12
Mental Illness
Weathering teenagers’ adolescence often means just riding out the rough seas with them until calmer waters are reached. But because adolescence is already a time of mood swings and behavioral irregularities, it is even more important for parents, guardians, and teachers to be aware of the emotional needs of adolescents, especially in times of crisis and stress, when adolescents’ vulnerability to mental disorders is at its highest. There are two rules of thumb parents should remember: Number one, behavioral changes that seem to cluster or are associated with other symptoms should raise your level of suspicion that you might be dealing with something more than just a difficult teenager going through a phase. And number two, it is better to be safe than sorry. If you have any concern that radical or progressive changes are happening to your adolescent, then you must seek help for your child.
Difficult or irregular behavior in teenagers can be expressed by a variety of emotional states, from moodiness and sadness to oppositional behavior, rage, and aggression. The line between these highly charged but normal adolescent states and “real” mental illness can be difficult to determine. That’s because these behavior traits (which are common in kids this age) can be seen both in teens without a diagnosable personality or mood disorder and in teens with one of the more severe mental illnesses, such as major depression, bipolar disorder, or schizophrenia. Signs of depression, for instance, are hard enough to detect in teenagers you’re around all the time. With digital devices their constant companions, normal teens seem withdrawn compared with teens twenty years ago, making it that much harder to distinguish between a shy, introverted adolescent and a seriously depressed one. Adolescents don’t engage in as many group activities as they did years ago. All this makes figuring out whether your teenage son or daughter is mentally troubled more vexing. “Real” mental illness must be diagnosed and is usually treatable, but how do you tell? When is it time to worry?
There are two general characterizations of adolescent behavior that can help in making this distinction: severity of mood and change in function. Any exaggeration or deepening of a teenager’s mood swings or a predominance of one mood over another—especially anger, sadness, or irritability, and especially if it lasts longer than two weeks—is a sign of possible psychiatric problems. Changes in sleeping or eating habits, a tendency to act out more than usual, taking more risks, and spending less time with friends and family are also warning signs. So are failed friendships and an absence from extracurricular activities. Another big difference between normal but still disturbing teenage behavior and mental illness is that troubling behavior in teens without mental illness is usually isolated and, more important, doesn’t interfere with the ability to function either in school or at work.
With major mood and affective disorders, however, there is rarely just one “thing” wrong. For instance, major depression is usually accompanied not only by tearfulness but also by changes in eating habits (and consequent weight gain or loss) or withdrawal from family life. Self-mutilation, alcohol or drug abuse, expressions of self-loathing, violence, and of course suicide attempts also often accompany major depression.
A sensitivity to criticism can be very acute, and given that teens already live in a world where most of what they do academically, athletically, and socially is being judged in some way, this is particularly hazardous. But only when this sensitivity is accompanied by, say, “somatic” complaints—that is, frequent pain, aches, nausea, and other physical symptoms of which they may not even be aware—is it likely they are suffering from clinical depression.
Adolescence is a unique time, as it is a period in life when some mental illnesses first emerge. What comes as a bit of a surprise is that we need to have a mature enough brain to “do” mental illness. In fact, it is known that many mood and affective disorders involve abnormal functioning of the frontal lobes, especially the prefrontal cortex. How, for instance, can you have adult-like schizophrenia that stems at least in part from abnormal frontal lobe activity if your frontal lobes aren’t hooked up to the rest of your brain yet? This is likely one of the reasons why schizophrenia has its onset in the late teens and early twenties—it is not a disease of childhood.
Another interesting point is that severe mental health problems are more common in adolescents than either asthma or diabetes. One in five teens will suffer a mental or behavioral disorder serious enough to affect his or her daily life. Even more alarming: roughly half of all adult mental health disorders begin during adolescence. Among youths twelve to sixteen years of age, up to 20 percent of girls and 10 percent of boys have considered suicide. After motor vehicle accidents, suicide is the leading cause of death for teenagers and young adults. Substance abuse, high-risk behavior, plummeting school grades, even frequency of health problems can all be indicators of depression or other psychological stress in adolescents—or they can be warning signs of serious mental illness on the horizon.
