9
Pot
Much of the American public is fiercely divided about marijuana. On the one hand, many believe it to be no different from having a few beers. Marijuana is also now used medicinally as a painkiller, and it has recently been legalized in some states for recreational use as well. On the other hand, there are studies that show that smoking pot can lead to the use of harder drugs and even can stunt one’s intellect. No wonder we’re confused. Scientific breakthroughs showing how certain chemicals work on the brain have recently reaffirmed the risks that marijuana poses, especially for adolescents. What is not in dispute is that marijuana is a favored substance of abuse in all social strata and demographics, from the just-scratching-to-get-by inner cities to the well-heeled Hamptons. But because recreational marijuana use is legal now in at least two states, Washington and Colorado, the movement to embrace marijuana as a relatively benign mainstream drug of choice has accelerated.
While casual marijuana smoking may not bend many social mores in much of the country anymore, neuroscience is beginning to reveal that it is not as inconsequential—at any age—as previously thought. Pot is now regarded by many experts as a “gateway drug” leading to the use of more dangerous illicit substances. It impairs mental functioning and coordination and poses a threat to public safety when, for instance, individuals who are high get behind the wheel of a car.
Among the stories I’ve heard, one young person who began to smoke pot regularly at the age of thirteen and continued well into his twenties now says that though he has not smoked a joint for several years, he still feels as if he’s in a fog. He doesn’t even drive a car because he doesn’t trust his attention and concentration; he struggles to keep a conversation going; and he says he suffers from anxiety, depression, and paranoia. He also says he’s amazed that his middle-aged mother remembers all sorts of things about her early life, but that he can recollect only scattered bits and pieces.
More than 100 million Americans over the age of twelve admit to having tried marijuana at least once in their lives. Despite seven decades of criminalization, marijuana remains the most popular illicit drug in the world, with upwards of 200 million people using pot each year, according to the United Nations Office on Drugs and Crime. The highest use is among young people—and the age of initiation is getting younger.
In fact, marijuana is outpacing alcohol as a public health problem in teenagers. In the last five years, marijuana abuse has been responsible for almost two-thirds of admissions of teenagers, ages fifteen to nineteen, to rehabilitation centers, compared with less than a third for alcohol. The director of a rehab hospital in Connecticut that cares for a lot of clients from New York City and the suburbs told me recently that in the past five years the population at his clinic has gone from primarily adults to primarily adolescents and young people between the ages of seventeen and twenty-five. These people are largely multisubstance abuse cases.
