10
Hard-Core Drugs
It takes only a single bad decision to result in catastrophic consequences, as it did for Irma Perez, a fourteen-year-old California girl, on April 23, 2004. According to her sister Imelda, Irma was at a party where she was offered a single pill of MDMA (3,4-methylenedioxymethamphetamine), a synthetic stimulant and mild hallucinogen also known as Ecstasy. Immediately after swallowing the drug, she became sick, “vomiting and writhing in pain,” but her friends, afraid of getting into trouble, delayed calling 911 or taking her to an emergency room for hours. Instead, as Imelda wrote on www.nationalparentvigil.com, the website she helped found, they made the situation worse:
They tried to give her marijuana, thinking it would relax her and possibly help her because they had heard it had medicinal qualities. Irma suffered for hours and when she was finally taken to the hospital the next morning, she was in terrible shape. Five days later she was taken off life support and died. . . . How did Irma actually die? Dr. Leslie Avery and Dr. Peter Benson, a forensic medical expert, say that Irma’s brain swelled from a lack of oxygen. “Her cerebellum dissolved as her brain tried to escape its confined space,” Benson said (in a San Mateo Daily Journal article).
Every year since 2006, hundreds of ordinary Americans have gathered for a somber, candlelit ceremony in front of the headquarters of the Drug Enforcement Agency in Arlington, Virginia. The name of the event, begun by eight couples, is the Vigil for Lost Promise: Remembering Those Who Have Died from Drugs. Those in attendance on this one night every year are mostly parents, brothers and sisters, aunts and uncles, nieces and nephews, but many are just friends who gather in remembrance of someone they loved. An overwhelming number of those whose memories are honored each year were in their teens or twenties when heroin or cocaine or prescription drugs took their lives. More than 150 names are inscribed on a virtual wall on the website of the Vigil for Lost Promise. All of them were victims of drugs; all of them are deceased.
After a decade of steady decline in drug abuse, a national survey cosponsored by the Partnership at Drugfree.org and the MetLife Foundation in 2011 revealed that the use of Ecstasy had risen 67 percent among teens. Originally patented as an appetite suppressant, Ecstasy, which is usually ingested in tablet form, is currently not approved for any medical use or treatment. It is also known as molly, which is the pure form of MDMA, and it remains popular with teenagers and young adults because it is thought to enhance sex, heighten emotions, and confer a feeling of connectedness with others. Though the government classified molly as a Schedule I controlled substance—the category for drugs with high abuse potential, no medical use, and a possible fifteen-year jail term for illegal possession—it gets used a lot at raves where electronic dance music (EDM) is played, especially in Europe. An MDMA high is called “rolling” by music ravers and is essentially a prolonged state of euphoria in motion, which goes hand in hand with electronic music and its nonstop, almost hypnotic, pulsing beat. A too-powerful form of the drug can be lethal, and because people don’t know what they are getting when they buy it, they sometimes bring testing kits to raves.
The negative side effects of Ecstasy are considerable—confusion, agitation, irregular heartbeat, seizures, sleep disorders, liver and brain damage, and of course death. In fact, in September 2013 two young people died at New York City’s Electric Zoo music festival and four others were hospitalized as a result of taking MDMA. Though general admission tickets for the three-day concert cost $179 a day, promoters canceled the final day because of the deaths and issued refunds. The last thing that twenty-year-old Olivia Rotondo said before collapsing in front of a paramedic was “I just took six hits of molly.” Hours later she was dead.
Short of these lethal and unpredictable effects, regular use of the drug has been found to impair short-term memory and learning as well as the production of serotonin, vital to the regulation of mood. In a 2008 study, Dutch researchers found sustained damage from Ecstasy on white matter maturation and hippocampal development in both humans and animals, even in low doses. Because white matter is still being laid down in adolescence, the brains of teenagers are more susceptible than adults’ brains to the destructive effects of Ecstasy. Ecstasy’s toxicity to serotonin cells, in particular, suggests even more disruption of memory and mood. In rats exposed to amphetamines during their “teens” and then tested in adulthood, working memory was found to be significantly impaired and prefrontal cortex function disrupted. These effects were not seen in rats exposed to amphetamines in adulthood only. Confounding the problem for adolescents is that while they seem to have greater neuronal responsiveness to cocaine and methamphetamines than adults, they have less sensitivity to some of the physical side effects, especially motor coordination. It’s no wonder that studies also show that a key predictor of addiction is reduced sensitivity to these undesirable physical side effects. An adolescent who doesn’t have a negative reaction the first time he or she takes drugs is much more likely to take those drugs again—and again and again and again.
