of the physiological defenses—makes it so much easier to move the boulder up the hill. Without the dysregulation, stress, and distress they cause, the emotional experience and its impact can disperse more through the present-day adult and more capable body. This can make the experiences of the watered-down version of the original experience that is behind the defenses more tolerable to be with. It can also get us to a place where we can resolve it successfully, with mastery, while being amazed at how and why it took us so long to get there.
Other Factors That Contribute to Affect Tolerance
We have seen how emotional embodiment can contribute to affect tolerance by decreasing dysregulation, stress, and distress in the processing of unpleasant emotional experiences that are, by definition, states of dysregulation, stress, and distress. Apart from emotional embodiment, there are other factors that contribute to a person’s ability to tolerate emotions. The two most important factors that contribute to affect tolerance are a) the support we have for our emotions from others, and b) our own attitudes toward emotions. Let us look at each briefly.
Emotional support from others: The support one has for one’s emotions from others is perhaps the most important factor determining a person’s ability to experience and tolerate emotions. Research shows that the ability of a child to experience, identify, express, and tolerate a large range of emotional experiences is very highly correlated with corresponding abilities in the child’s primary caregivers.9,10 This can take the form of support from others in the present, or it can take the form of support from others in the past that the individual has internalized.
One’s attitudes toward emotion: A person’s attitude toward an emotion is an important factor in determining the person’s capacity to experience and tolerate the emotion. There can be any number of such attitudes. For example, some people resist unpleasant emotions because they believe it is unhealthy to dwell on them. Some believe men should not show any vulnerability and women should not experience anger. Some people do not understand that unpleasant emotions are inherently difficult to experience because they are states of stress and dysregulation in the brain and the body, and that one has to override the innate resistance to unpleasant emotions to experience and process them for healing to take place. The more educated a person is about the role of emotion in physical and mental health, the more functional the person’s attitude toward emotional experience is likely to be. Please note that the two factors discussed are related to each other. The more support one has for an emotion growing up, the more functional one’s attitudes toward an emotion are likely to be.
Affect Tolerance, Symptom Threshold, Level of Body Expansion, and Formation of Psychophysiological Symptoms
Given the level of support we have for our emotions from others and the functionality of our own attitudes toward emotions, affect tolerance can be imagined as a function of the level of emotion (subjective assessment of whether it is high or low), the level of intensity (subjective difficulty in tolerating emotion), and emotional embodiment, as in the following diagram (figure 8.1). We can also see how symptom threshold, or the level of suffering at which a psychophysiological symptom forms in a person, might be increased and psychophysiological symptoms might be resolved through emotional embodiment.
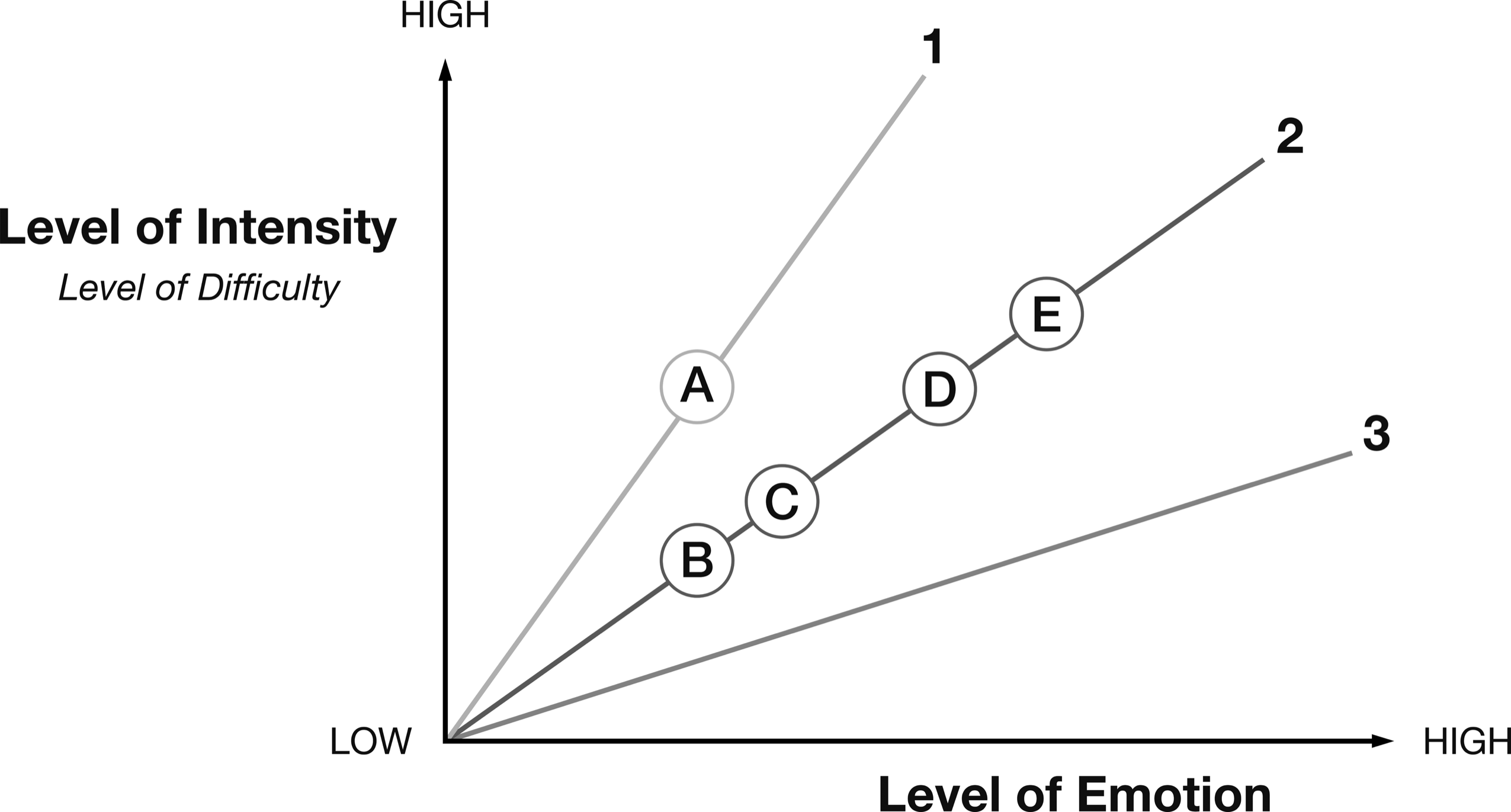
Figure 8-1: Relationship between Affect Tolerance and Emotional Embodiment
Figure 8-1 presents the relationship between the level of emotion (horizontal axis) and the level of intensity (vertical axis) as a function of the level of expansion of emotion in the physiology (lines 1, 2, and 3). Please note that the level of emotion and the level of intensity are not independent of each other. A person is likely to find higher levels of emotion to be more intense.