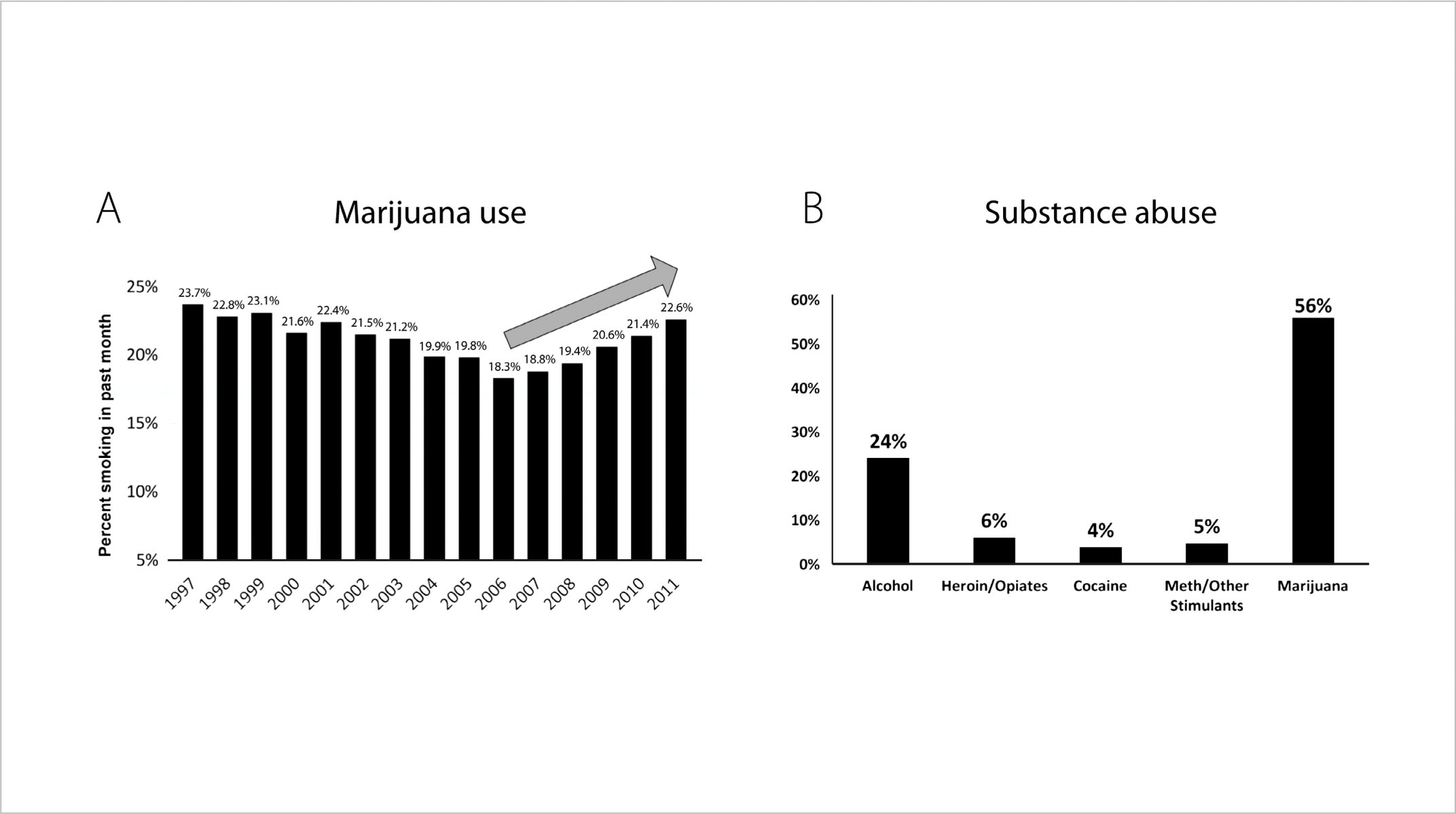
FIGURE 21. Increases in Marijuana and Substance Abuse in Teens in the Last Decade.
Of course, marijuana abuse is hardly a new problem. In 1906 Congress passed the first drug law in the United States, called the Pure Food and Drug Act. At the same time, concerns and criticism about marijuana and its potential addictiveness were front and center, though not for the medical or scientific communities but for law enforcement. Between 1913 and 1937, twenty-seven states, beginning with California, passed legislation outlawing or severely restricting the cultivation and sale of pot. The watershed moment for marijuana in the United States came on July 1, 1930, when the Department of the Treasury established the Federal Bureau of Narcotics, headed by Harry Anslinger. In 1937, with President Franklin Roosevelt poised to sign the Marijuana Tax Act, Anslinger testified before Congress, and although no scientific studies had yet been conducted on cannabis, he said, “Marijuana is an addictive drug which produces in its users insanity, criminality, and death.” Dr. William Woodward of the American Medical Association also testified at those 1937 hearings and said, contrary to Anslinger, “The American Medical Association knows of no evidence that marijuana is a dangerous drug.” (At least we know that mixed messages about pot are nothing new!)
Five years later, the New York Academy of Sciences’ cannabis panel issued the first scientific study on the drug and concluded there was no association between smoking pot and either criminality or insanity. Anslinger, naturally, was outraged. As retribution, he made it impossible for years for researchers to acquire cannabis in order to conduct studies. Roosevelt’s tax act also effectively outlawed marijuana, placing it under the same severe restrictions as heroin and cocaine. The war on marijuana had begun.
Cannabis is the only plant that contains the unique class of molecular compounds or metabolites known as cannabinoids, including tetrahydrocannabinol (THC), which is largely responsible for marijuana’s peculiar physiological and psychopharmacological effects. More than four hundred chemicals have been identified in cannabis, at least sixty of which are cannabinoids. One reason THC has such a potent effect in human brains is that we manufacture our own cannabinoids, called endocannabinoids (translated literally, “inside cannabinoids”). So we have natural cannabinoid receptors on our neurons on both sides of the synapse. When marijuana is smoked, the THC is rapidly absorbed into the blood and distributed to the tissues. Cannabis affects body temperature, blood pressure, and heart and breathing rates.
