Chapter Commentaries for the 2017 Edition
Chapter One: Tina’s World
Ten years is a long time in a child’s life—but a mere instant in the development of a discipline like child psychiatry or the neurosciences. During the decade since the first edition of this book was released, much progress has been made in these fields. Yet systems—and the ideas within them that frame policies, practices, and programs—change far more slowly.
It is estimated, for example, that once a new concept or principle of practice is well established by research, it takes between twenty and thirty years for the “new” ideas to become standard practice. And, as we all know, by that time there is often newer research that suggests modifications and improvements on this “innovation”—and it will take years before these become standard practice, too. The bottom line is that the rate of discovery is faster than the rate at which an organization or system can adapt and incorporate these changes.
We see evidence of this “innovation gap” in all aspects of our life. An important example related to the main challenges that faced Tina and her family is in the early childhood area. For decades, there has been overwhelming economic and developmental research demonstrating the value of high-quality early childhood interventions for “at risk” young families like hers. For every one dollar invested in high-quality early childhood programs like preschool and support for new parents, nine are returned in terms of improved academic performance, better employment, and reduced addiction, mental illness, and crime—yet we still do not provide high-quality, affordable preschool, paid family leave, and adequate support for vulnerable families. Sadly, if anything our public systems like child mental health, child welfare, juvenile justice, and education are slower to change than other organizations such as those in the corporate sector.
Over these last ten years, The ChildTrauma Academy has been working to close its “innovation gap” in several areas. One of the most important relates to the conceptualization of “therapy.” In the twenty-five years since I worked with Tina, my understanding of therapy and the therapeutic interaction has changed dramatically.
During our work, as we challenged ourselves to better understand these children, we kept asking: what is a meaningful therapeutic interaction? How long should that interaction be? Fifty minutes? Ten minutes? Two seconds? Does the “dosing schedule” of therapy—and the supposed therapeutic interactions—have to be once a week for fifty minutes? Could it be twice a week for thirty minutes or some other variant? What is an effective dose of therapy? Who provides that therapeutic experience? Only a “trained” professional? Or can a parent, coach, friend—or the client herself, in an inner process—provide a therapeutic moment?
And how much time do you need between therapeutic interactions to optimize positive change? How do you “space” the therapeutic doses? Are there specific patterns that lead to more effective change—or is simple regularity enough? And are there specific environments or experiences that interfere with—or enhance—a therapeutic interaction?
Over the last ten years our interest and understanding of these issues has matured. In the last paragraph of “Tina’s World,” we note that an hour a week of therapy was unable to “undo that set of associations,” which were related to her history of being abused. It is more accurate now to re-phrase that comment; therapy does not undo associations. Instead, it creates new associations which, over time, can become the new “default” or “template” for guiding responses to future experiences.
In Tina’s case, if she had been given enough time and opportunity to interact with healthy and attuned men and boys who provided sufficient positive or neutral interactions for a long enough time and in a clear enough pattern, she could have created new default associations about men—and male attributes. The associations created by her early history of sexual abuse would remain, although hopefully over time they would be much less “activated” and their intensity would fade.
The major challenge here is that we know so little about how to dose and schedule therapeutic experiences in order to create this therapeutic change. But study of the brain and how it changes may provide us some clues. These days, the buzzword in neuroscience is “neuroplasticity,” which refers to the capacity of neurons and their networks to be altered by experience.
There are some promising clues to the concept of therapeutic dosing in the study of how new synapses—those connections between neurons that link them into networks—are formed and altered to create or change memories. One of the most studied and most important areas of the neurosciences has to do with what is called Long-term Potentiation (LTP). Basically, this refers to the strengthening of synaptic connections, which occurs in response to a brief pattern of intense stimulation. The resulting cascade of cellular changes following this intense stimulation leads to enduring neuronal changes all the way to the chromosome, altering gene expression. It is widely believed that LTP is an important factor in learning and memory formation.
This has important implications for the dosing of therapy: it suggests that even really short experiences can have a big impact. Indeed, long-term and enduring changes in neural networks can be created by an intense period of stimulation that lasts less than a minute. Synaptic splitting, which is one way these connections can change, can occur in mere seconds of intense stimulation—and if the intense experience is repeated four times within an hour, the change will be maintained long term.
Just as a traumatic experience can alter a life in an instant, so too can a therapeutic encounter. Unfortunately, in order for positive “doses” of interaction to lead to long-term change, much more repetition is needed. Consequently, the pattern and spacing required to ensure long-term maintenance of any therapeutic change is going to require a density of therapeutic interactions that our current mental health model of fifty minutes once a week cannot provide. For children like Tina to truly benefit from therapy, it needs to be embedded in a context of safe and positive interactions.
The good news is that anyone can help with this part of “therapy”—it merely requires being present in social settings and being, well, basically, kind. An attentive, attuned, and responsive person will help create opportunities for a traumatized child to control the dose and pattern of rewiring their trauma-related associations. For people who have been sexually abused, like Tina, just being acknowledged in a supportive, respectful, and non-threatening way aids healing. The more we can provide each other these moments of simple, human connection—even a brief nod or moment of eye contact—the more we’ll be able to help heal those who have suffered traumatic experience.
Chapter Two: For Your Own Good
Today, no one would argue that a three-year-old who witnessed the death of her mother, was slashed and left for dead, then placed in foster care is not at risk for suffering lasting psychological damage. While, thankfully, most children have the capacity to recover, the data suggesting that severe early life stress can have a lifelong impact has only continued to accumulate since this book was first published.
So too has our understanding of the role of sensitization and tolerance in trauma and healing. These are two key processes that alter critical stress response networks in the brain. Sensitization amps up the baseline activity and reactivity of these systems, while tolerance dampens down stress response reactivity. (See Figure 6 at the end of this commentary.) Importantly, there are certain patterns of activation that lead to sensitization and can cause problems, while other patterns lead to tolerance and can build resilience.
Neuroscientists have been studying these phenomena for over 50 years. Their relevance to experiences like drug use, addiction, and pain management have long been obvious, but ten years ago, their importance in understanding the effects of childhood trauma was only beginning to be recognized.
Today, the neurobiology of sensitization and tolerance has taught us a great deal about the crucial roles of pattern and predictability in the development and regulation of our stress response systems. Early life experience sets the template for later life responses—this is true of our stress responses, not just our memories. Changing the average level of activity in stress systems and their responsiveness or reactivity during development can have profound and lingering effects.
The key point here is that some patterns of experience make these systems become more easily activated and more prone to reacting even to small changes—while other patterns help allow these systems to respond more smoothly and with less likelihood of over-reaction. Thus, the decades of neuroscience research that suggest how these mechanisms work can account not only for how and why symptoms can result from potentially traumatic experiences but can also give us essential clues to the healing process.
One of the major advances in the clinical arena over the last ten years is the understanding that some forms of developmental experience—for instance, food and housing insecurity, racial or cultural marginalization, and other stresses often associated with poverty—can result in physiological, emotional, social, and cognitive symptoms similar to those seen following extreme traumatic events, including physical or sexual abuse or exposure to domestic violence.
This has led some in the field to refer to big “T” trauma versus little “t” trauma; we don’t use that language but appreciate the point being made. We prefer to think of both capital “T” and small “t” as examples of “sensitizing” patterns of stress response activation that would result in predictable changes throughout the brain and body.
In neuroscience studies, you can create a sensitized stress response by simply creating uncontrollable, unpredictable exposure to small stressors, which, if experienced only once or twice or if their timing was known in advance, would not be likely to be traumatic for typical people. Many of us have had real-life experience with this, for example, in a workplace where a supervisor is unpredictably shaming, then supportive, then angry. Over time, in this situation, many employees become will become sensitized to the boss’s moods and experience anxiety, intrusive thoughts and worries, particularly a desire to avoid dealing with the person. These are all classic PTSD symptoms, though a bad boss rarely will be awful enough to cause a full-fledged case in an adult with no history of developmental adversity.
