11
Stress
Barely a day goes by when parents and teachers of teens don’t witness an outburst of anger, tears, poutiness, withdrawal, irritability, even hostility from their mercurial kids. On the other hand, adolescents are prone to overexcitement and bursts of enthusiasm. The question often is, how do we know when things have become too extreme? How do we distinguish between episodes of normal teenage angst and something darker, more troubling? It is difficult enough to find out what our kids had for lunch at school, let alone get them to admit to depression or anxiety. And then actually getting them to articulate it, to talk about it—well, that seems like a very tall order!
Emotions are the barometer of mental well-being. It isn’t hard to remember the devastation I felt when a boyfriend broke up with me in high school or I didn’t get the grade I wanted in a class in college. Nor can I forget my euphoria when I learned I’d been accepted into medical school. A world without emotion is, frankly, difficult to imagine. During adolescence, more than at any other time, emotions rule our lives. Teenagers are usually up or they’re down, and they are very rarely something in between. As parents we sometimes experience our teenagers’ emotional highs and lows as frighteningly out of control, and because our teenagers are as yet unable to smooth things out using their frontal lobes, it’s up to us to be the filter, the regulator, to provide the sense of calm their brains can’t yet provide.
So when and how do we know whether an emotional outburst or mood swing, an impulsive act or even a severe disappointment, is normal teenage behavior or something we should worry about, like the first sign of depression or an anxiety disorder? There are signposts and degrees and ways of making these distinctions, but before we dive into them, you first need to understand what emotions are—and are not—when it comes to adolescent development.
In large part what makes adolescence so difficult is that much of a teenager’s response to the world is driven by emotion, not reason. Adults aren’t the only ones who know this; teenagers do, too. Often they describe their lives as a “drama” that can be either “too awful” or “too wonderful” depending on the circumstances. The emotional lives of all human beings are closely tied to the working of the amygdala, from which arise our most primal feelings and reactions—fear, anger, hate, panic, grief. Emotionally, the main difference between adults and adolescents is that there is much less activity in the frontal lobes of adolescents, making it harder for them to handle their emotions, especially in crisis situations.
In Chapter 1, we learned that teens may be less protected against stress compared with adults because of the way they respond to the stress hormone THP. Instead of a calming effect, the hormone stirs up additional anxiety in the teen. Stress can be induced internally, by thoughts and emotions, or externally, by the environment. Teen brains are different from adult brains in another way as well. Because teens are not fully accessing their frontal lobes, other areas of the brain can get a little out of hand and create more extreme impressions of an external threat. Primal feelings, like fear, are produced by what’s called the hypothalamic-pituitary-adrenal axis (HPA). Faced with a stressful situation, the amygdala is the first to respond, and when stimulated, it releases stress hormones that signal the pituitary gland to release certain chemicals, which then prompt the adrenal gland to release adrenaline (also known as epinephrine). The adrenal glands are located right above the kidneys, and when activated in highly stressful situations, they put the body in position to respond to danger by raising the heart rate, dilating blood vessels, increasing oxygen, and redirecting blood away from the digestive tract and into the muscles and limbs in order to run away. If the instinct is to stop and defend, then our pupils dilate, our vision sharpens, and our perception of pain decreases, all in the service of preparing us for “battle.” In this state of high alert, every stimulus is a possible point of danger and the body is ready for it. The threats to immediate survival are far fewer today than when our primitive ancestors roamed the earth, but the fight-or-flight response remains encoded in our genes. Adolescents, whose amygdalae are less under control by their frontal lobes, are prone to responding to situations of stress with more extreme emotions than adults, who can rely on their prefrontal cortex within the frontal lobes to control their anger and fear.