Three-quarters of young adults with psychiatric illness had their first diagnosis between the ages of eleven and thirteen. In a study in England, researchers followed more than a thousand kids from childhood through age twenty-six. They found that 76.1 percent of adults who were in active treatment had a diagnosis made before age eighteen and 57.5 percent before the age of fifteen. For young adult patients who were receiving intensive mental health care, the rates were higher, with just a shade under 78 percent being diagnosed before age eighteen and a bit more than 60 percent before fifteen.
Importantly, in most cases the type of illness was the same; that is, if they had anxiety or depression as teens, then they were likely to have suffered anxiety or depression as adults. Some did not follow this pattern, though, with adult-onset schizophrenia being preceded by a wide array of juvenile psychiatric symptoms. Schizophrenia most commonly emerges in the mid- to late teens and early adulthood, including into the early thirties. However, psychosis, which can be a forerunner of schizophrenia, depression, or bipolar disorder, is seen earlier and also can be a first symptom of schizophrenia.
Also, the more minor problems of adolescent conduct disorder (CD) and oppositional defiant disorder (ODD) appeared to precede a variety of adult psychiatric disorders. While only 20 percent of eleven- to eighteen-year-olds were diagnosed with behavior problems in the British study, they became 25 to 45 percent of the adults with a mental illness. Psychiatry has tended to ignore the role of early conduct disorder, and this gives us reason to pay attention to it. The main point here, of course, is that even minor, and definitely major, psychiatric problems need to be addressed early since they put the person at higher risk for mental illness later in life. Parents, teachers, and even teens themselves need to be made more aware of this fact.
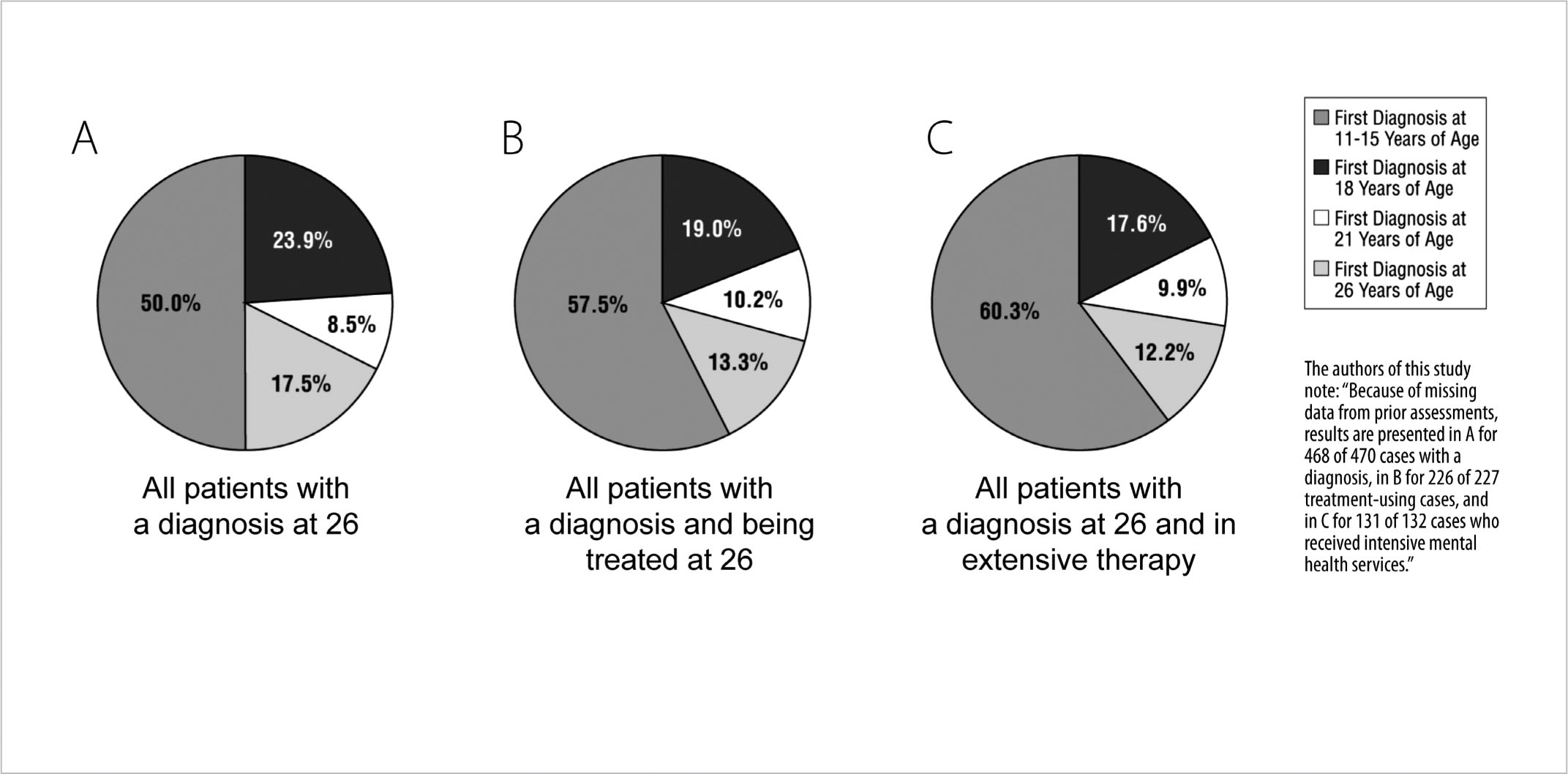
FIGURE 27. Prior Juvenile Diagnoses in Adults with Mental Disorders: A. Age at first diagnosis, of any psychiatric disorder, among patients with confirmed mental disorders at age twenty-six. B. About three-fourths of all subjects diagnosed by age twenty-six had received that diagnosis before the age of eighteen. C. Almost 80 percent of patients with very severe mental illness, requiring intensive therapy, were diagnosed by age eighteen.
Conduct and oppositional disorder can be very disruptive to the family, to say the least. I have a colleague with a teenage daughter diagnosed with CD who has been in and out of residential facilities for several years. CD often emerges in the teen years, and according to the National Institute of Mental Health, between 2 and 5 percent of all teenagers receive this diagnosis. Young people with conduct and oppositional disorder also have a much higher likelihood of engaging in risk-taking behavior, such as binge drinking, unprotected sex, and driving under the influence. Fortunately, because this association is so well known, the diagnosis of a conduct or oppositional disorder should be a huge red flag, and an opportunity for aggressive intervention.