This same sensitization—often described as “walking on eggshells”—can happen with foster or adoptive parents when the behaviors of the child are, to the carers, completely unpredictable. Obviously, a child’s tantrum is not considered a “traumatic” event on the scale of witnessing a shooting, yet over time the physiological and psychological effects of many small, uncontrollable stresses can be very similar to those we associate with more extreme experiences.
The pattern and context of stress system activation—i.e., whether it is controllable or not, whether it occurs predictably or not—is as important as the intensity of the activation, and can sometimes be more so. In the real world, this means that a child of color living in poverty with no exposure to abuse, domestic violence, or other overt “trauma” can develop “trauma-related” problems that look just like those seen in a child who witnessed a shooting or lived through a natural disaster. And, if children like this also have exposure to overt major trauma such as community violence, their problems will be compounded.
To explore this further, let’s briefly review the features of the patterns of stress activation that can lead to a less sensitive, less reactive stress response capacity. As we’ve seen, the majority of physical, emotional, behavioral, social, and cognitive problems related to developmental trauma can be linked to changes in the pervasive, widely-distributed neural networks involved in responding to stressors. We’ve seen as well that neural networks are “plastic”—capable of changing. So what does research in the area of neuroplasticity tell us about how to change these systems?
The first and primary principle of neuroplasticity is that in order to intentionally modify—in any way—a specific neural network, we must first “activate” (or, in some cases “deactivate”) that specific neural network. This of course seems obvious; in order to learn how to play the piano, one must sit at the piano and play. Reading a book or watching a YouTube video about playing piano won’t change the specific neural networks responsible for piano playing. Your time at the piano may benefit from what you can learn in a book or video, but you will not create or modify the widely-distributed neural network that allows “piano playing” unless you activate it fully by actually tickling the ivories.
The same is true for traumatic memory and the sensitized stress response networks that are yoked to the complex, widely-distributed trauma reaction that follows the traumatic event. For Sandy, her set of trauma memories were reinforced and strengthened each time an evocative cue activated this chain: for example, when she did something as simple as drink milk. The vast majority of these activations for the first years following her mother’s murder were unpredictable to her because she didn’t know when to expect them. As a result, her stress response systems became more and more sensitized, and she often experienced an extreme and prolonged response. And as a result of that, she got worse.
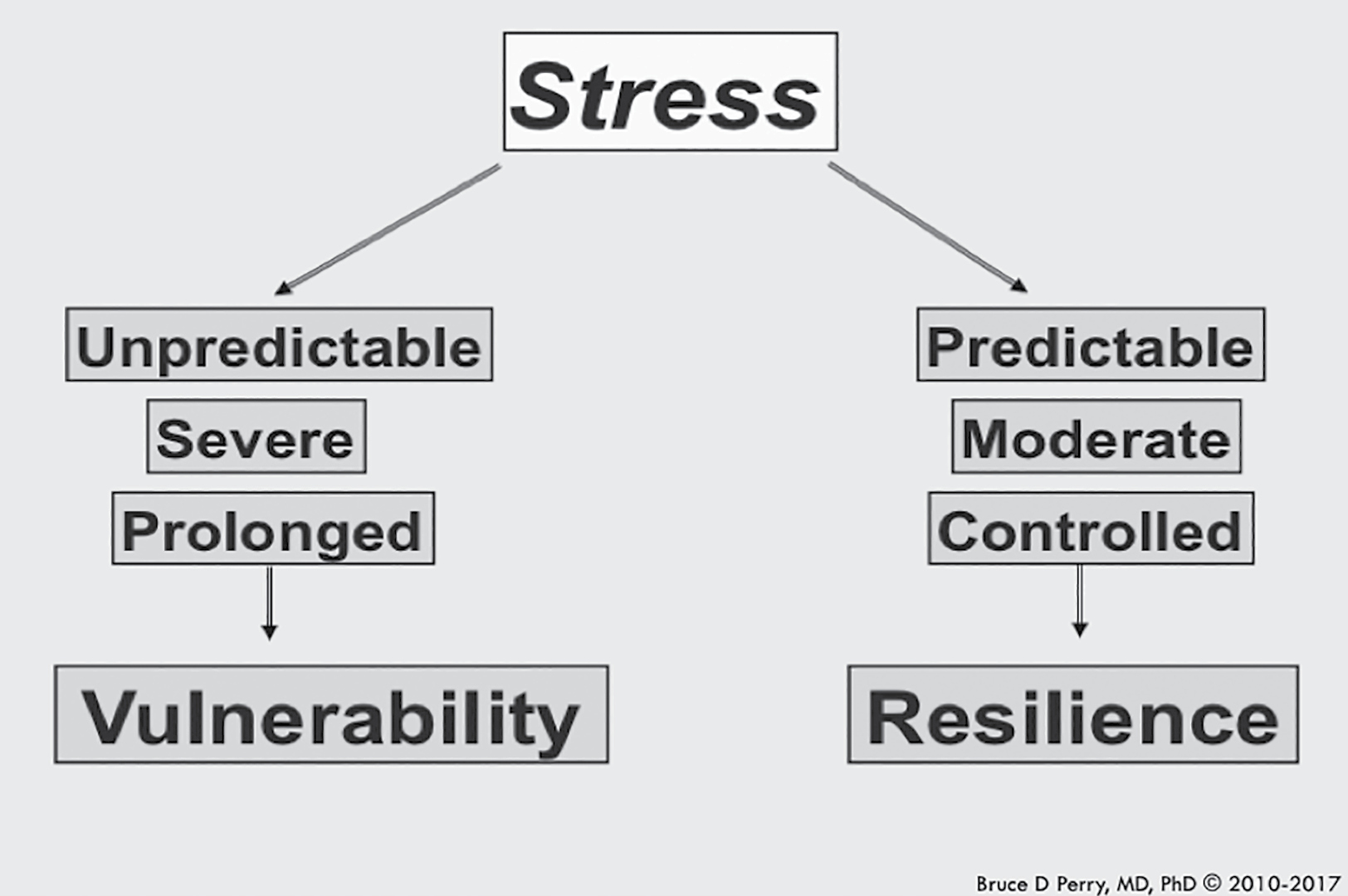
A major challenge of doing therapy when trauma and sensitized stress responses are involved is that the principle of specificity has to be applied in order to change the sensitized stress response systems; healing involves the process of “revisiting” and “reactivating” very painful experiences in some way. The key to effective healing and therapeutic work is paying attention to the three essential elements of the resilience-building and healing pattern of stress activation. These are predictability, controllability, and moderation.
What we’ve learned about these factors since we first wrote this book relates back to the concept of “dosing.” What is a moderate dose of revisiting a trauma and reactivating a chain of traumatic memory? Who determines what is moderate? Should it be the clinician who asks the child to recount the traumatic event—or the child?
When we ask a child to come to our office once a week for a 50-minute dose of revisiting, doesn’t that, in itself, take control away from him or her? Can we create safe and regulated settings for children to control the dose, space, and pattern of their healing journeys? In Sandy’s case, during our therapy, she could go back to these dark times, spend some moments living with the pain of the reactivated trauma memory—but she also could control her own disengagement, so she could regulate herself before revisiting the experience.
She controlled what parts of that experience she would reactivate and reenact—this provided controllability. She also decided for herself how long she would stay there—this controlled the dosage. She determined how much time would pass before she would revisit those experiences, which controlled the spacing of the experience. In our sessions, she allowed herself to activate some component of her pervasive trauma memory, and then created controllable, predictable, and moderate activation of her sensitized stress response systems. Over time, this led to a less reactive system, a shift in symptoms, and some degree of healing.
We cannot emphasize enough how important it is for traumatized children to be given the most possible control, predictability, and ability to moderate the timing, duration, and intensity of their experiences. They need these elements to be maximized, not just in therapy—but in the rest of their lives, particularly places where they spend a lot of time, like school. To become resilient, children need environments where they feel safe and comfortable, and know what to expect so that their sensitized, overreactive stress systems can gradually become calmer, and more “smoothly” regulated.