Besides adrenaline, a second neurochemical, cortisol, contributes to an adolescent’s emotional cauldron. Normally, cortisol fluctuates over a twenty-four-hour cycle, with the highest levels occurring in the morning upon awakening. Those levels increase 50 to 60 percent throughout the day before dropping, at first rapidly and then more slowly, for several hours in the afternoon and evening until a low point is reached around midnight. Studies have found that in mid- to late adolescence, and especially in girls, cortisol levels are slightly higher than in the normal adult population. Negative emotions—stress, worry, anxiety, anger—have all been significantly associated with higher levels of cortisol. So, too, has loneliness; and this is why in adolescents being alone is also associated with increased anxiety and stress.
Heightened emotion goes hand in hand with stress, and the stressors for adolescents are everywhere—from speaking in front of a class to peer rejection and bullying. The effect of stressful experiences and emotional trauma on adolescents can have serious consequences for mental and emotional health later in life. Stress in adolescents works differently from stress in adults, and the effects of stress on learning and memory in teenagers can predispose them to mental health problems, including depression and post-traumatic stress disorder (PTSD). Substance abuse also often develops, when stressed kids start self-medicating by taking stimulants or antianxiety drugs they sneak out of bottles in their parents’ medicine cabinets. Anxiety is astronomically high in kids today, with a host of societal issues, less consistent family life, and exposure to all sorts of stimuli on the Internet, not to mention the vagaries of social networking. These are otherwise good, normal kids, but stress can seriously strain their ability to cope.
Stress is terrible for learning. You know what I mean. A little pressure can be motivating, but once you pass beyond that, stress contributes to inattention and a real inability to learn. We have all seen a nervous kid in the midst of a spelling bee: the kid freezes, and an otherwise easy word becomes insurmountable. This “freezing” of memory is real. The hippocampus, for one thing, basically stops functioning normally. Why? The surge of cortisol during a stress response can interfere with memory. Rats that are great at learning a maze under normal conditions completely freeze up and are unable to learn if a stressor, like a cat, is placed outside their cage. One of the brain structures that suffers the most damage in chronic stress is the hippocampus, critical to both memory and learning. The cascading effects on learning include impaired LTP and the elimination of synaptic connections.