Mentally, marijuana causes an altered state of consciousness that is perceived as relaxation, pleasure, and even euphoria. Ordinary sensory experiences such as eating, listening to music, or watching a movie are intensified. Anxiety is usually decreased, but sometimes marijuana can increase it instead and can also cause depression or paranoia. At high doses users can feel a reduction in motivation and spontaneity and a general lethargy, but occasionally also confusion, hallucinations, and nausea. The immediate effects of marijuana usually kick in about fifteen minutes after smoking; others can last for three or four hours.
A consequence of pot smoking usually referred to as “the munchies” is an uptick in appetite with a neurobiological basis. Italian scientists recently isolated the probable cause: marijuana appears to affect the brain’s hypothalamus, which regulates food intake.
THC is the psychoactive agent in cannabis that produces the high. The stumbling and lack of coordination experienced by someone high on pot occur because THC affects the cerebellum. Slurred speech, hyperawareness of sound, other audiological and visual distortions, and the sense of time slowing or speeding up are results of THC’s effects on the sensory regions of the brain.
The pot smoked by kids today is not the pot you might have smoked in college. In 1985, THC concentrations in marijuana averaged out to less than 4 percent. In 2009 the average THC concentration in marijuana was close to 10 percent.
The most critical issue for teens is that THC disrupts the development of neural pathways. In an adolescent brain that is still laying down white matter and wiring itself together, such disruptions are far more harmful than if they were taking place in an adult brain.
The first major research breakthrough came in 1988 when Allyn Howlett and William Devane identified how TCH binds to cells, or receptor sites, in the brains of rats, and in 1990 scientists at the National Institute of Mental Health identified the location of those receptors in humans. One of the naturally occurring endocannabinoids discovered was the neurotransmitter anandamide, whose name comes from the Sanskrit word “ananda,” meaning bliss. Anandamide is found throughout the brain and especially in areas involved in regulating mood, memory, appetite, pain, cognition, and emotion.
This cannabinoid, researchers found, also looks a lot like another natural compound known as the body’s ideal painkiller: endorphins. Discovered in the mid-1970s, endorphins were the prize scientists had been looking for as they puzzled over why the brain has receptors for opiates. One of the most widely known opiates at the time was a chemical that oozes from poppy plants and produces sensations of euphoria and pleasure. That substance, called opium, contains naturally occurring forms of both morphine and codeine.
Parents will sometimes ask me why their teens say they need pot to relax. Part of the answer may lie in the fact that the adolescent brain, because it is firing more often and more intensely than an adult brain, is also experiencing more stress, and with increased stress comes an increased desire for relief. Enter pot. Scientists have found that THC affects the suppression of pain, and in 2011 scientists at the National University of Ireland, Galway, found that one of the keys to the suppression of pain is the production of endocannabinoids in the hippocampus. They also discovered that the hippocampus plays an active role in the suppression of pain in times of high stress. Pain suppression, or analgesia, has long been regarded by evolutionary scientists as an important biological function to help humans escape life-threatening situations.
At one time scientists believed that endorphins were also responsible for what is known as the runner’s high. The general agreement today, however, is that the explanation of the sense of euphoria and relaxation that characterizes intense exercise is a lot more complicated. When researchers developed a line of mice in which the gene responsible for the production of endocannabinoids was deleted or knocked out, the mice exhibited a 40 percent decrease in running activity. If the motivation to run or to exercise intensely is related to the runner’s high, then certainly endocannabinoids appear to be at least one primary driver. Evolutionarily, this makes sense, too, since someone skilled in endurance running was likely to be better at tracking down prey—or outrunning danger—than the more sedentary members of primitive societies.