Conduct disorder is also very costly to society and requires expenses on the part of the family, school system, and medical system, as well as the juvenile justice system. A study out of the University of California, San Francisco, in 2008 estimated that annual medical costs for a child or teen with a conduct disorder were $14,000 compared with $2,300 for a child or teen without conduct disorder. There are now many home- and school-based programs for effective management of conduct problems, and these should be accessed ASAP once this diagnosis is suspected. In parent management training programs, therapists teach adults how to effectively interact with their children and how and when to use reinforcement or punishment to encourage appropriate behavior. Online courses are being made available for parents at places like www.thereachinstitute.org. And more and more school districts also are making available instruction and advice for both parents and teachers about how to deal with CD. CD is almost an extreme form of some of the misbehavior normally expected in adolescents.
Next up are anxiety and eating disorders, which show a surge in adolescence. As we saw in the previous chapter, the adolescent brain is more affected by stress, and hence it is no surprise that anxiety is prevalent in this age window. In fact, recent reports suggest we have an epidemic of anxiety and related disorders such as anorexia in teens these days. Studies across the United States reveal that between 2 and 9 percent of all teens have some kind of anxiety disorder. These include obsessive-compulsive disorder (OCD), panic disorder, agoraphobia, and other social phobias. There is a gender difference, with girls having higher rates and earlier onset of anxiety disorders. Anxiety disorders have a strong connection to environmental stressors; this is especially true of anorexia, the most common eating disorder, which typically appears during adolescence and is much more common in girls than in boys. I recently learned about a fifteen-year-old girl who in 2009 decided to go on a post-Christmas diet with her mother to shed a few extra pounds they’d both gained over the holidays. After five or six weeks, the mother had lost the weight she’d gained and stopped dieting, but not the daughter. In February 2010 the girl’s swim coach reported his concerns to a school nurse, who contacted the parents. Apparently the girl was very good at deceiving people about how much she ate by hiding food up her sleeves or throwing it away when no one was looking. Her mother took her first to the family doctor, who agreed to monitor the girl’s health, and then to a psychotherapist, whom she began to see regularly. Nothing, however, seemed to work, and in August 2010 the five-foot-seven-inch girl was admitted to the hospital weighing just ninety-one pounds. After gaining twenty-five pounds in the hospital over a period of several months, she was released to her family and sent home for Christmas. Unable to return to school until the next academic year, she took a part-time job three miles from home. Six weeks later she collapsed and was rehospitalized. That’s when her parents found out that instead of taking public transportation she’d been walking three miles to work and back and not eating the lunch her mother packed for her each day. She suffered from a perforated ulcer and needed surgery, which her doctors were not sure she’d be strong enough to survive. She did, but within days her major organs started to fail. A collapsed lung, paralysis, and brain damage ensued. On March 26, 2010, she died of a heart attack at age sixteen, barely more than a year after she and her mother had decided to lose a few extra pounds.