The issue with MDMA is not only the immediate effects. It turns out experimental laboratory research shows that adolescent brains exposed to MDMA undergo changes in their synapses in almost every system you could imagine. These include systems for serotonin, and a lowering of serotonin can increase the risk for depression and stress response. Stress can in turn affect glutamate receptors that modulate learning and memory.
The research into how and why drugs like Ecstasy and cocaine are so dangerous for adolescents is turning up new findings every day. The basis of many of these findings is that with a still-maturing brain, teens are especially vulnerable to drugs that work directly on the brain’s chemistry. In new rat studies, adolescent brains have been found to be more susceptible to lower doses of cocaine and to suffer more severe symptoms. Their brains are also more motivated to work for the cocaine reward; this means they find it difficult to abstain, and so become addicted faster and harder than adult rats. They also relapse more easily. These results are all too pertinent for humans: nine out of ten addicts say they first used drugs before they were eighteen years old.
Adolescents process cocaine differently from adults. First and foremost, cocaine is a stimulant, but it stimulates a greater release of dopamine in the adolescent brain than in the adult brain. Two areas in the teen brain appear to be especially sensitive to the effects of cocaine: the nucleus accumbens, which, remember, is the reward center, and the dorsolateral striatum, where habits are formed. Dopamine concentrations in these two regions of the brain are greater in adolescents on cocaine than in adults. A researcher involved with rat studies at McLean Hospital, in Belmont, Massachusetts, likened these areas to a “biochemical express lane.” A similar study from Canada showed adolescent rats ran around faster than adult rats when exposed to the same amount of cocaine.
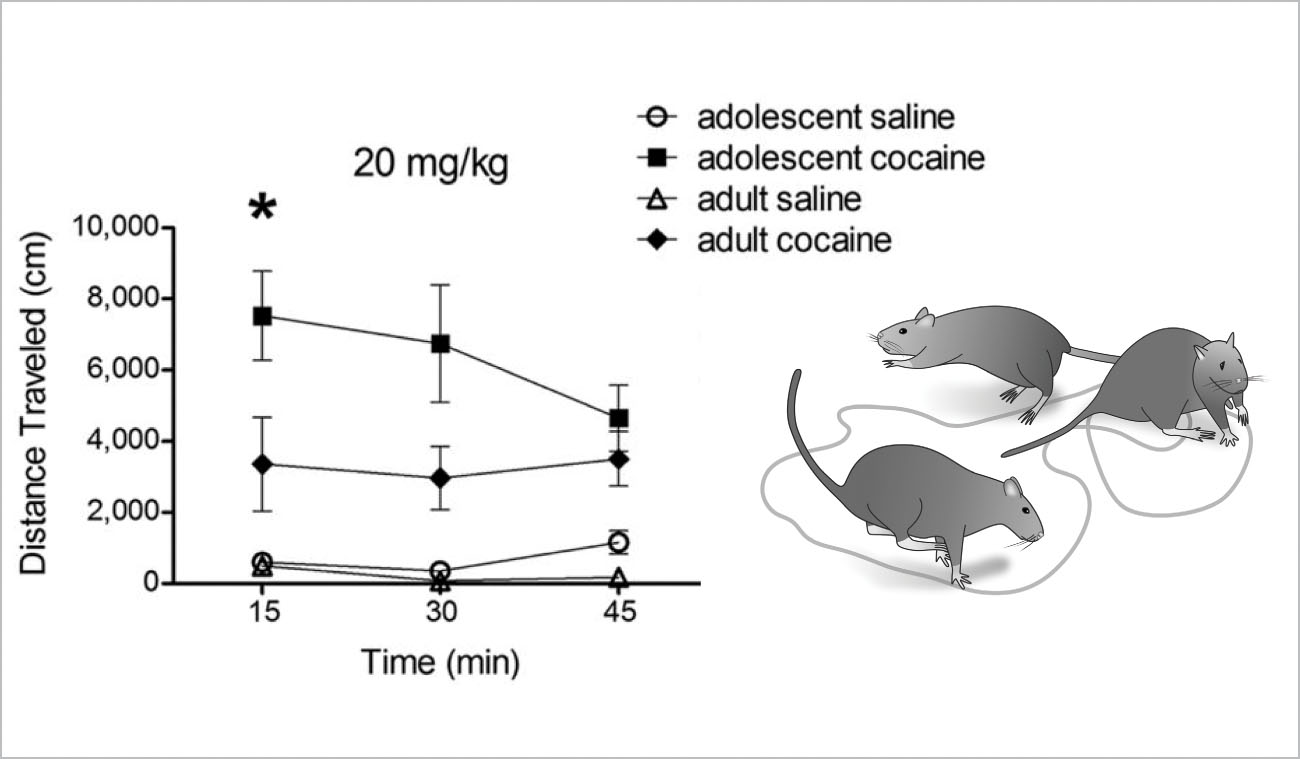
FIGURE 24. Enhanced Effects of Cocaine on the Behavior of Adolescent Rats: Cocaine makes both adolescent and adult rats run faster, but the adolescents travel farther than the adults.