Lines 1, 2, and 3 represent increasing levels of emotional embodiment or expansion of emotion in the body and brain physiology. In general, the more embodied an emotion, the lower the level of intensity for every level of emotion. Line 1 corresponds to a scenario where emotion is least expanded in the body. Here, every level of emotion is experienced with higher levels of intensity than on lines 2 and 3, which correspond to higher levels of emotional embodiment. Point A refers to the limit or threshold beyond which psychophysiological symptoms form in a part of the body. When the body is expanded by undoing the physiological defenses against emotion to expand the experience of emotion in the physiology, this allows the person’s affect tolerance profile to shift to a flatter line, 2, where every level of emotion is experienced with less intensity than on line 1.
What combinations of level of emotion and intensity of emotion might a person report after emotional embodiment work, on line 2, without forming the psychophysiological symptom? Here are some reports we typically hear from people who go through emotional embodiment work. In one scenario, the person might report the same level of emotion with less intensity overall and in every part of the physiology involved in the expansion of the emotional experience (point B). As we have mentioned before, when you lift the same load with two arms instead of one, both the overall strain and the strain on either arm are less than if one arm were to carry all the weight.
In another scenario, the person might report a higher level of emotional experience with less intensity in all the parts involved (point C). The load is heavier, but there are now two arms instead of one, and both the overall difficulty and the local difficulty in either arm are still lower than before.
Or the person might report a much higher level of emotion than at B and C, but the overall intensity, as well as the local intensity in every part involved in the expansion, might still not exceed the symptom threshold at D. Interestingly, at E the person might report a higher level of emotion and even a higher level of intensity than at D without forming the symptom. How might that be possible? Let us look for the answer in terms of the symptom threshold.
The threshold on line 1 is at A. In the immediate aftermath of emotional embodiment work that moves a person from line 1 to line 2, where is the new symptom threshold likely to be? It would seem that it has to be between B and D, at least in the short run, because the intensity or psychophysiological difficulty in some part of the body and brain physiology cannot be higher than at A, the symptom threshold on line 1.
There is yet another possibility that we run into as an outcome from emotional embodiment work. A person could well end up with a symptom threshold that is even higher on line 2 than point D, point E for instance, if not in the short run then in the long run. What this means is that in the more expanded and regulated brain and body physiology represented by line 2, even combinations of higher levels of emotion and higher levels of intensity, at A or D, might not trigger the psychophysiological symptom. This can happen in the session itself, which can immediately become the basis for a new threshold, such as E on line 2, especially if the client is held at that level for a long time in the session for habituation or imprinting (depending on your theoretical point of view) for the new level of symptom threshold to be established.
Alternatively, the new threshold E on line 2 can be established over time. Just as a person who does weight training is able to lift increasingly more weight over time without injuring any muscles or increasing his or her body weight, the psychophysiology of a person who is doing emotional embodiment work with higher and higher levels of emotion and intensity without forming symptoms can develop the ability to experience higher levels of emotion and higher intensity overall, or in all parts of the physiology involved in the emotional experience, without forming a symptom.
Because the level of intensity or psychophysiological difficulty rises steeply with the level of emotion on lines such as 1, which represent lower levels of expansion and regulation in the body, we can expect people with potentially lower levels of body expansion due to stronger psychological and physiological defenses to have lower symptom thresholds. We can expect people with flatter lines—such as 3, representing abilities to experience higher levels of emotions with relatively lower levels of intensity—to have relatively higher thresholds in terms of combinations of levels of emotion and levels of emotional intensity.
In conclusion, please note that a number of factors, including a person’s environment, might determine how much of the body can be expanded, how much emotion can be generated, and how much a person can tolerate emotional experiences without forming symptoms. We often find that we have shorter fuses when we are with our parents than with our friends, when we are hungry, or when we are sick. A person might have greater capacity for one emotion, such as anger, than for another emotion, such as sadness. So it is important not to think of an individual’s capacity for emotion or affect tolerance as fixed, as though it were independent of the environment or particular emotions.
In the next chapter, we will discuss different types of emotions, some familiar and some unfamiliar, to enlarge our understanding of the range of emotional experiences we are capable of.