(The chart below illustrates the key principles here).
Chapter Three: Stairway to Heaven
Almost twenty-five years have passed since the disastrous raid on David Koresh’s Ranch Apocalypse in Waco, Texas, and in that time, our understanding of how threat and fear affect both groups and individuals has evolved.
Specifically, we have learned much more about the importance of relationships within a group to create opportunities for development and healing—or to do the opposite. Increasingly, we’re realizing that the health of the group can have a large effect on the health of an individual.
As we’ve seen, perceived threat and fear will change the way the brain works in any given situation. In general, when people feel threatened, key networks in the cortex will shut down: specifically, the regions involved in reasoning, planning, and other complex thinking. This allows rapid action in emergencies, but is obviously not the state of mind you want to have when you are in class or studying for a test (see Appendix, Figure 3).
In fact, all of the functions of the brain—learning, thinking, feeling, moving, regulating hormones and other chemicals—are “state-dependent.” This means they will change with our physical, and importantly here, emotional states and experiences.
The consequences are profound: a child in a state of fear will have a difficult time learning anything, even physical activities, like sports. And children’s behaviors will reflect their emotional state: during fear, they are primed to fight, freeze, or flee, as we have seen.
But as we discuss in much greater depth in our second book, Born for Love, groups also respond to situations in a state-dependent manner (see Appendix, Figure 5). Human beings are social creatures, and our individual neurobiology and body physiology are influenced by those around us. The moods and actions of those around us are contagious—especially those of the perceived “leader” of the group. This has countless implications: the most relevant of these for working with traumatized, maltreated, and fearful children is that the “helping” adults cannot teach children to regulate their emotions and behaviors unless they themselves are in an emotionally calm and reasonably well-regulated state.
Just like dogs, all humans, especially traumatized children, can sense fear and anxiety—so self-care for those who work with maltreated children is essential for effective therapy. Front line workers—or parents, teachers, or caregivers—who are themselves being poorly treated by supervisors or others in power can inadvertently pass their distress down to these vulnerable children.
This means that a demoralized, disrespected, and overworked clinician will have a hard time being effective. An underpaid, micro-managed teacher will be less likely to inspire learning, and an overwhelmed, anxious and exhausted foster carer will be less capable of being present, nurturing, and regulating. (Sandra Bloom’s Sanctuary Model, which helps organizations prioritize this insight, is among the best I’ve seen. For those who would like to help leadership implement relevant changes, see Sanctuaryweb.com for more information.)
Another major change in the field in the past decade is the increased awareness of the “Adverse Childhood Experiences (ACEs)” epidemiological studies. As we mention throughout the book, developmental adversity impacts the entire body—not just the brain. The first ACE study, which looked at the current health of 17,000 adults, was led by Robert Anda of the Centers for Disease Control and Vince Felitti of Kaiser Permanente in California. They began publishing results in 1998. The basic findings were stunning: as the number of ACEs increased, so did the risk for everything from heart disease, stroke, and obesity to addictions and depression in adult life. (We discuss this work throughout the book; for more on the specifics of this research, see Chapter Seven in Born for Love). Despite the importance and power of these findings, a twenty-year “innovation gap” followed. Only within the past five years have these important studies begun to have widespread impact on practice and policy.
These and similar findings have led to an explosion of “trauma-informed” practices in education, juvenile justice, mental health, child protection, and even in neighborhoods. This has been heartening and there are many programs that have truly made a difference in children’s lives.
At the same time, unfortunately, as with all large-scale shifts of focus in society, especially when people recognize that there is money to be made, there is a lot of chaff with the wheat. Self-declared experts arise with packages of programs allowing systems to “check the box” about being “trauma-informed.” Over time, this will settle out, and we remain hopeful that the ultimate result will be positive.
In the meantime, appreciating how state-dependence plays out in organizations can be useful in understanding some of the challenges we face when attempting to make positive changes in practice, programs, and policy in any organization or system (see Appendix, Figure 5).
Chapter Four: Skin Hunger
Over the years, I have been asked about almost all of the individual children we discuss in the book. Sometimes people want an update; often someone will identify closely with one of these children; some people describe sharing similar symptoms and feel relieved to understand a bit more about themselves. Clinicians, too, will share that they had similar challenges or point out where I neglected to mention a key issue, which was frequent, owing to both my own limitations and those inherent in writing about very complex clinical situations. And some people even have offered to foster or adopt one of these children.
The comments and queries vary; by far, however, the most frequent questions are about Mama P. Can I just meet Mama P. ? Does she live in Texas? Does she still take in children? I think I know Mama P.
We all should have a Mama P. in our lives. The wonderful qualities of Mama P.—her patience, strength, wisdom, and capacity for love—made her a special and powerful healer, and as a long-time leader in the foster care community, a key part of the child welfare system where she lives. Nonetheless, I must keep her personal information private.
I started my adult psychiatry residency at Yale in 1984. Since then, the nature of child welfare in the United States has shifted dramatically. One major change has been in the way children and families are served by the child welfare system. With a new emphasis on finding “forever families” for children, the system has focused increasingly on getting children into permanent guardianship—often with someone in their extended family, like an aunt or grandparent—or adoption. From the perspective of child trauma, this is a positive trend, but, as with everything else involving human systems, the shift has not occurred without raising a different set of problems.
In the US, the responsibility for funding and carrying out child welfare services such as investigation, removing children from homes deemed unsafe, placing children in foster homes, shelters, kinship homes, and funding some level of evaluation and needed medical and mental health services falls to the state. Each individual state will choose how to do this: some states delegate the majority of these responsibilities to counties and provide some organizational oversight and funding, while other states have a system that is unified at the state level.
In all cases, the federal government provides some funding for these agencies. Title IV-E is a federal program that will reimburse states for some of the cost of providing foster care, adoption assistance, and kinship guardianship assistance on behalf of each child who meets federal eligibility criteria. Not all children who require care from Child Protective Services do meet these criteria, so generally speaking IV-E-funded cases are an underestimate of the actual numbers of children served by the states. Nonetheless, the shifts in Title IV-E-funded cases from 1984 through to 2013 indicate the dramatic change in the focus of child welfare resources.
In 1984, there were 102,100 children in “out of home” or substitute care—in other words, foster care or kinship care—funded by Federal IV-E funding. There were 11,600 children in IV-E adoption or guardianship homes. Thus, just 10% of the total funded cases were in permanent placements. But by 2001, 49%—and by 2013 74%—of the IV-E-funded children were adopted or with permanent guardians. In 2015, roughly 430,000 children were in foster care (both IV-E- and non-IV-E-supported), and at least 500,000 were in IV-E-supported permanent adoptive or guardianship homes.
So why does this shift in IV-E-funded cases matter? This entire book is about the impact that developmental trauma, neglect, attachment disruptions, and related childhood adversity can have on the child. And we know that the rates of significant emotional, behavioral, social, and cognitive problems in children removed from their homes can reach up to 70%, if not more, over time. The number of children in need grows; the problems related to their developmental trauma don’t disappear when they enter a “forever home.”
Over time, the burden of dealing with these children’s complex problems has shifted to the families providing elements of permanence for these children: kin and adoptive carers. But the child welfare system has not caught up enough (remember the “innovation gap”) to develop high quality “developmentally-informed” and “trauma-sensitive” resources for these families or for the foster families that care for hundreds of thousands of these children each year. We are simply shifting the problems from one system to another.
If only there were 430,000 Mama P.’s available to provide the individualized, nurturing care that the 430,000 children in foster care require—and deserve. If only the half a million children in permanent or adoptive care had caregivers who understood the complexities of developmental trauma. Unfortunately, the foster care systems in most states struggle to get qualified homes—and when they do recruit a family, the amount of education provided about development, trauma, attachment, and the various challenges these children face is minimal. Most carers are self-taught with all of the potential benefits and pitfalls that can bring. In general, many of our foster and adoptive carers are overwhelmed by the needs and challenges of these children, and many tend to be poorly equipped or supported to deal with the range of complex problems that these children often have.