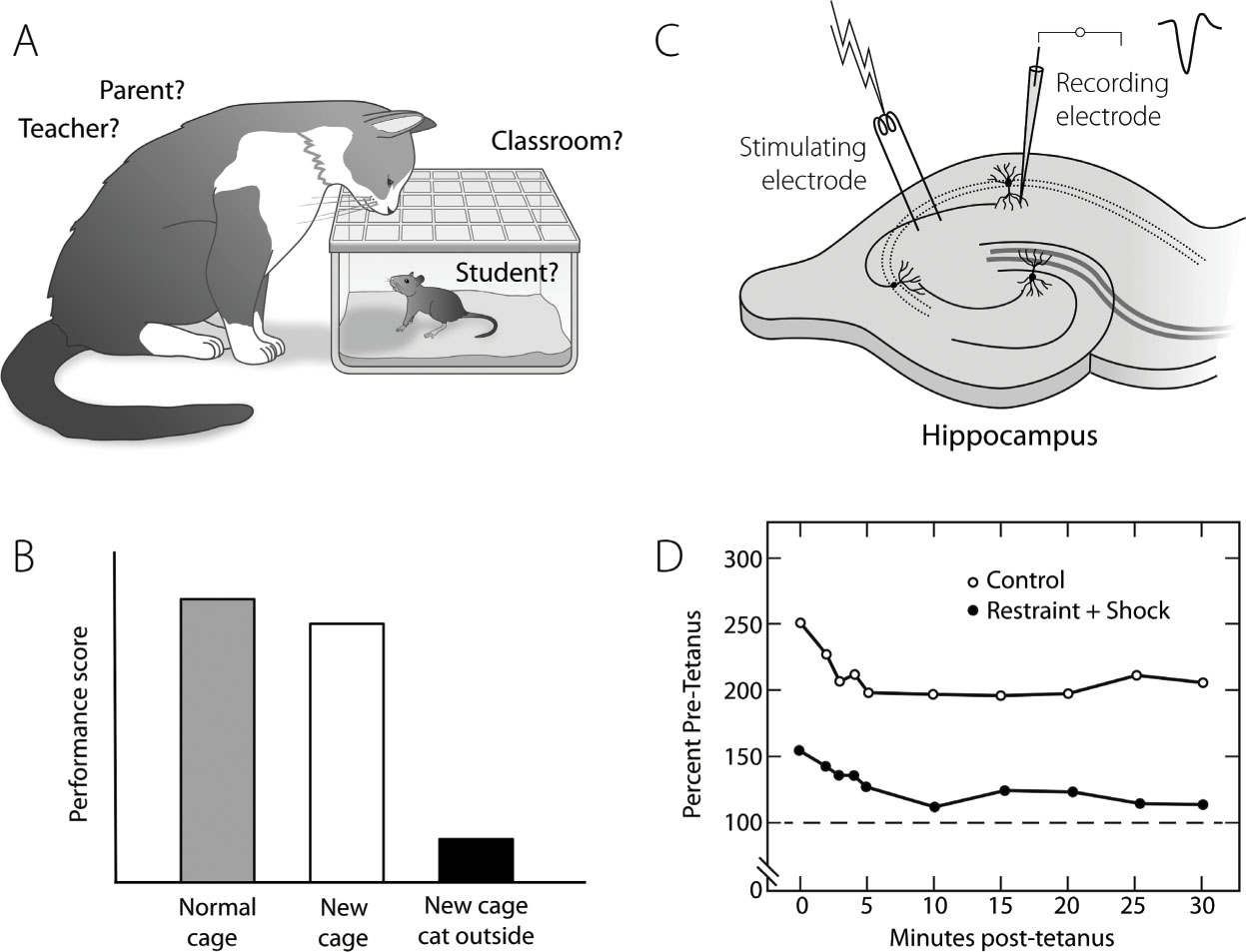
FIGURE 25. Stress Can Decrease Learning and LTP: A, B. Rats performed well when learning a task under normal home cage conditions and also when moved to a new cage. But as soon as a cat was placed outside the new cage, the rats froze frequently and were unable to learn. C, D. In hippocampal slices from the “stressed” rats, burst stimulation elicited much weaker LTP than in those of the control group, demonstrating the effect of stress hormones on synapses.
We need to be mindful of what our teenagers consider stressful and realize that school can sometimes be analogous to the cage in the rat experiment, and that parents and teachers can be as stressful as the cat in that research paradigm!
Generally speaking, when this happens, thinking becomes less flexible. In animal studies, researchers have found that the brains of adults, after a period of stress, bounced back within about ten days. In adolescent animals, however, the effects of the stress were delayed by about three weeks, indicating the effects were not only long-lasting but also possibly irreversible. This gives us pause when we consider human teenagers and all the stressors that can take them over the top.
How else does stress alter the brain? Research is just beginning to yield clues. Experiments in rats show that even adolescent rats can stress out. A group of McLean researchers in Boston found that when adolescent rats were exposed to social isolation, they tended to do worse on escape tasks and showed signs of what could be construed as “helpless” behavior. Males were much more severely affected than females. When their brains were examined, they showed decreased amounts of synapses as well as myelin, especially in the frontal lobes and hippocampi. The amygdalae appeared to increase in size, perhaps in an attempt to handle the challenge. Stress was clearly altering the maturation of their brains!
Stress is a big player when it comes to emotional trauma. Adolescents are at especially high risk for experiencing emotional trauma compared with the rest of the population, and the consequences for their brain development can be devastating. One large study in North Carolina in 2010 showed that a quarter of all adolescents by the age of sixteen have experienced a “high-magnitude” event or “extreme stressor,” including everything from a serious accident, an illness, or the death of a parent to sexual abuse, family violence, natural disaster, war, and terrorism. Low-magnitude events include parental separation and divorce and a breakup with a best friend, boyfriend, or girlfriend. A third of all the teens surveyed had experienced a low-magnitude event at least once in the three months prior to participating in the study.