Once endocannabinoids were discovered, researchers began to find them everywhere, and they are especially dense in key brain areas involved in cognition, memory, emotion, motor coordination, and motivation. When THC is introduced through inhaling or ingesting marijuana, it bathes the brain, but it also heads straight for the abundant endocannabinoid receptors in the hippocampus, amygdala, basal ganglia, cerebellum, and nucleus accumbens, where it interferes with the brain’s chemical processes by either inhibiting or enhancing certain activity. Because THC binds to the endocannabinoid receptors four times as well as the brain’s naturally occurring cannabinoids, THC molecules are able to overwhelm the receptor sites and interfere with normal brain function. When that happens in the cerebellum, for instance, it interrupts the smooth functioning of the motor cortex; this is why pot smokers can appear to be slack, clumsy, and slow moving and have trouble reacting promptly in dangerous situations. And that lack of responsiveness, with chronic use, results in an inability to learn from negative experiences. Most important of all, these negative effects appear to be exaggerated the earlier a person begins using marijuana. In their early teens, pot-smoking adolescents have been shown to have smaller whole brain volume, reduced gray matter, and increased damage to white matter compared with nonusers. That damage, scientists say, can still be seen in the brain scans of chronic users well into adulthood.
A small part of the amygdala, where cannabinoid receptors are especially dense, is responsible for producing the sense of awe. This same part also helps the person know what information is new and what is not so that a person can respond with the appropriate sense of heightened awareness to novel stimuli. When pot smokers claim that colors are more beautiful, music is more profound, and taste is more acute than when they’re not high, it’s because the flood of THC has caused this part of the amygdala to overreact. When bathed in THC, everything appears new to the brain’s emotional center. Teens, whose brains are already in a nearly constant state of heightened awareness, are especially affected by this overstimulation, and breaking the pot habit, for this reason, is more difficult for adolescents than adults.
There are more problems with the amygdala the day after smoking pot, too. Having already been overstimulated by THC, the amygdala now has fewer cannabinoid receptor sites; this means it takes more than the normal amount of stimulation to get the brain interested in learning something new. How to do it? By smoking more pot, of course. For a teenager, this kind of marijuana “saturation” quickly leads to addiction.
In a blog run by the 420 Times, a self-described “magazine of medical marijuana and natural healing,” a man recently posted a message about his frustrations in trying to deal with his pot-smoking daughter:
I’m an upper middle class, mid-thirties father. I’ve smoked a few times but didn’t like it and don’t drink alcohol either. I support legalization and usage of drugs but only if it’s done in a healthy and supportive environment and by individuals that do so in a responsible manner.
My 15-year-old daughter is generally an exceptional student and extremely trustworthy person. She gets straight A’s in school, is very disciplined, etc.
We’ve given her a massive amount of freedom, but we found out that she had been smoking and drinking with her friends and lying to us for the last 2 months. As of now she’s effectively grounded until further notice. The issue isn’t so much that she had been smoking as much as lying and hiding from us for months now.
When we told her that she can’t do marijuana until further notice she broke down crying and says she “needs it” and won’t stop using it. This is pretty solid evidence for me that she should not be using it.
The most significant factor in the association between marijuana abuse and potential brain damage is age. Early teen users are twice as likely to become addicted, and those who indulge in pot before the age of sixteen have more trouble with focus and attention and make twice as many mistakes on tests involving planning, flexibility, and abstract thinking. Also, the younger a pot smoker is, the more he or she smokes. Bottom line: The earlier the use, the greater the abuse.
Forgetfulness is the most widely reported cognitive deficit associated with marijuana use. THC has an effect on LTP, and can decrease the activation of glutamate receptors that build synapses during the memory process. What’s more, the effects of cannabinoids can last for days in adolescents, in contrast to the briefer effect in adults. Researchers looked at LTP and simulated the effects of cannabis exposure by bathing rat brain slices in 2-AG, a synthetic cannabinoid. They found that slices bathed in 2-AG had little to no LTP, while slices in normal control conditions showed good LTP. The effect of cannabis on LTP is known to affect two points in the synapse-building process: it first prevents the signal from leaving the axon and then blocks the machinery that makes new synaptic proteins to make stronger synapses.