On top of that, schools are even less capable of being supportive of the foster family’s efforts, often ignoring good input from the foster or adoptive parent and implementing practices such as suspension, expulsion, seclusion, and restraint. All of these measures simply make things worse for the child and the family.
Then, there is the medical community—who should know more about all of these issues—who are viewed as the experts by schools, families, and, all too often, themselves. The medical community—including psychiatry—can be as trauma-and-development-ignorant as any other. Over the last ten years, this has not changed much, unfortunately.
And one area where this ignorance is especially tragic is in the inappropriate and harmful use of medications. If anything, this has become worse over the last ten years. Irrational psychopharmacology—where doctors prescribe medications for which there is no evidence of effectiveness or actual evidence that the medication does not work—has exploded. So has the use of multiple medications, or poly-pharmacy, even though there is rarely any evidence related to whether or not it helps.
Foster children are much more likely than other children with similar problems to be prescribed multiple medications that will have no impact on their symptoms. These medications, particularly the so-called atypical antipsychotics (medications like Risperdal, Abilify, and Seroquel) can shorten life and have severe side effects, like weight gain great enough to increase risk for diabetes.
The over prescribing and inappropriate prescribing of such medications to children in foster care has been so dramatic that the Government Accountability Office has issued a special report condemning it. Both the federal government and several states have sued Big Pharma for targeting foster care children, resulting in multi-million-dollar settlements.
In the last few years, attention to these issues by legal groups, such as the National Center for Youth Law in Oakland, the press (an excellent example can be seen in the online series from the Mercury News by Karen de Sa), and advocacy groups such as Foster Youth in Action, has increased awareness of this problem. These investigations and advocacy are leading to some positive changes. For example, California passed legislation to monitor prescribing to children in foster care.
But sadly, rather than joining in or even leading efforts to improve the quality of care for foster and adopted youth, most medical and psychiatric groups have resisted or even openly opposed these efforts. Change is hard, and it is hardest for those with the most to lose. As Annette Jackson and I wrote in 2014, “the academic or interest group most threatened by the innovations which challenge their existing frame of reference or perspective, will be the most vocal and hostile to the new ideas.” Nevertheless, we persist.
Chapter Five: The Coldest Heart
Looking back at this chapter, I laughed—and blushed—at the arrogance of our last sentence. We are still nowhere near unlocking the secrets of the brain, and, if anything, advances in the developmental and social neurosciences have added complexities that we didn’t even know about ten years ago. It’s that “the more we learn, the less we know” thing. We are still far from understanding complex cases of sociopathy like Leon’s.
In addition, we are learning that the quality of the genetics, neurochemistry, and neuroimaging studies that have examined human psychiatric conditions like sociopathy are woefully inadequate and may be essentially uninterpretable: too often, they have inadequate sample sizes, poor characterizations of the population studied—and of course, they use DSM labels, which, as we’ve seen, are deeply problematic.
As a field, we have spent a lot of time and money getting, well, not too far, in understanding the complexities of brain development and its effect on behavior. With all of that said, we are still actually making progress.
As we slowly increase our understanding of development, the brain, and humankind, there will always be a gap between what we are learning and what we can actually apply. Right now, that chasm seems especially large—but it is often darkest just before dawn.
Sometimes, of course, we create practices, programs, and policy based on “what we know” only to learn later that this “understanding” was immature or even wrong. Psychiatry has far too many examples of this: the frontal lobotomy, ice-cold baths, and insulin-induced shock are only the low lights. The area of what is now known as “translational medicine” is intended to take what is being discovered in basic sciences and develop practical applications of those discoveries. The concept is good; the application part has been challenging, and this occurs at least in part both because of the “innovation gap” and the tendency of those who benefit from the existing approaches to push back when “translational” innovations emerge.
Our working group has always been at the interface between discovery and application; we have attempted to bring advances in the neurosciences—and related disciplines—into clinical practice, education, and caregiving. This requires “translating” complex facts, principles, and concepts into a language that is clear and understandable. A key problem is that things really do get lost in translation. Due to the abundance of facts in the neurosciences, we often choose to teach concepts or general principles when we communicate to non-neuroscientists; we use shorthand and teaching devices to illustrate the key concepts, such as the images and tables included in the Appendix.
But for each principle, there are often important exceptions to the rule.
And simplification often includes hidden distortions that can lead to false conclusions when people try to generalize from it. An attempt to teach about the explosive rate of development in utero and in the first years of life, for example, can get turned into “Dr. Perry says it’s too late to change the brain after age three.”
Another example of this over the last ten years has been seen in the emerging “trauma-informed” world. The phrases “the amygdala hijacks the brain” and “an amygdala storm” have become common language amongst the “trauma-informed.” The attempt to teach a little about the neurobiology of threat interpretation and how fear alters the way we process and act on information gets turned into a distorting buzz phrase.
Unfortunately, people like simple explanations such as “The amygdala is the ‘fear center’” and a child’s meltdown is an “amygdala hijacking.” Misunderstandings and distortion about the complex functioning of the amygdala in processing and interpreting fear-related cues became so pervasive that Joseph LeDoux, the pioneer in study of the amygdala and fear, and the person typically cited when the “amygdala storm” language is used, finally wrote a blog entry about it. It was titled “The Amygdala Is NOT the Brain’s Fear Center.” Indeed, this region is involved in many different emotions and the complexity of the brain means that phrases like “hijacking” often incorrectly reduce complex human behaviors into the actions of will-less zombies.
Translational work has implications for policy and practice outside of clinical settings. The legal system, for example, has been using neuroscience and developmental trauma research in a variety of ways. Cognitive impairment and obvious mental illnesses—both neurobiological conditions—have always been taken into consideration in determining guilt and sentencing. In recent landmark cases, including two Supreme Court cases, the role of the “immature adolescent cortex” in judgment and impulsivity has been cited in modifying sentencing guidelines related to the death penalty and life without parole; neither sentence can now be used with adolescents. The ChildTrauma Academy has been involved in educating the courts and the juvenile justice system about the neurobiology of trauma, the role of trauma in the development of violent behaviors, the impact of seclusion and solitary confinement, the effects of indiscriminate use of shackles on youth in court, and especially, the creation of trauma-aware and trauma-sensitive practices in juvenile justice settings.
Unfortunately, the legal system is also vulnerable to the “mistranslations” or distorted interpretations of work on trauma and development. On numerous occasions, I have been asked to become an expert witness to give testimony about the impact that a given experience has had on a person; this is a significant area in civil (not criminal) litigation, seeking to prove “damages” following some event or injury. Sometimes the event is clearly traumatic. For example, an employee is seriously injured in an explosion at a factory that also kills several co-workers and the effects are obvious: sleep problems, anxiety, cue-specific panic, avoidant behaviors.
In other cases, the legal team will try to convince me that an adolescent living in a household with documented history of domestic violence was instead “traumatized” by a hostile teacher and that his impulsive and aggressive behaviors all stem from this teacher’s “abusive” practices, such as giving him a “0” on a homework assignment that he forgot to bring in.
I don’t do very much forensic work, and when I do, I try to pick cases where I think I can learn something—and Leon’s case was, in fact, one of these. Over the last ten years, research has confirmed that people convicted of violent crimes, like Leon, have astoundingly high rates of early life attachment disruption and chronic developmental trauma, especially exposure to violence. These findings have lead to efforts to create a “trauma-aware” judiciary and “trauma-informed” juvenile justice and criminal justice programs—in prisons and probation. True rehabilitation will not be possible without awareness of the multiple complex effects of trauma, neglect, poverty, racism, and other developmental adversities. Addressing recidivism and successful re-entry to the community is impossible without a respectful, humane, and developmentally-informed, trauma-aware perspective.