While the acute and immediate symptoms of anorexia or binge eating and purging are troubling, the diagnoses involve another major risk: some studies show that almost half of teens with anorexia nervosa have considered suicide, and almost 10 percent have actually attempted it! Indeed, a recent study from Germany published in 2013 showed that half of all teens with anorexia had some other psychiatric diagnosis, especially depression. The researchers suggested that early treatment of the eating disorder may prevent the onset or reduce the severity of the later-life psychiatric disorder. So, just like conduct disorder, anorexia is another red flag. You need to get on top of it, as uncomfortable as it may feel, and alert your pediatrician about the symptoms you are seeing.
Depression is increasingly recognized as a growing problem in teenagers. The overall prevalence of depression during adolescence is higher than in childhood. Mood disorders in general, including depression and bipolar disorder as well as anxiety disorders, are the most frequently diagnosed psychiatric conditions in teens. Between 20 and 30 percent of adolescents report at least one major depressive episode, and that’s enough to bump up the risk of an adult episode considerably. In fact, researchers have found that the risk of an adult episode of depression increases even if a teenager experiences only depressive symptoms and not a full-blown clinical episode.
However, adolescents and adults differ in how depression is manifested. Adolescent depression is more likely to be chronic and is associated with a thirtyfold increase in the risk of suicide. Also, while adults frequently withdraw from friendships when they are suffering from depression, teenagers often spend even more time with their peer groups. This is probably a function of the fact that teenagers not only are more social at this stage of their lives but also believe only their friends can understand the depth of their pain and suffering.
There are two other significant, postdiagnostic differences between adolescents and adults with regard to depression. More positively, depressed adolescents who take medication appear to improve more rapidly than adults and are more willing to believe in that improvement. On the downside, with regard to medication, scientists have determined that teens can react differently from adults to standard antidepressant medications, such as Prozac, Zoloft, and Wellbutrin, and have a greater risk of developing suicidal thoughts and behaviors. These drugs belong to a class called selective serotonin reuptake inhibitors (SSRIs), which boost the neurochemical serotonin in the brain.
A colleague of mine once shared the story of a friend and her husband who had two boys, both in their early teens. The older boy was depressed and put on Zoloft and then sank into suicidal despair, which they believed was a result of the medication. One day, with his younger brother in the next bedroom, he hanged himself in his closet. As he died of strangulation, his feet reflexively kicked out and banged against the wall, noises heard by his unwitting younger brother on the other side of that wall. Ten years later, at the age of twenty-four, the younger brother, who was then on antidepressant medication himself, also hanged himself. It’s impossible to know if one or both boys suffered a reaction to psychiatric medicine. Even if just the older one did, the effect of having his brother kill himself in the next room could have been enough to negatively affect the younger and poison his entire future, making a suicidal depression almost inevitable.
Today the FDA includes a “black-box” label warning with all antidepressants directed at young people. Those meds include two SSRIs, Prozac and Lexapro, which were specifically approved for the treatment of depression in children and teenagers.
Sudden changes in mood, action, thought, behavior, and feelings, especially if they’re severe, may signal an adverse reaction to the antidepressant and every clinician who prescribes these drugs to adolescents is required to make the risks clear to both patients and parents. Fortunately there are also atypical antidepressants that work differently from SSRIs and can be prescribed for mood disorders in children and adolescents.