Now that we can perform MRI scans on people and look at their gray and white matter, it seems that the same things may be happening in human teens exposed to stress as in the rats. The prefrontal cortex, hippocampus, and amygdala are major regulators of the stress response in humans, too. Like the rat’s hippocampus, the teen’s hippocampus appears to get smaller (not good for memory and learning), and the amygdala appears to grow in size. An increase in amygdala function may explain some of the exaggerated responses seen in PTSD.
When trauma is severe or prolonged, an adolescent is more prone than an adult to developing PTSD. Normally, PTSD develops when someone is exposed to an incident or event that threatens his or her personal safety or survival. One thing to remember is that normal adolescents, even without any abnormal stress, have exaggerated amygdala function and therefore increased stress responses. BJ Casey and her team at Cornell University’s Sackler Institute used fMRI to show brain activation in response to a fearful stimulus (a picture of a frightened face) in eighty people ranging from age eight to thirty-two. Her results showed that adolescents had much higher amygdala activation when shown stressful pictures than children or adults.
So stress on top of an already overactive stress-response system can create havoc in the teen brain. Without treatment, those who suffer PTSD can become susceptible to crippling fear and anxiety throughout the remainder of their lives. The symptoms and problems associated with adolescent PTSD include not only fear and anxiety but also sadness, anger, loneliness, low self-esteem, and an inability to trust others. Behavior problems associated with adolescent PTSD also run the gamut from social isolation and poor academic performance to aggression, hypersexuality, self-harm, and abuse of drugs or alcohol.
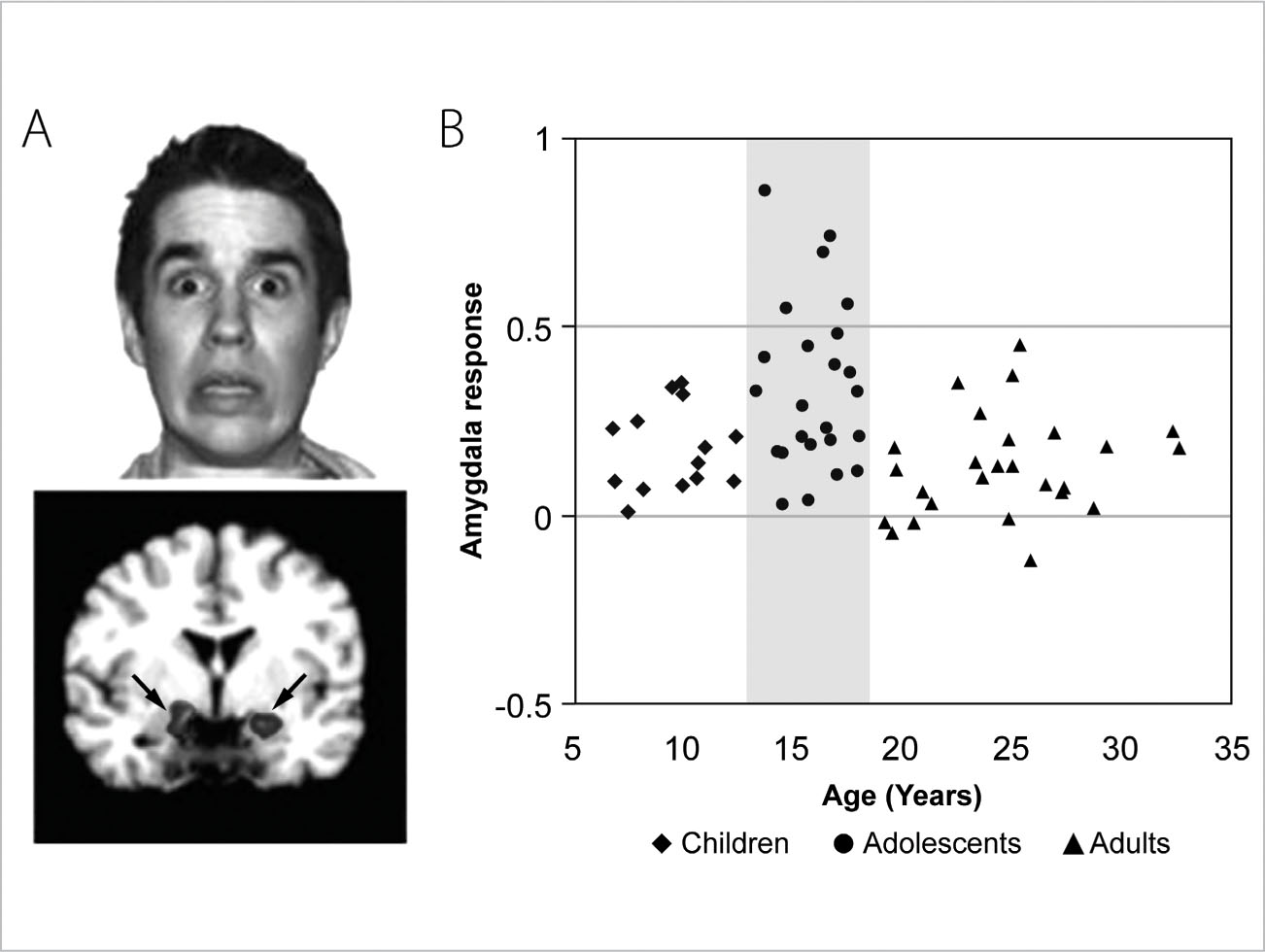
FIGURE 26. Enhanced Response to Fearful Stimuli in Adolescents Compared with Children and Adults: A. Researchers showed subjects faces with both frightened and nonfrightened expressions. B. Functional magnetic resonance imaging (fMRI) was used to determine activation of the fear circuitry in the amygdala. The adolescents’ responses were generally stronger than those of either the younger or the older subjects.