Memory impairment after exposure to cannabis is similar in adults and adolescents, but adolescents suffer the effects far longer. When heavy marijuana users, ages thirty to fifty-five, have been tested, studies consistently show that in the days and weeks following ingestion of cannabis, they have poorer memory and learning skills. By day twenty-eight, however, their cognitive problems have resolved. Adolescents with only short exposure to cannabis show cognitive deficits similar to those of chronic adult users, but with continued use their cognitive impairment does not completely resolve and in some cases can last for months, even years.
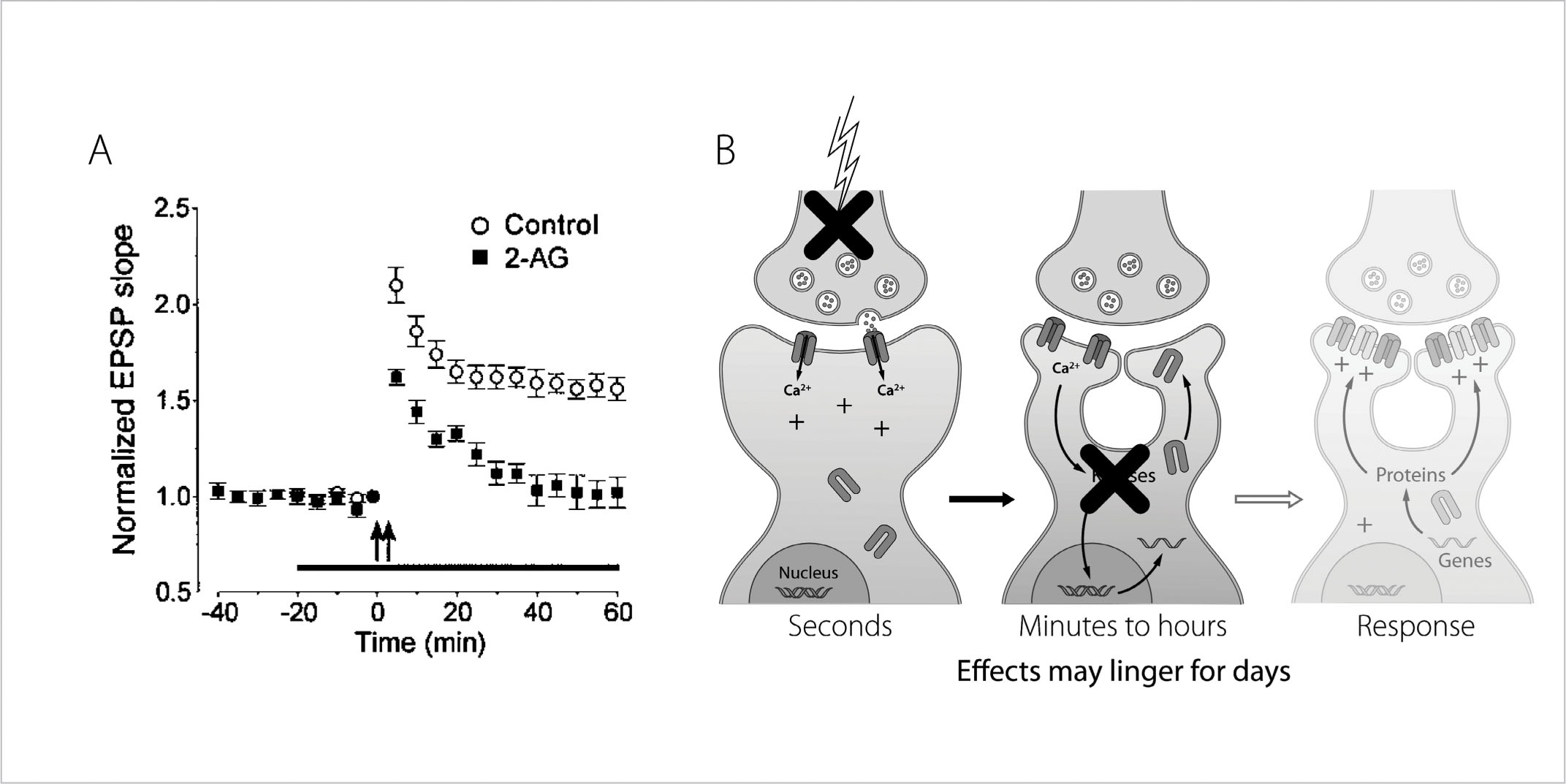
FIGURE 22. Effects of Cannabinoids on Learning: A. Brain slices stimulated in the presence of synthetic cannabinoid 2-AG show little to no LTP, while slices stimulated in normal “control” conditions showed good LTP. B. Cannabis prevents the signal from leaving the axon, and blocks new synaptic proteins from developing stronger synapses.