Between 20 and 60 percent of adults with bipolar disorder experienced the initial symptoms of the illness before they turned twenty. Teenagers diagnosed as bipolar also present a range of symptoms different from those of adults. Adolescents have fewer episodes of pure mania and more mixed episodes of both mania and depression. Adolescents are more likely to exhibit irritability and aggressive behavior as part of the manic or depressive phase of the illness. They also have more psychotic features, such as paranoia, during the acute manic phase. Teens experience more rapid cycling than adults, with shorter durations between manic and depressive episodes, and have higher rates of dual diagnoses, suffering multiple mental health problems such as substance abuse as well as bipolar disorder.
Mania and bipolar disorder are not as common in teens as simple depression, with less than 1 percent of kids ages eleven to eighteen being diagnosed with these illnesses. However, when it is present, the onset of bipolar disorder appears most commonly in the midteens. Also, there is a gender imbalance, with depression being more common in girls than boys.
Whether antidepressant medications are involved or not, suicide remains the greatest danger of a troubled teen’s life and is one of the leading cause of death in adolescence and early adulthood, according to the CDC. A nationwide survey of high school students shockingly revealed that 16 percent of kids reported at least contemplating suicide and 8 percent actually attempted it. Girls attempted suicide about three times more often than boys, but boys were more often successful, a fact thought to be due largely to their more frequent use of firearms. The rates are frightening when you think about access to the Internet, where information about how to commit suicide is sadly and distressingly available for anyone to read.
When it comes to suicide, too often the refrain from parents and teachers is that they didn’t know what was going on in the teen victim’s mind. That’s especially difficult when an adolescent is deceptive or simply secretive about his or her innermost feelings, but that’s all the more reason why we have to engage our children on a daily basis in order to know what’s going on in their lives—and in their minds.
Perhaps not even that, however, could have prevented what happened to Elizabeth Shin, a nineteen-year-old college student from New Jersey. On Sunday, April 9, 2000, the day before she took her own life by setting her clothes on fire, Shin lit a few candles in her dorm room at the Massachusetts Institute of Technology in Cambridge, Massachusetts, then sat down in front of her computer and began typing in her journal. “Yoga chick,” she wrote, referring to the exercises she often did to relax and take her mind off her studies. “Unfortunately I can’t spend all of my life in a yoga position. Or, maybe I can?”
It was a lighthearted entry, nothing to be alarmed about, and certainly no indicator that just one night earlier she had contemplated plunging a knife into her chest. After joking about yoga, her journal suddenly turned dark. She wrote the beginning of a poem to her ex-boyfriend, who had just broken up with her, in which she asked, “May I have white roses when I die, my love? / Will you place them at the head of my grave?” Then, as if catching herself, she suddenly switched back to being the astute, objective observer, playfully making fun of herself: “Uh oh, I am in a morbid mood. I only write death poetry (bad unpoetic stuff at best) when I am morbid. . . . Here I am, typing away aimlessly, hoping to exorcise my demons. Rats. It’s turning out to be more like exercising them. Are my demons in better shape than me?”
Later in the day, her parents and younger sister paid her a surprise visit, having driven up from their home in New Jersey to deliver a TV, cases of spring water, and boxes of cereal and lo mein. At dinner that night with her family at a local Chinese restaurant, she spoke about needing to get passport photos for a trip in the summer to her parents’ native South Korea. She also asked her little sister to come up and spend a weekend with her soon. The family returned home. Elizabeth returned to her room, and later that night she told a friend she wanted to kill herself by taking a bottle of Tylenol with alcohol. Instead, she fell asleep. Twenty-four hours later, though, one of Elizabeth’s parents picked up the phone. It was an official from MIT calling in the middle of the night. “There’s been a fire,” the voice at the other end of the line said.
There are few things worse than the death of a child. There are few things more horrible than the death of a child by suicide. Elizabeth Shin’s self-immolation was unusual and ordinary all at the same time. It was unusual in how she killed herself; it was ordinary in that it was impulsive and yet thought out, the product of teenage angst and yet also genuine depression. Most of all, it was the result of a young woman unable to see beyond the walls of her own misery.