“Translation” matters. It does help the people in these systems better understand these children, youth, and families, and this can truly help improve our systems. And, no matter how often our efforts at translation get twisted, we can’t give up. Connect, correct, clarify, and carry on.
Chapter Six: The Boy Who Was Raised as a Dog
Both Justin and Connor experienced severe early neglect, as well as other traumatic stressors that profoundly affected their development. For Justin, having been raised in a kennel with much canine, but little human contact, was obviously not a normal upbringing; Connor, who was simply left alone all day during the work week for his first 18 months by a negligent nanny also suffered enduring problems.
It’s pretty much inevitable for people who are trained to be doctors—and psychiatrists particularly—to focus on pathology when we meet children like Justin and Connor. How do we identify and measure their deficits? What can we do to understand the causes of their problems? What are the mechanisms that led to these specific difficulties, and bearing these in mind, what can we do to try to help?
This chapter was written with that general frame of reference. Ten years on, however, I have become much more focused on the strength and resilience demonstrated by children like Connor and Justin in the face of such dramatic and devastating experiences. Most importantly, I want to know why they were able to make such rapid progress while other children with similar symptoms and seemingly similar abuse and neglect do not. The key word here turns out to be “seemingly.”
If the children in this book tell us anything, it is: “Listen closely and look carefully at my life story.” Unfortunately, in medicine, we are notoriously “bad listeners” and are often poor observers. It takes time to gather a complete and thorough developmental history—certainly much more time than a typical initial assessment visit to most clinics allows. Multiple sources of “patient history” are required to fill in the gaps. These include medical and educational records, conversations with parents, teachers, previous mental health providers, and more. All of these take time and money to gather. And even if you do all of this, if you don’t ask and don’t look for the presence of critical experiences that influence development, you won’t find them.
Systematic evaluation for a history of developmental trauma (or adverse childhood experience, ACE) is only now becoming a routine component of a mental health evaluation—and this is a significant advance. Still, it is rarely included in typical pediatric visits—despite the fact that we know this is a major risk factor for physical health problems such as asthma, diabetes, and cardiovascular risk. As discussed throughout the book, the timing and nature of developmental trauma matters. As we developed our NMT assessment process, we realized it was essential to quantify the nature, severity, and timing of an individual’s developmental trauma. But does this allow us to “look carefully” enough?
As we mention in this chapter, these two boys had two things in common: early neglect and a good response to developmentally-appropriate intervention. Closer examination of their histories gives us some clues to why they were so responsive to treatment. Despite his years of neglect, Justin did have positive relational connections in his first year of life, before his primary caregiver, his grandmother, died. Once he started living in the kennel, he also did have the warm physical contact and unconditional love that so many of us get from dogs, albeit in more typical situations.
In Connor’s case, he had normal and healthy loving parenting for the first eight weeks of his life—along with ongoing “booster” touch and connection in the evenings and weekends throughout the time he was neglected. Both of these boys had an abnormal but partial history of positive relational interactions in the first years of life. Even fragmented positive interactions were protective.
“Listening closely and looking carefully” means that we need to quantify children’s “relational health”—in other words, the nature, number, quality, and timing of their relational connections, what we might call their overall “social connectedness.” Social connectedness refers to the quality and number of connections an individual has with family, friends, and acquaintances: it is a key component of community and cultural cohesiveness. As we discuss in depth in our second book, Born for Love, this connectedness is a major factor in both individual and community health.
As we worked to develop the NMT, we created a process to measure the timing and severity of adversity such as abuse and neglect—as well as the timing and intensity of “social connectedness,” which includes the strength of the child’s connection to healthy aspects of family, community, and culture.
The “balance” between the scores on the adversity measure and the relational health measure gives us a more accurate estimate of true “developmental risk”—in other words, a child with a strong network of social connectedness is at far less risk from a potentially traumatic experience than a child without such support would be.
Over the last six years, The ChildTrauma Academy’s network of clinical partners has systematically evaluated over 30,000 children, youth, and adults using these adversity and relational health measures. We also looked at the current emotional, social, behavioral, and cognitive functioning of these 30,000 individuals.
What we learned included some significant surprises. The first and most important of these is that relational health measures are more predictive of outcomes than adverse developmental experiences are. In other words, having a strong social network with many, high quality relational interactions over time predicts good mental health and other positive outcomes better than traumatic experiences predict poor prospects. Relational connectedness buffers current distress and helps heal past trauma.
That’s not to say that developmental adversity doesn’t do serious harm—it certainly can. But strong relational health can help protect children from lasting damage connected to these experiences and is essential to their resilience. Consequently, if you want to predict someone’s mental health and functioning based on their childhood experiences, looking at positive social factors will actually tell you more than focusing exclusively on trauma. If there is trauma, good social supports can actually counteract the harm that has occurred.
This observation has profound implications. For one, it’s consistent with data on population and community health, which shows that social support is critical for health and that communities lacking healthy social ties tend to be wracked by problems like diabetes, heart disease, obesity, and addictions. These findings are also in line with research on resilience, which again, links it to social ties and healthy support. Finally, it suggests important and practical intervention and prevention strategies, such as measures that aid school and community connection, programs to support and connect parents, and basically anything that helps people make friends and nurture families.
Our research also confirmed that the timing of developmental risk does make a significant difference in outcomes. In twelve-year-old children, for example, having been maltreated in the absence of social buffering during the first year of life—and then being in a much healthier and safer environment for the next eleven years—led to worse outcomes than the reverse; i.e., where the child was healthy and safe in the first year, but not for the next eleven! In this case, the first year of good experience helped “inoculate” against the eleven years of adversity—but unfortunately, a bad first year was really tough to overcome, even with eleven years of safe and positive experience.
This pattern is consistent with what we know about brain development, so much of which occurs in the first few years. It’s also consistent with the large impact of high quality home visitation models like Healthy Families America and Nurse-Family Partnership, which involves nurses visiting and regularly supporting first-time moms during pregnancy and the first year of a child’s life. These programs have been shown to improve academic achievement and cut crime and addiction later in life. Nonetheless, seeing these large effects of early experience come out so strongly in our data is sobering.
Currently the public systems we have to identify and help the most isolated, marginalized, struggling young families—and their infants—are under-resourced and ill-equipped to meet the demands. As our society struggles with the myriad problems related to childhood trauma, developmental adversity, and relational poverty, it will be essential to infuse the problem-solving process with well-interpreted, quality data. If we don’t learn from these children and families—if we don’t systematically “listen closely and look carefully”—we will all lose out.
Chapter Seven: Satanic Panic
Starting with our work treating the children of the Branch Davidians in 1993, The ChildTrauma Academy has had a good relationship with the Texas agency that oversees Child Protective Services (CPS) in that state.
The leadership knew me, they had come to trust our work, and they frequently asked for input about ongoing program or practice issues. We, in turn, learned more about the challenges facing individual caseworkers and the CPS system as a whole. It was very tough work; individual workers and supervisors faced high workloads, emotionally wrenching situations, frequent high-conflict interactions with family members or attorneys, and, all too often, not a lot of support or clinical supervision.
Furthermore, the natural emotional contagion that occurs between humans makes proximity to continuous traumatic situations a perfect setup for “secondary” traumatic stress, with all of the anxiety, sleep problems, depression, irritability, and demoralization that can go with it. This combination leads to a depleted and burned out CPS workforce.
Unfortunately, the solution for many caseworkers is to quit. During the time we worked with CPS in Texas, it was typical for one third of the new caseworkers to quit within the first year. Those who stay have to try to stay regulated—and keep good control over how they manage stress. Of course, there are healthy and unhealthy ways to regulate yourself. Healthy ways include working out, keeping good boundaries between work and home, connecting with colleagues and friends on a regular basis for support and just for fun, taking adequate time away from work, and more.