Even more worrisome is the link between chronic pot use during adolescence and decreases in IQ. In the last five years, several studies have shown that verbal IQ especially is decreased in people who have smoked daily starting before age seventeen, compared with people who smoked at a later age. These studies also show different patterns of activation of brain areas required for decision-making using functional MRI, making the findings even more significant.
Marijuana use has also been observed to inhibit functioning in the areas of the cortex that play a critical role in recognizing errors, specifically insight into one’s own thoughts and behavior. Neurologists and neuroscientists have associated the inability to detect errors with several psychopathologies, including the psychotic delusions of schizophrenia. There is evidence that schizophrenics have less white matter than normal people, and this pattern is also seen in those who have used pot chronically during adolescence.
The risk of schizophrenia is also two to five times higher than normal in people who used marijuana chronically during adolescence.
In a 2010 article in the Toronto Star, Nancy J. White tells this story:
At age 17, sitting in the basement with friends smoking pot, Don Corbeil first noticed all the cameras spying on him. Then he became convinced a radioactive chip had been planted in his head. “I thought I was being monitored like a lab rat,” he explains.
It never occurred to him that marijuana could be messing with his brain. Corbeil had been smoking pot since he was 14, a habit that escalated to about 10 joints a day.
He started hearing voices and, at one point, Corbeil thought he was the Messiah. Police found him one day talking incoherently, and brought him to hospital, where he was eventually diagnosed with drug-induced psychosis.
Corbeil had dabbled in other drugs, such as acid and ecstasy. But marijuana was his mainstay.
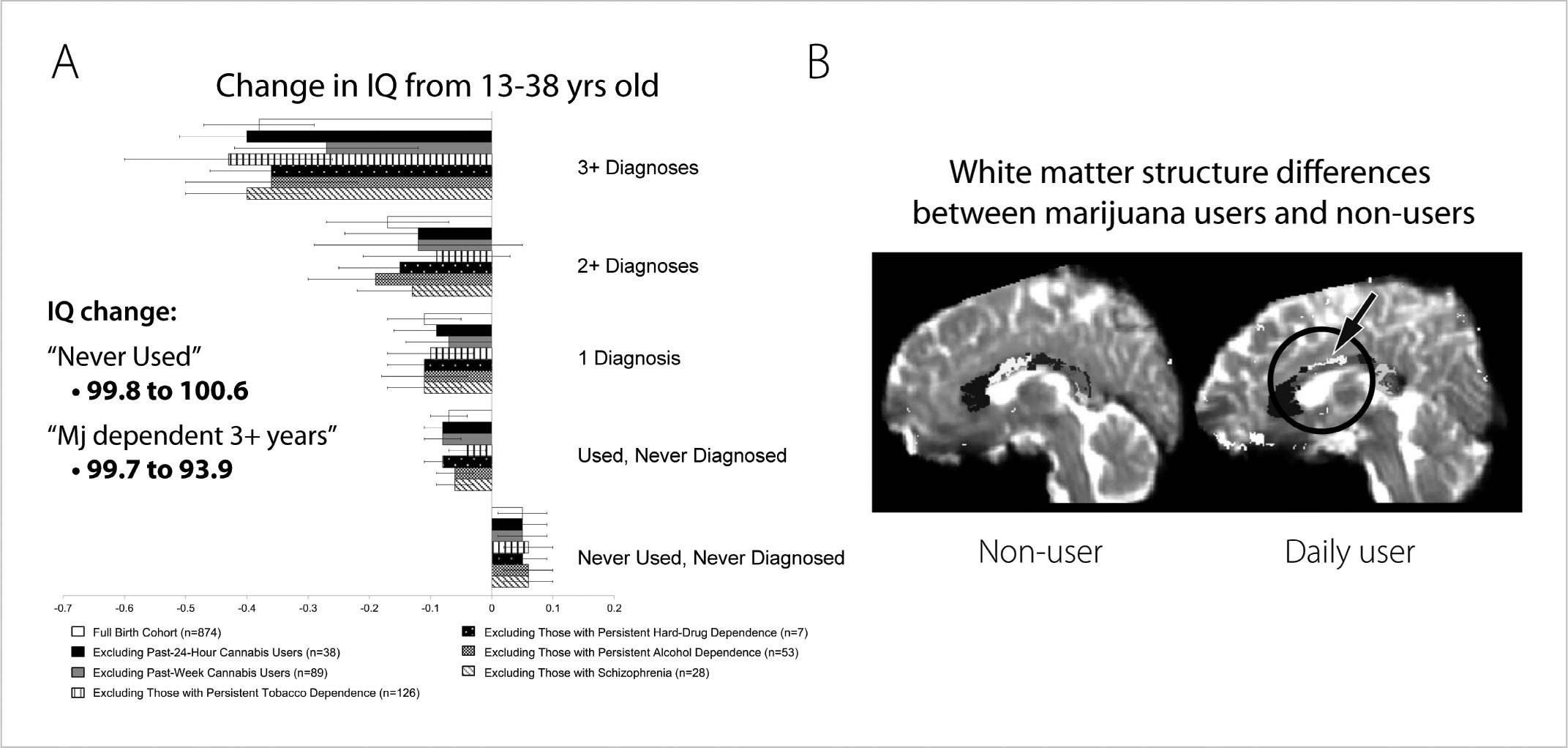
FIGURE 23. Long-Term Effects of Marijuana on Gray and White Matter in the Teen Brain: A. Chronic marijuana use before age seventeen can result in a drop in IQ (the more years of chronic use, the larger the drop). B. Imaging studies of human brains show that white matter in the corpus callosum (the area that joins the two hemispheres of the brain together) is thinner and less myelinated in those who used marijuana chronically during adolescence.