Teenagers as well as children suffering from PTSD are likely to reenact their traumas in their artwork, with toys, or in the games they play. They are also more likely than adult sufferers of PTSD to be impulsive and aggressive. Research suggests that something as simple as confronting another person’s fear or anger can trigger abnormally high activity in the emotional centers of the brain in someone suffering from PTSD.
Most people associate post-traumatic stress disorder with war veterans. In war, most combatants are men and women in their late teens and early twenties, and so their brains pay an even heavier price than those of older adults. Scientists at the National Center for Veterans’ Studies at the University of Utah found that 46 percent of those who had been deployed to Iraq or Afghanistan (the majority of whom saw combat) reported suicidal thoughts. This is exponentially higher than the 6 percent average of nonveteran college students who reported giving serious consideration to suicide. Young veterans were also seven times more likely to have made a serious suicide attempt than nonveteran college students.
For adolescents in general the two strongest predictors of PTSD are exposure to violence and the sudden death of a loved one, according to the American Psychiatric Association. And of the two, the unexpected death of a loved one is the more common. Nonetheless, researchers have found that health care professionals often overlook the potential for PTSD in adolescents, perhaps because this developmental stage is already marked by emotional highs and lows and other behaviors typical of adolescence, like rebelliousness, withdrawal, acting out, and depression. All of these, however, can also be indicators of PTSD. An important difference between adolescent depression and PTSD is that fear and agitation are more characteristic of PTSD than moodiness and withdrawal. Not surprisingly, anxiety disorders are more likely to develop in children and teens exposed to trauma.
Trauma and stress are harsh on the teenage brain, but stress-induced brain alterations can also occur years before adolescence, even in utero. In one study a majority of seventeen-year-old girls and boys whose mothers had experienced above-normal stress during pregnancy (divorce, loss of a job, death of a loved one) had higher-than-normal levels of stress hormones even at rest. While males are more likely than females to be exposed to traumatic stressors, research shows that females exposed to traumatic events are more likely to develop PTSD.