Craving and relapse are hallmarks of drug addiction, and teens get hooked on drugs harder and faster than adults precisely because so many of the drugs target the very active reward system in their brains. Because the nucleus accumbens is still maturing during adolescence, its functioning is characterized by a search for the highest excitement with the least amount of effort expended. In fact, it takes less than three months for adolescents to transition from experimentation to weekly use.
Another concerning issue is that rat studies show the enhanced dopamine in the adolescent brain can actually change the way it processes information permanently, leaving the brain more susceptible to addiction in adulthood. Those researchers in Canada who showed that adolescent rats have a greater response than adults to the same amount of cocaine also found permanent changes in a host of structures, including the nucleus accumbens, striatum, insular cortex, orbitofrontal cortex, and medial forebrain bundle—all of which are implicated in addiction. What was equally concerning was that these changes were still present even after one month of abstinence, hinting at the permanence of cocaine’s effect.
Drugs like cocaine are the perfect brain temptation. Other popular stimulants include amphetamines and methamphetamines. A quarter of all high school seniors in America admit to having used a stimulant like speed, and in the Southwest and rural Midwest, amphetamine use by teenagers is double the national average.
Like cocaine, amphetamines and methamphetamines both increase the concentration of dopamine in the brain, and like cocaine both produce a euphoric high. Medications used to treat attention deficit hyperactivity disorder, abbreviated ADHD, are also increasingly being abused by teenagers. Typically, teens use the pills for non-prescription purposes, most often to stay awake late at night studying or for a boost of energy or concentration when doing homework or writing a paper. But because Ritalin and Adderall and Concerta—drugs used to treat ADHD—are stimulants, they are also capable of trapping adolescents in a cycle of habitual use and addiction.
In high schools across the country, the fastest-growing drug of abuse is heroin. It didn’t take long for Ian Eaccarino to become hooked on marijuana and other drugs, and he spent the better part of two years trying to get clean. On the Courage to Speak website, his mother, Ginger Katz, wrote about how quickly her twenty-year-old son became hooked on heroin.
Nine months before he died, Ian and two friends snorted heroin for the first time. He was a college sophomore at the time. One boy became scared, one became sick—and Ian liked it. When he finally went to drug rehabilitation, he told me: “Mom, there is a smorgasbord of drugs at college. If you don’t have the money, they would give it to you for free and then you’re hooked.”
It was Katz who found her son’s lifeless body in his bed the morning after he accidentally overdosed on heroin.
The evening before he died, I realized that he had relapsed. He knew that I was scared and that it hurt me so. He said to me, “Mom, I want to see the doctor in the morning and I don’t want to move in with my friends.” That was the deal. Later, he came upstairs and said, “I’m sorry Mom.” It keeps ringing in my ears. Never did I think he would go downstairs and do it one more time. Even with all the remorse, the drugs were bigger than he was.
Prescription drug abuse has been on the rise nearly every year for the past decade, with 15 percent of all high school seniors reporting nonmedical use of sedatives, especially the prescription drugs Valium, Ativan, Klonopin, and Xanax. Researchers at Rockefeller University found that adolescents exposed to OxyContin (the narcotic oxycodone) can suffer lifelong damage to their brains because of permanent changes in the reward system. As the adolescent brain prunes itself, OxyContin appears to trick it into keeping more dopamine receptors than it needs. Painkillers like OxyContin activate the brain’s opioid receptors and release more dopamine in the brain’s reward center.