A study done in Great Britain found evidence to support the conclusion that cannabis use was an important causal factor in the development of schizophrenia and that smoking marijuana doubles the risk of psychosis. More recently, a study that followed nearly two thousand teenagers into adulthood found that young people who smoked marijuana were twice as likely to develop psychosis over the next ten years as those who did not smoke marijuana. Another study concluded that marijuana use in late childhood and the early teens could actually hasten the onset of psychotic behavior by three years.
Other mental illnesses have also been linked to cannabis. A scientist at Canada’s Centre for Addiction and Mental Health surveyed more than fourteen thousand people and discovered that those who smoked marijuana nearly every day not only were twice as likely to suffer psychosis but also were twice as vulnerable to anxiety and mood disorders, especially depression. In 2010, the Netherlands Institute of Mental Health and Addiction released a study based on data collected by a World Health Organization mental health study of fifty thousand adults in seventeen countries. One of the conclusions the Dutch researchers came to was that early marijuana use was linked to a 50 percent increase in the risk of having an episode of clinical depression after age seventeen. One of the largest studies followed tens of thousands of young Swedish soldiers for more than a decade. The heaviest users—that is, those who said they had used marijuana more than fifty times—were six times as likely to develop schizophrenia as those who had never smoked pot.
Why is this happening? Once again basic research is showing us that marijuana exposure during adolescent brain development can change the receptors in multiple areas of the brain—not only in the hippocampus and cortex, resulting in changes in cognition, but also in the nucleus accumbens in a way that can increase the “addictability” of the brain to other substances. This goes both ways actually. Nicotine in cigarettes also changes the number of cannabinoid receptors in the brain and makes brains more sensitive to the effects of marijuana.
Ever since marijuana entered the public discourse, people have debated whether it’s a gateway drug or not—that is, can smoking pot lead to use of harder drugs? At least one expert on adolescent drug use told me he believes pot is, in fact, a gateway drug, though not in the way you’d expect. He said it’s not because of peer pressure, per se, but rather because of peer exposure.