Unhealthy ways, of course, include disengaging or even dissociating and sleep walking through the work, or trying to self-regulate with food, cigarettes, alcohol, or other drugs. This continues to be one of the major challenges of most CPS systems; adequate training, ongoing support and quality clinical supervision are needed to help all staff manage this important but often distressing work.
In the case of Texas, CPS responded to these problems, in part, by issuing a grant for crisis intervention and debriefing to follow obviously severe incidents like what happened in Waco, in Gilmer as described in this chapter, and other cases of severe child injuries or deaths. Each year for over ten years, The ChildTrauma Academy was awarded this grant; our program proposal was always called “Crisis Intervention and Secondary Trauma Prevention.”
It involved a reactive set of program activities, such as going into Gilmer to meet with the caseworkers, children, families, and other personnel involved and providing consultation and recommendations. It also included a set of proactive program activities, like providing a curriculum on trauma, neglect, and secondary trauma for caseworker training and ongoing professional development. We felt very strongly that if the caseworkers were better trained about trauma and related issues, they would be less vulnerable to secondary trauma and more effective in their work.
In other words, we would have less need to have expensive after-the-fact interventions if we had more proactive program elements ahead of time. And yet, every year we had that grant, the Crisis Intervention component was funded and the preventative proactive component was defunded. Following event after event, we would give feedback about the practice, program, and policy actions that would prevent such events—such as the panic that occurred in Gilmer and the resulting custody cases and trauma—and every year our recommendations were disregarded and tucked away in someone’s file cabinet. It was frustrating.
The importance of self-care in effective child welfare work was just getting lip-service. Further, the crucial insight and support that frontline workers need to better understand these children—and themselves—was not being provided. Texas officials would listen to us when they were in the midst of a crisis—like in April 2008, when they asked us to lead the mental health and assessment process after the removal of 439 children from the Yearning for Zion (YFZ) Ranch run by the Fundamentalist Church of Jesus Christ of Latter-Day Saints (FLDS) in Central Texas. The FLDS is a polygamist sect led by “prophet” Warren Jeffs. Claims had been made that children being raised in the group were being sexually abused.
That was a pretty complex—and often surreal—situation, but that’s a whole other book. Seriously, it is. Maia wrote a book with one of the key witnesses in that situation, Brent Jeffs, who is the nephew of Warren and whose account of having been sexually abused in the church by his uncle set off the series of events that led to the raid. (It’s called Lost Boy.)
In any case, Texas CPS leadership changed, and I started to feel that we were becoming part of the problem by simply rolling over every year when the proactive part of the grant was defunded. They wanted our help in crisis but didn’t want to listen to our input about how to prevent these catastrophes. By 2009, we were actively involved with child welfare systems in other states; when the call for proposals for the Texas grant came along, we didn’t apply. We were learning more about systemic change—and despite our best efforts, that Crisis Intervention and Secondary Trauma Prevention project wasn’t changing the child welfare system in Texas.
So how could we help change systems? All of these extreme and complex situations in the child welfare and mental health system where we were consulted were, to some degree, preventable. Think of each of the children described in this book and their life stories. Whether it is the parent, foster parent, therapist, case-worker, judge, FBI tactical team, pediatrician, teacher, or child psychiatrist, an awareness of the fundamentals of the brain, development, attachment, trauma, and neglect could have diverted or minimized the tragic trajectories of these children. Thus, the relentless focus of The ChildTrauma Academy has been on translation and dissemination of this content over the last thirty years.
We have much to be hopeful about in this area. We have been actively involved in the development and implementation of training and other “capacity building” projects that teach and implement the core concepts of our Neurosequential Model in multiple settings (clinical, school, juvenile justice) and for non-professional caregivers (parents, foster and adoptive parents). Over the last ten years we have developed curricula and related activities to teach these concepts to just about any profession you can think of—physicians and psychologists of all sub-specialties, social workers, nurses, occupational therapists, physical therapists, teachers, judges, parole officers, law enforcement, all the way up to the corporate and business community.
We have developed training, practice, and program elements suitable for dozens of organizations and systems: early childhood settings, schools at all levels, jails (juvenile and adult), courts (family and criminal), and the child welfare, mental health, and juvenile justice systems. As we will describe later, these efforts have exploded over that last ten years.
The most promising projects involve actually embedding these concepts into schools of social work, education, and medical school. When we engage professionals after they have been trained, we are asking them to shift or change their perspective: a big ask. However, when we teach the social work, education, or medical student these concepts up front, this becomes their primary frame of reference; it is much easier for them to immediately understand and implement developmentally-informed and trauma sensitive practices when they enter the field. As we’ve seen over and over, it’s better to start early whenever possible.
Chapter Eight: The Raven
The young woman stood patiently in the background as the group of people slowly dispersed. We had a brief moment of eye contact, both of us smiling. She looked familiar. But I meet so many people—and I’m terrible at remembering names, so I couldn’t place her.
I had just given a public lecture focused on the importance of relationships in shaping our physical and mental health. A small group of people approached me. This woman, however, stood apart, letting everyone else go first. Soon the auditorium was empty, aside from a few members of the organizing committee cleaning up—and an older woman in the very back of the auditorium with two young children.
She stepped forward, clearly anxious. “Do you remember me?”
“You look familiar but you’ll have to remind me… I’m getting old and my memory is shot.” I tried to use humor to hide my embarrassment.
“Funny. You always did joke around.” She rolled up her sleeve and I immediately recognized the raven tattoo.
“Amber. Oh wow. So great to see you.”
And it was. She looked different; older, no obvious piercings and her hair was light brown, almost blonde. She smiled as I asked her to catch me up on her life. We spent the next ten minutes talking and as we did, the older woman and the children walked from the back of the auditorium up to where we were sitting. I could soon see that the woman was Jill, Amber’s mom. When she approached, Jill smiled and we exchanged a few words about how they ended up in this city, which was far from Texas. Amber corralled her children, hugging one in each arm.
“I want you to meet my children,” she said, “This is Tori*. She is seven, and Thomas* is three.” She turned to speak to her children. “This is my friend Dr. Perry. We met a long time ago when I was just a little girl.”
Not so little, I thought. Interesting that she said that—maybe she felt smaller than she was at the time. The children had a moment of obligatory stillness, looked at me—probably trying to imagine “Mom” as a little girl—then wiggled out of Amber’s hug and continued exploring the auditorium under the watchful eyes of Grandma Jill.
It was one of those rare moments in a clinician’s life when you have the opportunity to see how things played out for a patient. She’d had had her ups and downs, but for now, was in a healthy relationship with the children’s father. They lived together, but had decided to not marry. Jill lived nearby and often helped out with the children. Amber had decided initially to become a social worker and had a brief spell working in child welfare, but she found it “too triggering.” She now worked with a non-profit faith-based organization supporting refugee families.
This clinical “rupture” of the treatment process with Amber described in this chapter is characteristic of the discontinuity of most therapeutic work with maltreated or traumatized children. In most public mental health clinics, the average number of consecutive clinical visits before there is an unplanned break in treatment is about three. The family moves, or wears out, or the crisis that brought the child in passes. If the child is in foster care, he may end up going home, or to the hospital, or a residential setting, or another foster home. The fragmentation of therapeutic contact is complicated by the medical economic model, which tends to approve and pay for ten or maybe twenty visits.
Ten years of abuse, neglect, humiliation, marginalization—twenty placements—two grade-levels behind in school, speech and language problems, sensory integration issues, no friends, no family, no social skills, impulsive, inattentive, dysregulated, attachment problems, hundreds of evocative cues from years of maltreatment, now in a new foster home. We approve twenty sessions of Trauma Focused-Cognitive Behavioral Therapy for all of that.