Severe and chronic stress also goes hand in hand with physical and emotional abuse. Researchers at University College London used fMRI to scan the brains of twenty children and young teenagers who outwardly appeared healthy but who had been maltreated, and then compared the results with those of healthy children who had not been abused. The scientists found that during the scans, when the maltreated children and teens were shown pictures of angry faces, their amygdalae and anterior insulae, known to be involved not only in threat detection but also in the anticipation of pain, showed heightened activity similar to that in a combat soldier.
Research from late 2011 also revealed that adolescents who suffered physical or emotional abuse or neglect had evidence of brain damage, even in the absence of a diagnosable mental illness. Scientists at Yale University found that adolescents had less gray matter in the prefrontal cortex if they’d been physically abused or emotionally neglected. Reduction of activity in the prefrontal cortex in these abused youths could interfere with their motivation and impulse control, as well as their ability to focus, remember, and learn. Adolescents who were emotionally neglected also showed decreased activity in the parts of the brain that regulate emotions. Of those teenagers who were physically abused, boys revealed a greater reduction in areas of the brain associated with impulse control and substance abuse, meaning they had a greater tendency to abuse alcohol and drugs, while girls had reduced activity in the areas of the brain linked to depression. The scientists stressed, however, that these deficits were not likely to be permanent, in large part because of the brain’s plasticity during adolescence.
What remains clear is that in today’s world there appears to be no end of stressors in the lives of adolescents, and with their increased exposure to news events through digital technology, it is truly impossible to protect children and teens from the seemingly daily presentation of mayhem, violence, and disaster in the news. Ameliorating the effects of trauma, then, is that much more important, especially when the traumatic event is also a public one and therefore in some sense experienced by many at the same time, as happened, for instance, when two bombs exploded at the Boston Marathon finish line in April 2013. More individualized trauma is really not any different. An example would be bullying—either in person or online. Teens are very susceptible to harassment and negative criticism, and may not have the ability to see the lack of fact or logic in the accusations made by a bully. Schools and parents must take bullying seriously: it is not trivial for the victim.
The American Psychological Association suggests a number of ways to help adolescents in the immediate aftermath of a trauma that becomes public:
• Create a safe place for adolescents away from onlookers and media.
• Kindly but firmly direct adolescents away from the site of violence or destruction, the severely injured, and any continuing danger.
• Provide support to adolescents who are showing signs of panic and intense grief, such as trembling, agitation, refusing to speak, loud crying, or rage. Stay with them until they are stabilized.
• Help adolescents feel safe with supportive and compassionate verbal and nonverbal communication. Reassurances are very important.
• Provide information about the traumatic event in language adolescents can understand. This will help them to understand what happened and feel more in control.
The flip side of adolescents’ vulnerability in the face of trauma is their resilience, which was also witnessed in the cases of some of the teenage victims of the bombings who attended high school proms and returned to college classrooms just weeks and months after the traumatic events. Resilience isn’t something you’re either born with or not. It’s actually something that’s learned, and for that reason teenagers, while particularly vulnerable to the negative effects of stress, are also better equipped than most adults to learn how to positively respond to stress. As an adult you are in a position to convey that information to your teenage sons and daughters, to tell them to take care, take control, and take time out. They can take care of themselves physically by eating right and getting enough sleep. They can take control of their lives by setting goals, even small ones, and working toward them one step at a time. And they can take time out from the Internet, from texting, from Facebook, and instead talk out their problems with a good listener they trust.
You have to be wise enough and mature enough to know that this “good listener” might not be you but could be another adult figure—an aunt, an uncle, a grandmother or grandfather, even a levelheaded friend their own age. Whether or not the adult your teenager can confide in is you, what is indisputable is the importance of adults and healthy family functioning in the lives of adolescents, especially when those adolescents are experiencing extreme stress.