In 2010, I was a board member of the Society for Neuroscience, one of the largest professional groups of its kind in the world. In San Diego, at our annual meeting, I had the privilege of meeting and talking at length with the actress Glenn Close, star of such movies as The Natural, Fatal Attraction, and The World According to Garp. We invited Glenn to give a keynote address because of her involvement with mental health issues and advocacy of neuroscience research. Glenn is warm and affable and down-to-earth, and she has a great sense of humor. She’s also tireless. In 2009 she helped found the nonprofit organization Bring Change 2 Mind, which helps to foster a better understanding of mental illness. All of it, she told me and a captivated audience of neuroscientists that day, sprang from a deep well of familial commitment:
“I’m the twelfth generation of a stiff-upper-lipped, pull-up-your-socks, do-it, don’t-talk-about-it, for-God’s-sake-don’t-show-anything, work-hard, don’t-whine, make-money, don’t-spend-it, win-on-the-playing-field, know-how-to-play-backgammon-bridge-and-golf, be-great-at-cocktail-parties Connecticut Yankee family,” she said. “We are also a family who had absolutely no vocabulary for mental illness.”
The push for Glenn came when she realized her adored sister Jessie and nephew Calen were both engaged in what she called a “life-and-death battle with bipolar disorder and schizoaffective disorder.” There were signs, decades earlier, she said, when her sister suddenly developed behavioral and emotional problems in high school. Jessie, like Glenn, attended the private school Rosemary Hall (now Choate Rosemary Hall) in the early 1970s. She experienced severe mood swings and often acted impulsively when she was in her manic state, taking, for instance, a dare from classmates and sliding the dorm mother’s cat down the laundry chute. The mood swings affected her studies, and she was forced to repeat the ninth grade. After she dropped out in the tenth grade, her life spiraled downward. There were suicide attempts and hospitalizations and then multiple marriages. Only when she was forty-five was she finally properly diagnosed and medicated.
Jessie also spoke at the conference and explained how when she was a teenager neither she nor her family really understood what was happening. What surprised her is that, years later, as a mother struggling with her own mental illness, she failed to recognize the symptoms in her son Calen.
“Mental illness is not easy to spot when you have no experience with it,” she said. “In 1999, when Calen was sliding down into the hell of [mental illness], I thought he was simply being a trying teenager. Calen is my eldest child so I had no clue what was the norm. If only I’d known some of the warning signs. All I knew was that Calen wasn’t Calen anymore. I’ll always look back with shame and guilt that I had no idea what was happening to my son or what kind of help he needed.”
Calen also spoke at the conference and said he thought the timing of the onset of schizophrenia is very cruel because it usually comes precisely at a moment when peer groups (that is, other teenagers) have limited empathy and self-awareness, and hence are not able to be supportive. The resulting social isolation adds insult to injury and at the worst time possible: smack in the middle of adolescence. Calen today is in his twenties, and his mother says she recognizes now, in retrospect, that her son’s symptoms when he was a teenager were not adolescent angst at all but rather the first signs of an underlying mental illness.
The overriding indication that Calen’s moodiness and withdrawal were not typical teenage behavior was his delusion that he was either Jesus or “the most evil thing walking the earth.” Brought by his father to the emergency room of a local hospital in Helena, Montana, where they lived, he kept repeating “blue square, red square, blue square, red square . . .” as he stared at the geometric patterns of the emergency room wallpaper. It was a code, he said, to help get him back into “reality.” Once he was admitted to the locked psychiatric ward, he thought he would have to fight his way out:
I began to prostrate myself, praying for God to let me endure the fight that I would now have no choice but to take part in. For whatever reason on that day I thought I was now going to be forced to fight for my life. Security guards were called on to the unit as I was obviously needing to calm down. Sensing I was in danger, I grabbed the chair from the common room and stood with my back facing the wall. A nurse rushed past me to close and lock an open door, I was now cornered, and it took four guards to pin me down and restrain me by my arms and legs.
When I was fighting the guards, I looked up and saw an older man standing close by with a white beard and hair. I kept begging him for help, thinking that he was God, and I didn’t understand why he wasn’t intervening. But it wasn’t his battle, it was mine. They carried me and four points [restraints] strapped me down to a bed, finishing by injecting me with a strong dose of Haldol, and I passed out.