The administrator of that rehab facility for teenagers in Connecticut I mentioned earlier in this chapter said he himself became an alcoholic at the age of just thirteen. Now middle-aged, he says he has seen many young kids end up on hard-core drugs after taking painkillers for a sports injury. As a society, we’re too soft on pain, he told me. Parents don’t want to see their kids hurting, so they make sure their son or daughter has a prescription for painkillers. So a kid might take Percocet, for instance, and continue taking it even when there is no more pain involved because there’s a bit of a physical addiction. Eventually the Percocet runs out, he explained, but you can get oxycodone on the street. Oxy, of course, is expensive, so when the person is offered much cheaper heroin, it’s hard to resist. But since this person doesn’t think of himself as an addict and would never shoot up, he snorts the heroin, which is ten times stronger and ten times cheaper than oxycodone. Before you know it, a kid with a sports injury is hooked on smack—and lost—and when he finally realizes there’s an even cheaper high in shooting up heroin, he’s hit rock bottom. It’s pretty grisly, but this rehab administrator says he’s seen it happen over and over again. How do you talk to teens about this kind of danger? I asked. He said they have to be ready to hear it, but the more you can get them to identify with other people it’s happened to, the more you can embed the stories of addiction into situations they can relate to, and then the easier it is to get the message across.
Adolescent addiction is particularly pernicious because over a long period of usage, the brain responds to the hyperactivity of dopamine by reducing dopamine receptors, and a loss of receptors means less stimulation. The result is called tolerance. The addict must take increasingly larger doses of the drug to obtain the same high he or she experienced the first time around. And with the reward pathways so hypersensitized to being stimulated, withdrawal also comes quickly and is more pronounced than in adults, leaving the teenage drug abuser susceptible to anxiety, irritability, and depression and therefore even more determined to get high again.
The chilling realization about drug use and adolescence is this: The same brain processes that make negotiating the teen years so difficult make substance abuse more likely. An immature prefrontal cortex means less control over impulsive behavior, less understanding of the consequences, and fewer tools to stop the behavior. And an immature nucleus accumbens is also more active than an adult’s, and this means teens will almost automatically seek out high-risk, high-reward activities that take little effort and offer maximum bang for the buck.
The immediate dangers of taking drugs, the life-and-death consequences, are now well known. But the ramifications of a single bad decision or impulsive act are myriad and affect not only the families of the drug abusers but also everyone else around them—including, and especially, other adolescents. After Irma Perez, the California middle school student who died after swallowing a single tablet of Ecstasy, was laid to rest, four adolescents and a twenty-year-old had to face the consequences of giving her the drug and not getting her the medical assistance she needed in a timely fashion. Two eighth-grade girls pleaded guilty to furnishing a minor with a controlled substance and cruelty to a child that was likely to result in harm or death. They were forced to cooperate with the district attorney’s office during the prosecution of the three other defendants and attend an eight-month drug rehabilitation program for adolescent girls. The twenty-year-old man, Anthony Rivera, received a five-year prison sentence for providing the Ecstasy pills by selling them to seventeen-year-old Calin Fintzi, who in turn sold them to Irma’s two eighth-grade friends. Rivera also provided the marijuana he thought would help ease Irma’s painful reaction to the Ecstasy pill. And the fifth person, eighteen-year-old Angelique Malabey? She served six months in jail for helping Rivera hide the drugs after Irma’s death.
Please understand that there is biology making substances of abuse even more irresistible to the teenager than to an adult. We need to approach the substance-abusing teenager aggressively, and possibly with more empathy than we do an addicted adult. A teen still has the capacity to change, to recover, but only with very aggressive intervention. Even a “good” kid can get mixed up with the “wrong” kids and fall into the trap of substance abuse very easily. Hence, as parents and teachers, and even teen peers, we need to keep a very watchful eye on signs of drug abuse. Withdrawal, dramatic changes in appetite and sleeping habits, excess irritability, or lack of personal hygiene, among other things, should raise concern. Talk to other adults around the teen and check if they have observed the same thing. I hate to say it, but have a low threshold for suspicion. You will be doing your child a favor. If you have to play detective in a child’s room when he or she leaves for school, do it . . . for your child. If there is any evidence, you must call your pediatrician and describe what you are seeing. Addiction is a medical issue, not just “delinquent behavior”—addiction is a disease, and it can be treated. There are dozens of websites that will lead you and your teen to free care, and a good place to start if you have no other options would be the National Institute on Drug Abuse (www.drugabuse.gov). Most communities and towns have resources you can access. If you think there is something going on, you must make contact—you could be saving your child’s life down the road.