The caseworker checks the “therapy” box and we all move on. Any wonder the long-term outcomes for children in the child welfare system—despite the millions of dollars and person-hours spent trying to help them—are so bad? Maybe part of us doesn’t want to see how things play out for our patients; maybe part of us wants to believe the magic of our twenty sessions: one hour a week actually built in a new “template” for relationships, re-organized the stress response networks in the brain, created a new set of “default” associations to bypass the evocative cues, taught the child social and cognitive strategies, built in new executive functioning capabilities in the cortex, and jumped the child two grade levels in school. (Oh, I forgot—that is not our job—that is for the schools to fix.)
Ok, maybe I’m a little too harsh. Important and enduring things can happen in those sessions; you can reach a child and make a difference, but I hope you get the point. Our current models cannot conceivably meet the overwhelming needs of these children. Knowing this, we must change the models. And we have some very good insights—and research—to help us make changes. Probably, the most important clue we have has to do with the remarkable power of relationships.
Indeed, one of the most important and recurring findings regarding health—in all domains of life—is the powerful role of relational continuity, enduring connectedness with others. The key role for relationships in resilience and healing has been described for decades; yet we continue to develop educational and therapeutic models that pretend that people are interchangeable. Each year in elementary school we get a new teacher: the special bond that can form has a shelf-life, the academic year. Then, in middle and high school, each year, we have many more new teachers.
Certainly, these relationships are important, but what about the power of continuity? If a mentor starts with an at-risk child in middle school, has lunch with that child once a week for the school year, and mentors the same child all the way through high school, there are multiple benefits to the child—including a significantly higher rate of graduation. The duration of the mentoring relationship appears to be one of the major factors in effectiveness. Having a series of mentors over the same time period has fewer benefits, and for some children, these ruptured relationships make things worse. Healing relationships are not interchangeable: we recognize this with marriage and family, and we don’t expect people to simply substitute in a new spouse or new siblings when the school year changes. We recognize it with our own adult friendships, but we have a hard time appreciating the need for this kind of permanence in children’s lives.
Another great example of the importance of enduring relationships is a remarkably effective organization called A Home Within, founded by Dr. Toni Heineman in the Bay Area in 1994. She was tired of working with foster children that came into her practice and then disappeared when they were moved. She made the commitment to create an enduring therapeutic relationship with the foster children she worked with no matter where they went—other foster homes, hospitals, residential centers or back home. She stayed with these kids; and they flourished. Soon, Dr. Heineman got other therapists to volunteer to do the same for one or two foster children.
Over the years, hundreds of clinicians across the United States have been providing high quality ongoing therapeutic services with children in foster care. The outcomes are excellent; in fact they are far superior to the typical outcomes of youth in the foster care system. Relationships help buffer present stressors and heal from past trauma. And so, the heart of any reinvention of therapeutic models has to be the number, nature, and permanence of relationships in the child’s life: the enduring therapeutic web. After all, the key characteristic of a relationship that buffers stress is that it is lasting: the person is known to be safe, familiar, and at least reasonably predictable. This cannot be built in a day: viewing people as interchangeable simply creates a repetitive cycle of grief and loss. To break it, we have to stick around.
Chapter Nine: “Mom Is Lying. Mom Is Hurting Me. Please Call the Police.”
Merle, James’s adoptive mother, clearly had problems with attachment. She had a desperate need to be needed—but unfortunately, there was a lot of toxic stuff mixed in with it. In general, however, foster and adoptive parents tend to have big hearts. While each family makes the choice to parent and adopt for a range of personal reasons, by and large such people are comfortable as “helpers” and they usually have the best possible intentions.
And this is a good thing, because these children and youth need help. But it can be not so good when “the well runs dry.” Living with and caring for children affected by trauma and neglect can be very challenging, to put it mildly. It can often rapidly lead to exhausted, demoralized, disengaged, and burned-out caregivers. The very qualities that make a foster parent capable of connecting, empathizing, and nurturing can make her vulnerable to the emotional turmoil these children carry and can create. Secondary trauma can affect these families, just as it does caseworkers or clinicians working in the child welfare system. And of course, as noted earlier, the system is not great at providing support, training, or supervision for foster and adoptive families.
While it is getting better, the vast majority of situations leave these families with challenging children and minimal support. Add to this the tendency to overload the best foster families with too many challenging children at one time and you set up a perfect storm: a higher probability of child-on-child bullying and abuse, a higher probability of very symptomatic, dysregulated children, and a higher probability of disrupted placement. And that, of course, is simply another relational discontinuity, and this failure further reinforces the child’s distorted view of himself and the world. All of this contributes to poor outcomes for the children and youth. It is not unusual for us to work with a child who has had dozens of failed placements.
Now, shift your focus from the challenges in a foster family to the challenges that a young, often marginally-capable parent faces during reunification with three, or four, or seven of her challenging children. Several years ago, I was consulting with a well-known and highly respected national organization; I believe they do really good work. The caseworkers were presenting the details of a high-needs child who had been stabilized in foster care. I asked about how long this child would be able to be in the home with the current treatment plan in place. My focus was on relational continuity.
But they were working on reunification within a few months. Previously, the child’s mother had been in an abusive relationship and she’d been using multiple drugs. After her children were removed, though, she got out of that relationship, completed rehab, and was now back in school learning a trade. I envisioned a fragile young mother just getting her life together so I asked more.
It turns out that she had seven children in three different placements—and all of them were struggling and having difficulties in their placements and in school. The plan was to reunite them all in her custody. I could see clearly that this would fail. One single parent, with minimal extended family or community connection, was expected to care for seven extremely troubled and traumatized children, all while dealing with her own trauma issues and recovery from addiction.
This, and similar situations, prompted me to develop a new “metric”—in this case, a measure of the strengths of a particular caregiver and home, balanced against the challenges posed by the specific children in the home. Simply subtracting the challenge score from the strengths score gives us a “caregiving reserve” score. Anything below -200 is pretty challenging; the family described above scored -860 on this measure. We have added this “Caregiving Challenge Estimator” (CCE) to our online set of Clinical Practice Tools and it helps treatment teams and families see when they are either setting up a foster family to “burn out”—or creating a situation in which a biological family reunification will likely fail.
Like our other metrics, we hope that the “picture” that the CCE generates will lead to better decision making. If a “helper” or caregiver sees that she is overloaded, she is more likely to be open to better “self-care” planning and to accepting additional help when it is available. If a case-worker sees that a foster family is stretched too thin, he won’t push to place another child there; if a judge sees an impending disaster—like the one described above—in a reunification, possibly she will be open to a better transitional plan with more supports for the biological family.
Would a metric like the CCE have helped anyone see Merle more clearly? Could it have helped child protective workers recognize that James was in a potentially dangerous situation? In this case, probably not. The metric would have shown that the caregiving challenge in Merle’s home was well beyond her capacity to provide—but she had what is thankfully a rare pathological need. When we try to understand the behaviors of someone like Merle, it always takes us back to their personal history. What happened to her during her own childhood, when she was growing up? We tend to parent the way we were parented. We speak the language spoken to us when we were young. We mirror the gestures and facial expressions of our parents, family, and culture. Humans pass both good and bad things down from generation to generation. How does that happen?
As you might expect, it’s complicated—but this is another area where we have learned a great deal more than we knew when we originally published this book. There are multiple mechanisms that shape us. The most obvious of these factors is genes, but there is a new wrinkle in our understanding of genetics that makes understanding the way genes work even more complex. It’s called “epigenetics” and the research here shows that the environment into which a child is born helps determine which genes become active and which remain silent. For example, in a calm, safe environment, certain genes will be highly active—but in a chaotic and unpredictable situation, different genes will dominate. This is part of how the environment in the womb and in children’s first few years of life affects development.
And genetic, epigenetic, prenatal, early childhood interactions, and our whole lifetime of experiences in turn are influenced by community and culture. The exact mixture of which ingredients are most powerful for any given feature will vary: genetics is pretty important when it comes to the color of your eyes, for example, while your family, community, and culture are pretty important in determining what language you speak and your style of dress. And this complexity matters when we look at the degree to which trauma in one generation impacts the next generation. It is highly likely that Merle reflected her own experiences of childhood in how she herself parented—and before her, her caregivers had reflected their own. With each generation, there are additions, subtractions, twists, and turns in how we are influenced by the generation that raised us, but the momentum of transgenerational mirroring is powerful.