Schizophrenia is less common than either depression, bipolar disorder, or anxiety disorder, but it is not rare; it affects about one in one hundred people. Interestingly, the brain has to reach a certain level of maturity before it can manifest schizophrenia. The disorder commonly first shows up in a person’s late teens or early adulthood. The warning signs can be similar to depression in that kids can appear withdrawn, socially isolated, and sad, with changes in their eating habits and hygiene. However, there are a few distinguishing features, which can include the presence of hallucinations, strange speech patterns, and psychosis, and psychosis, in turn, can be a highly agitated state along with paranoid behavior and delusions of persecution or grandeur. There is a schism, or detachment from reality, and that is where the word “schizophrenia” comes from. There is no actual split personality, however; schizophrenia is more a disconnection from the real world. Schizophrenia is a chronic condition, and treatment is essential, especially when a young person is still early in the disease process.
Hallucinations should make you worry about schizophrenia, but much more common causes of hallucinations, especially in teenagers, are the drugs LSD and PCP, and even large quantities of more commonly used substances such as alcohol and marijuana. The difference is that the person who is under the influence of drugs will also show signs of sedation, lack of coordination, and confusion. Hallucinations in schizophrenia are not accompanied by these symptoms or side effects.
While stress is one of the main risk factors for schizophrenia, as it is for mood and anxiety disorders, there are at least two others: advanced paternal age at time of conception and frequent marijuana use in adolescence. Researchers at the Netherlands Institute of Mental Health and Addiction carried out a study following two thousand subjects through adolescence and found that use of cannabis in the early teens can hasten the onset of psychosis and increase the risk of schizophrenia. Those most at risk were adolescents who had an immediate family member with schizophrenia or some other psychotic disorder. Even without smoking pot, teenagers with a family history have roughly a 1-in-10 chance of developing the condition. Marijuana use, though, doubles that risk to 1-in-5. Teens with no family history, the researchers found, have a 7-in-1,000 chance of developing a psychotic illness, which doubles if they smoke pot on a regular basis.
Besides psychosis, strong negative emotions and behaviors such as extreme loneliness and apathy may be indicators of more than a passing teenage mood, especially if those emotions and behaviors last more than two consecutive weeks. If they also cause your teenager’s grades to fall off the map or if he refuses to get out of bed and misses school, these, too, are indications of a possible underlying psychological disorder.
So what actually happens in the brain of an adolescent when mental illness is triggered? The chief culprit is stress, which we talked about in the preceding chapter. As adolescents’ brains are maturing, their HPA axis, the hypothalamic-pituitary-adrenal axis, the body’s chief stress-response mechanism, gets a workout. Researchers have found that clinical depression seems to emerge from a gradual dysregulation of the HPA axis from childhood into adolescence caused by a greater-than-normal release of cortisol in the brain. These higher-than-normal levels of cortisol both precede and predict the development of depression in adolescence and early adulthood. Why some people release more cortisol than others is not yet fully understood, and while there is no physiological or biological test for depression, researchers are hoping to develop one. Salivary cortisol can provide a good index of stress and can be collected noninvasively by having a patient drool through a straw into a collection cup while undergoing a stimulus. While not likely to be definitive, the test could become an aid in determining what psychological processes are at work in a patient who develops major depression.
Anxiety, like depression, is a frequent complaint of adolescence, and it often doesn’t take much for simple nervousness, restlessness, or fear to become a full-blown anxiety disorder. Many times adolescents will describe chronic feelings of uneasiness without knowing the cause and with no apparent immediate threat or stressor. Teens, by nature, worry a lot and are prone to being restless and irritable. To be characterized as a disorder, however, the anxiety must interfere with normal functioning. Excessive worry can cause a teenager to withdraw from daily activities and become shy and hesitant to engage in new experiences. In addition, excessive worry also can push a teenager in the opposite direction, toward more risk-taking, drug experimentation, and unprotected sex as a way to overcome, diminish, or simply deny the fears. In some cases, the excessive anxiety will produce physical symptoms, too: headaches, stomachaches, fatigue, trembling or sweating, even hyperventilation.