“Look, you start with pot at thirteen,” he said. “When looking back at this kind of kid, when he was on pot, he was around people trying other things, and you have less of an ability to say no to other drugs because of your still-developing frontal lobes. You’re probably already high anyway, so piggybacking on pot with another drug doesn’t seem all that bad.”
Another little-known fact is that levels of two abrasive components in marijuana smoke, tar and carbon monoxide, are three to five times greater in cannabis consumers than tobacco users. Smoking five marijuana cigarettes is equal to smoking a full pack of tobacco cigarettes, according to the American Lung Association. Marijuana smoke, which users inhale and try to hold in their lungs for as long as possible, also contains 50 to 70 percent more cancer-causing chemicals than cigarette smoke contains. (The use of a bong, a pipe that filters cannabis through water, is no insurance against these deleterious chemicals since the principal cancer-causing ingredient in marijuana is benzopyrene, which does not dissolve in water.)
All this research on the effects of marijuana on the teen brain should effectively be a public service announcement for parents everywhere, and the message is crystal clear: Adolescent brains are not as resilient as adult brains when it comes to marijuana. Teenagers are especially vulnerable to the drug because they are at a critical stage in the development of two of the most sophisticated parts of their brains—the frontal and prefrontal cortex—and these are precisely the parts most affected by marijuana. This is not minor or incidental. These brain regions are used every day for basic cognitive tasks, whether it’s abstract thinking, the ability to change one’s behavior in relation to changing demands in the environment, or the inhibition of inappropriate responses.
If you grew up in the 1960s or 1970s, it’s more than likely you did some level of experimentation with marijuana, but you surely know by now that today’s pot is not the Mary Jane of yore. It is exponentially more potent and, for that reason alone, exponentially more seductive and dangerous. So before we talk about how to steer your children away from pot and how to talk to them about its dangers, let me tell you first what you should not do. Do not minimize the subject—either out of your own belief that smoking a little weed didn’t hurt you or because you’re too afraid of learning that your teenager is indulging in marijuana. Don’t even joke about past pot use with your spouse or friends, because kids do pick up on these things. They do notice. They are paying attention and they are filing it all away.
Recent research shows that fear of losing their parents’ trust and respect is the greatest deterrent to adolescents’ drug use. They won’t tell you this, of course, but when asked by researchers what prevents them from experimenting, a majority of non-drug-using teenagers say it’s because their parents expected them not to and that their parents would be disappointed in them if they did. So take advantage of this power, however unacknowledged by your sons and your daughters. Whenever possible, be concrete and practical when talking about drug use. What are their goals? What are the things they value most? Reiterate to them that college, a scholarship, making varsity, or passing drivers’ ed—all those things will become more difficult to achieve if they use pot. To be convincing, of course, you also need to be knowledgeable about what marijuana does to the brain. That’s where this book comes in handy. You need to know what to say when your teenagers try to argue that pot is harmless, that it makes them feel good, that it doesn’t affect them negatively. For instance, if your son says that smoking pot helps him to relax and relieves him of his anxiety, then you have to remind him that he’ll always feel anxiety throughout his life and he can’t always turn to pot to find relief. It’s important to figure out what’s causing the anxiety and deal with the source rather than try to “medicate” it away.
Don’t lie to your kids either. If they ask you whether you got high or smoked pot when you were their age and you did, then you must be honest. But be honest within a context. Remind them that today’s marijuana tends to be more potent and easier to access given social networking, among other things. Remind them that scientists didn’t know nearly as much as they do today about the effects of pot on the brain and that your kids have the advantage of this knowledge when they make choices.
And because repetition is good for the adolescent soul (even though teens complain about it), don’t think that bringing up the subject or asking your son or daughter about pot smoking just once is enough, because it isn’t. That’s why whenever I can, I use the news or a story of a neighbor’s teenager or a new scientific study as a “teachable moment,” a chance to talk to my boys about what pot and cigarettes and alcohol and hard drugs have done to others and are capable of doing to them. Don’t avoid talking to your kids, even if you think they aren’t listening, because they are.
The implication of current marijuana research for teenagers is profound. Manipulating or interrupting this important stage of development with cannabis could change the entire trajectory of their brain development, with some deficits not appearing until much later in life. If, as parents, teachers, and guardians, we ignore the science, we do so at the peril of our own children.