Transgenerational trauma—which is passed down from one generation to the next—is an important aspect of the emerging field of traumatology. There are several lenses that can be used to look at the transgenerational impact of trauma; one of the most important of these is socio-cultural. Over the years we have worked with multiple groups that have been affected by relatively recent histories of genocide, ethnic cleansing, or cultural genocide. These include First Nations communities in Canada, Aboriginal communities in Australia, multiple Native American tribes in the United States, and several tribal or ethnic groups in Africa and central Europe. The complex impact of their large-scale multidimensional traumatic experiences is rarely appreciated and has not yet been studied nearly enough.
It is clear however that large-scale systematic abuse of a people will have a transgenerational impact that will echo down a family’s history. Whether this involves the centuries of genocidal policies and practices targeting Native American groups in the United States, the history of slavery of African American people, or policies like the removal of indigenous children in many countries to brutal residential schools, so-called “historical trauma” doesn’t stay in the past.
I believe that systematic analysis and study of these experiences is extremely important: what we learn here will not only enable us to help trauma survivors overcome their symptoms, but will also move us towards a more just society, which doesn’t have to replicate oppression and pass its scars on to our children and our children’s children.
Chapter Ten: The Kindness of Children
Peter’s teacher—and his school—demonstrated remarkable flexibility and tolerance by allowing me to visit his class to discuss the brain and neglect. If I hadn’t had some stature in this area, I suspect the response might have been, “We have worked with children like this for years. We know what to do.”
Indeed, for the last thirty years, a major frustration for trauma-aware parents has been the experience of finally figuring out what works to help their child stay regulated and learn, and then trying unsuccessfully to share it with the school. For example, one mom might tell a teacher, “I know it seems silly but he likes to keep this small toy in his pocket,” or, “If you see him start to get really quiet and withdraw, you might want to let him just walk around a little,” or, “You have to give him a couple of warnings before you make a transition.” Sometimes a teacher or principal will listen, but often not. And, of course, if the fourth-grade teacher listens and makes accommodations, it is no guarantee that the fifth-grade teacher will do the same. Again, relational discontinuities disrupt progress for these children.
Typically, the way educators have viewed, taught, and disciplined maltreated and traumatized children is through a “behaviorist” lens. Behaviorism is a field of psychology which, historically, has been focused on the observable behaviors the individual exhibits and ignores—or has less focus on—emotions or underlying internal mechanisms that drive people to act. This perspective fits well with the DSM model of assigning diagnoses based upon observable behaviors. For instance, Billy is inattentive, impulsive, and has difficulties with age-appropriate social skills. He meets diagnostic criteria for ADHD. Therefore, he “has” ADHD. But we all know that those very behaviors and skill deficits can also be caused by developmental trauma and adversity.
The perspective of behaviorism can be useful in many situations, but, like all models, it has shortcomings. A huge shortcoming for children and youth with trauma-related sensitization of their stress response networks is in the use of “operant” (also called “contingent”) strategies. This is the “reward and punishment” view you probably learned in Psych 101; one common example is the “point and level” system often used in residential programs in which children advance to “higher” levels with greater privileges if they behave as expected—or are “set back” to lower levels where they lose privileges if they do not comply.
The idea, of course, is that this will increase desirable behaviors through “reward” and minimize or extinguish undesirable behaviors using “consequences,” which, let’s face it, everyone knows means punishment. This model cannot and never was intended to help children develop complex capabilities such as social skills, which require a child to perceive subtle signals that often vary and cannot be taught through simple compliance. Nor can it help people learn to regulate their stress responses.
Sadly, when a child with a history of trauma struggles in school and has behavior problems as well, he will often be put into a “behavioral” program. And when the teacher gives the consequences attached to this approach, it will not calm him down or allow him to get control over his behavior; rather, it will escalate the child, increasing the probability of more disruptive behavior or even a critical incident, such as running away or becoming aggressive, which can lead to being physically restrained. Basically, what happens in these cases is that a “flight or fight” response is elicited from the child. The effect in the classroom is the opposite of what is desired: these children then get put into seclusion, or are suspended, or even expelled from school. Our schools, due to well-intended, but trauma-ignorant, practices, often make the lives of our maltreated and traumatized children worse. But it doesn’t have to be that way.
In 2010, Steve Graner—a lifelong friend of mine who happens to be an English teacher and coach—heard me speak at a daylong conference in our hometown, Bismarck, North Dakota. He and one of his teaching colleagues, Crystal Halseth, a science teacher, immediately saw the benefits of applying the concepts I was teaching about the brain, stress, and development to better reach children in their classrooms.
They talked with me and other colleagues at The ChildTrauma Academy, and we sent them the material we use for clinical training. We had always worked with schools to help them better understand children affected by trauma; we had hoped to develop a version of the Neurosequential Model for Education (NME). We were working to modify our training process and metrics so that they could be used in educational settings. But we were all so busy that the process of developing the model was slow. And so, we were happy to let Steve pick up the ball.
Steve and Crystal started by having a completely voluntary book group, in which they met with other teachers and discussed The Boy Who Was Raised as a Dog. They went chapter by chapter, and participants told them that they found the group stimulating and productive. Then, Steve, Crystal, and a number of other teachers started to think about how to bring rhythm into the classroom, both to help regulate children by giving them brief sensory “breaks” and also to teach content. For example, they started using rhyme more often in their curriculum. Word of mouth within their school led to another round of book study, and then another for other schools in the school district. (Steve ultimately wrote the majority of an older version of the book study guide included in this edition of the book.) Steve and Crystal went through and selected and modified some of our teaching content; we worked together to make sure it would be able to reach teachers without distorting the neuroscience or core clinical concepts.
With their energy and time, we finally had a way to develop the beta-version of the NME. In 2012, Steve retired from teaching, and we convinced him to come out of retirement to lead the ongoing development and dissemination of this program. As we will explore a bit further in the last chapter of the book, the growth and effectiveness of the NME has been impressive.
Over the last ten years, other clinicians and educators have been addressing the need to have a trauma-informed educational system. In our experience, Collaborative Problem Solving (CPS) is the most flexible and effective. CPS has been around for over twenty years and incorporates the key principles we teach in the NMT. It was co-developed by Dr. Stuart Ablon. CPS can teach parents, educators, children, and clinicians practical and effective ways to understand and address behavioral problems in the school setting; this includes trauma-related behaviors.
Most important, CPS has a sequence of implementation that understands the fundamental reality that, in order to “get to the cortex” and prepare children to learn abstract and cognitively challenging material, we have to first relationally connect with them. And, before we can effectively connect, the child has to be regulated—at least to a certain degree. The sequence of effective engagement, therefore is (1) regulate (2) relate, and then (3) reason with the child (see Appendix, Figure 7). Getting out of sequence will result in ineffective communication, frustration for both parties, and sometimes flight or fight or “shut down” dissociative behaviors. In any human interaction, the only way to the cortex is through the brainstem/diencephalon and then the limbic system (see Appendix, Figure 2).
While conventionally viewed as a cognitive intervention, CPS is also fundamentally a relational intervention and uses a variety of sequenced, effective, and rhythmic interactions to promote regulation, connection and, ultimately, the cognitive process of defining and solving a specific problem in a collaborative way. The Neurosequential Model and CPS can help embed all of the six Rs that are key to an optimal learning environment. These are: Relevant (developmentally appropriate) content, Regulating rhythm, Repetition (in the correct patterns of dose and spacing), Relational (safe and predictable), Rewarding (pleasurable), and Respectful (of child, family, and culture). (For more on CPS, see the website ThinkKids.org; to learn more about other trauma-sensitive practices in education see TraumaAndLearning.org.)