Among adolescents diagnosed with anxiety and impulse control disorders, between 50 and 75 percent show the first signs of the disorder during adolescence. There are a number of anxiety disorder subcategories, too, as set forth by the National Institute of Mental Health, which are not specific to adolescents.
The chief difference between teens and adults who suffer from an anxiety disorder is the source of the anxiety. For adults, anxiety usually emanates from problems with health or money, difficulties at work, and family issues. For adolescents, it often has to do with friends and school—social acceptance, academic performance, etc. The difference between those with ordinary teenage angst and those with bona fide anxiety disorders is one not of content but of degree. In a 2000 study of youths being seen at an anxiety disorders clinic, patients’ answers to a question about what worried them most frequently and most intensely were not much different from the answers of youths without an anxiety disorder.
Their top-five most frequent worries:
1. Friends
2. Classmates
3. School
4. Health
5. Performance
Their top-five most intense worries:
1. War
2. Personal harm
3. Disasters
4. School
5. Family
What is different between teenagers with an anxiety disorder and those with just normal stress is the level and constancy of the stress. In imaging studies of the brains of adolescents diagnosed with anxiety disorders, there is always more activity in the limbic system, in the fear and emotion parts of the brain, particularly in the amygdala, than in normal control subjects. Researchers have consistently found a positive correlation between amygdala activity and anxiety, but whereas depression is associated with the left amygdala, anxiety disorders are specific to the right amygdala, which is responsible for detecting emotional stimuli.
By nature, adolescents already have fairly overactive amygdalae, which means they really need their prefrontal cortices to exert even greater control. For teens at risk of an anxiety disorder, however, their still-maturing brains are not yet able to exert that kind of top-down control. For that to occur, brain regions need to “talk” to one another, and there is evidence in animal studies that adolescent brains aren’t doing as much “talking” as adult brains. This is due to the relative lack of myelin covering the connecting tracks, resulting in signals not traveling fast enough between brain areas.
Adolescent girls are more liable to suffer anxiety and mood disorders than adolescent boys. Teen girls report not only more stressors in their lives than boys, but also greater distress in response to those stressors. This sensitivity may be enhanced because the typical girl, with her enlarged midline connectivity on the undersurface of her frontal lobe, is more attuned to social and interpersonal relationships at this stage. In 2009 researchers at the National Institute of Mental Health reported that just when sizing one another up, girls show more brain activity in certain emotional circuits. At a time when adolescent girls are more and more concerned with how they are viewed by their peers, interpersonal stress can play a large role in the development of an anxiety disorder.
Teenagers with high levels of anxiety, whether or not they’ve been diagnosed with a disorder, will often try to self-medicate. In 2011 a group of Finnish researchers were engaged in an ongoing study called the Adolescent Mental Health Cohort that included 903 boys and 1,167 girls ages fifteen and sixteen. As part of their research, the scientists looked at rates of drinking, especially in relation to those who had been diagnosed with an anxiety disorder. Four percent of the more than two thousand male and female Finns in the study had such a diagnosis. At the start of the study only 10 percent of the teens reported drinking alcohol on a weekly basis. However, after just two years, 65 percent of the anxious youths said they were weekly drinkers; this amounted to a threefold increase in risk. (The study did not look at the differences between male and female adolescents.)
The vulnerability of a teen to emotional and psychiatric issues cannot be overemphasized. The teenage years are a developmental stage whose by-products are a hypersensitivity to stress, an inability to exercise self-analysis or insight, and membership in a peer group equally unable to interpret warning signs or to offer adequate empathy. Here is a major opportunity for the adults around teenagers: Be vigilant, exercise your own well-developed skill sets to ask questions, probe, stay connected, and, most important, have a low threshold to seek medical advice or counseling for symptoms that appear to change from the ordinary. Also, as kids these days spend so much time online, isolated, warning signs could be harder to detect. Kids sit alone in their rooms on the Internet and the phone. Years ago, social isolation was quite easy to notice: a kid sitting alone in the cafeteria, on the school bus, or on the top bench of the bleachers. Now moderate physical isolation is a natural consequence of online social interaction, making it much more difficult to detect. But, as a parent, you don’t know until you check. Be part of your kids’ lives at home. Don’t count on your teenager—or his or her friends—to sound the alarm.